



Scuba diving can be practiced recreationally or professionally. In both modalities the diver can be exposed to risks such as decompression syndrome and thus, the use of a hyperbaric chamber, hyper-oxygenation of the gas cylinder, barotrauma, and immersion in closed circuits. These situations have some phenomena in common, such as the great pressure differences, which can cause a wide range of alterations, including ophthalmological ones. The development of index myopia and nuclear cataract are ocular findings frequently associated with increased oxygen pressure. In this context, an imbalance is established between oxidative species and antioxidant defences, such as glutathione, which has a key role in maintaining the transparency of the lens. The cases are presented of 2 young coral fisher patients, who had recently developed a progressive myopisation associated with nuclear cataracts.
El submarinismo puede practicarse de manera recreativa o profesional. En ambas modalidades el buceador puede verse expuesto a riesgos como el síndrome de descompresión y al consecuente uso de la cámara hiperbárica, la hiperoxigenación de la botella de gases, el barotrauma y la inmersión en circuitos cerrados. Estas situaciones tienen en común la exposición a una gran diferencia de presiones, lo que puede provocar una amplia gama de alteraciones, incluidas las oftalmológicas. El desarrollo de una miopía de índice y catarata de tipo nuclear son hallazgos oculares frecuentemente asociados al aumento de presión de oxígeno. En este contexto, se establece un desequilibrio entre especies oxidativas y defensas antioxidantes como el glutatión, que posee un papel clave en el mantenimiento de la transparencia del cristalino. Presentamos los casos de 2 pacientes jóvenes, pescadores de coral, que presentaron una miopización reciente y progresiva asociada a cataratas nucleares.
Diving consists in the practice of diving in the sea. In the last decades this sport has become very popular due to the increased supplies for recreational diving. Different medical alterations have been identified both in newcomers to the sport as in professionals who practice advanced levels of diving.
Multiple ocular alterations have been related to the practice of scuba diving. The most frequent mechanisms of production are barotrauma, hyperoxygenation, decompression syndrome and the use of hyperbaric chambers. The location of the lesions mainly compromises the head and neck in up to 60–80% of cases.1
The aim of this work is to present the cases of 2 middle-aged professional divers who came to our clinic with recent myopization Associated to nuclear-type cataracts. This refractive change could be related to a change in lens thickness secondary to the oxidative damage of lenticular nuclear proteins that occurs as a consequence of this activity.
Case 1A 50-year-old man who came to our office reporting bilateral and progressive visual acuity (VA) decrease in recent months. He denied any medical or ophthalmological history of interest and was not taking any medication on a regular basis. He had never worn glasses before. However, in recent years he referred the appearance of myopia that varied intermittently. The patient was a professional diver and attributed the worsening of his vision to the recent initiation of closed circuit diving at high oxygen pressure. According to him, several of his colleagues had recently experienced similar declines in VA. On examination, best corrected VA on a decimal scale was 0.6 in both eyes. With a refraction of −0.5D in the right eye and −0.75D in the left eye. In biometry, axial length was 23.26/23.17mm, mean keratometry 42.6/42.9 and LT 4.37/4,39mm. Examination of both the anterior and posterior segments was within normal ranges except for the finding in both eyes of nuclear N04 cataracts according to the LOCS III classification.
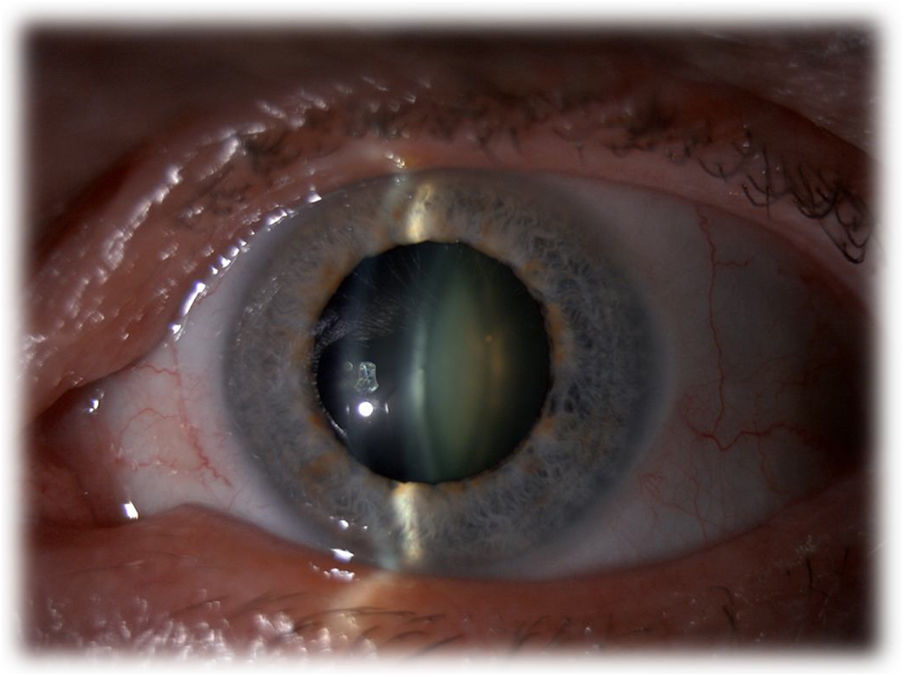
Case 2A 58year old man, who came due to progressive and sharp decreased AV in both eyes in recent years. He referred highly variable myopization since age 50. He had no relevant systemic or ophthalmological antecedents and did not take any regular medication. Best corrected AV was 0.3 in the right eye and 0.2 in the left eye. Refraction was −6.00 −1.00at 94° and −5.00 −0.75 at 100° respectively. At the time of the exploration, both the anterior and posterior segments were normal except for nuclear cataracts N04.2 according to LOCS III, bilateral and symmetrical (Fig. 1). In biometry the axial length was 24.21/24.02mm, mean keratometry 42.2/42.35 and LT 4.72/4.59mm.

Both patients used the hyperbaric chamber after each dive. Subsequently, phacoemulsification plus an intraocular lens implant of the “Extended Depth of Focus” type were performed, specifically Tecnis Simfony (Johnson and Johson Vision), without complications and with VA of one in both distant and near vision.
DiscussionWhile diving, the diver can be submitted to great differences of pressure, with the consequent appearance of medical and ophthalmological alterations. We present 2 cases of progressive myopia associated, supposedly, to the fast evolution of nuclear cataracts in young healthy patients who practice diving in a professional way.
Diving can be done in 2 ways; in apnea or with supporting equipment, which can be scuba or tank. It is important to take into account some basic concepts about the physics of diving to understand most of the ocular alterations that are triggered mainly by pressure changes. During the immersion, the diver is put under an absolute pressure comprising atmospheric pressure (Patm) and hydrostatic pressure (Ph). Patm corresponds to the weight of the air on the surface of the water, and Ph to the weight of the water on the diver. Patm is a constant to which Ph will be added as the diver descends. There are various laws that intervene in the physics of diving; one of the most important is Henry’s law, which establishes that the deeper the water, and therefore the greater the pressure, the more the gases that make up the air in the tank will be absorbed. The most abundant gases are nitrogen and oxygen, with nitrogen being the most dangerous because, if the diver does not compensate for the difference in pressure, he will suffer decompression sickness.2 During the descent, pressure increases and the nitrogen dissolves in blood, while during the ascent the nitrogen in liquid state passes to gaseous state.
Ocular alterations produced in divingBarotraumaBarotrauma is defined as physical damage produced by a difference in pressure between an area in contact with the body and the exterior gas or liquid.3 The “Mask Squeeze” is a type of facial barotrauma, which occurs when the diver is unable to compensate for the difference in pressure during the descent, as the pressure increases and the volume in the mask space decreases.4,5
There is a greater risk and severity of ocular barotrauma in the following situations; at greater descent, in carriers of masks with high inner volume or that do not cover the nose and in patients with glaucoma or previous ocular surgery. Severity varies from mild (subconjunctival hemorrhage and skin ecchymosis) to severe (orbital hemorrhage or emphysema). Barotrauma can cause an increase in intraocular pressure (IOP), which can oscillate during the dive according to the pressure of the bottle, the inhalation and exhalation exercised and the mask. It has been demonstrated that waterproof glasses that do not cover the nose produce an increase in IOP in a sustained manner over time, contrary to those that cover the nose and do not increase it.6 In our case, none of the 2 patients exhibited a history of barotrauma, probably because they had better equipment and technique.
Decompression syndromeThis syndrome is a gas embolism produced by a sudden decrease in absolute pressure during the ascent. It is potentially lethal. Arterial gas embolism is produced when the gas contained in the lungs expands and breaks the alveolar capillaries. Microbubbles of nitrogen enter the circulation and produce vascular occlusion at any level, including the retina and choroids. Injury is produced by the same obstruction but also by activation of the complement system and coagulation. However, in one study it was concluded that by taking safety measures the retinal alteration was not larger in divers compared to controls. On the other hand, it was found that those who performed decompressions often exhibited greater risk of retinal pigment epithelium alterations.7
Hyperbaric chamberIn this chamber, pure oxygen is administered at intervals, with an oxygen pressure higher than that existing at sea level. It was originally developed to treat decompression sickness, but today it is used to treat different hypoxia-related disorders. In addition, there are indications in ophthalmology such as occlusive vasculopathies. Benefits of the hyperbaric chamber include the increase of partial pressure of oxygen and the gradient of diffusion in tissues. This stimulates the proliferation of fibroblasts, collagen synthesis, capillary angiogenesis and peroxidase activity in ischemic tissue. However, it also exhibits adverse effects, since reactive species appear together with the increase of oxygen, producing greater oxidative stress on the tissues.
At the ocular level, oxidative stress will produce changes in lens proteins that generate molecular aggregates and abnormal reticulation thereof. These changes can alter the index and refractive power, thus generating the development of nuclear cataract and myopization. All of this can occur even when presenting normal LT, as in the case of our patients. The most important antioxidant in the lens is glutathione, which is responsible for maintaining transparency. It is found to a lesser extent in the nucleus, and that is why when a cataract appears due to hyperoxygenation it is usually the nuclear type.8 Ocular changes described in the literature due to the use of hyperbaric chambers are myopization, cataratogenesis, corneal endothelium thinning, lens epithelium damage, narrowing of retinal vessels and keratoconus.8 Most of these effects are rare and some are reversible and preventable.
Riedl et al. conducted a prospective cohort study in patients receiving hyperbaric oxygen therapy and found transient myopia in almost 90%, normalizing after 12 weeks of treatment.9 Evanger et al. compared refractive changes in 2 groups of patients, one receiving orofacial mask therapy and the other using an oxygen bell, and observed that the myopic change was of greater intensity and duration in the patients who received the bell treatment. These results agree with the fact that oxygen is responsible for the toxic effect, since with the bell more oxygen is received in the periocular area.10
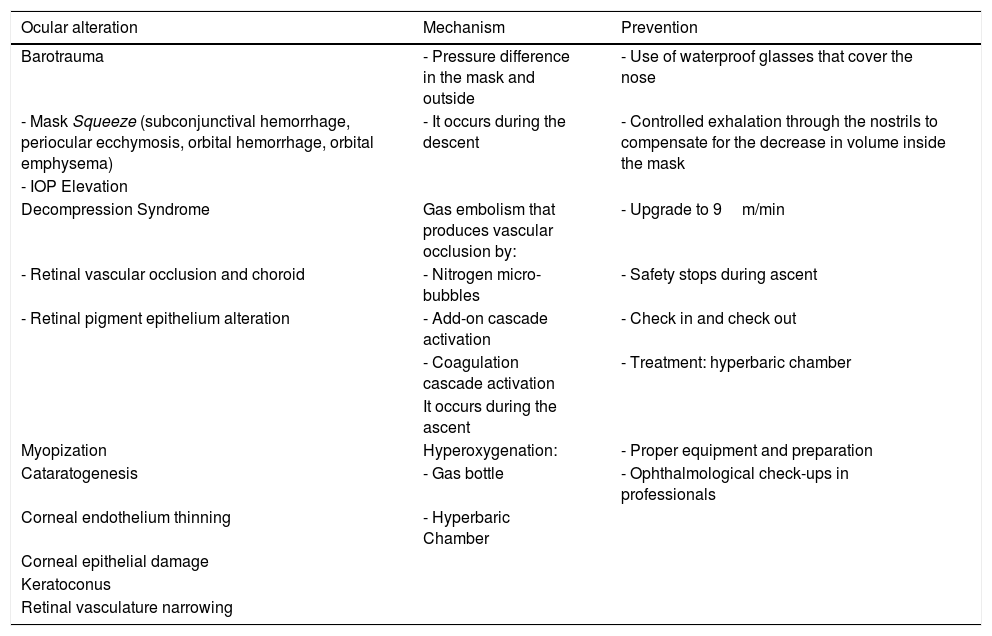
Table 1 shows different ocular alterations in divers, their mechanisms and forms of prevention.
Summary of eye disorders in divers: mechanism and prevention.
| Ocular alteration | Mechanism | Prevention |
|---|---|---|
| Barotrauma | - Pressure difference in the mask and outside | - Use of waterproof glasses that cover the nose |
| - Mask Squeeze (subconjunctival hemorrhage, periocular ecchymosis, orbital hemorrhage, orbital emphysema) | - It occurs during the descent | - Controlled exhalation through the nostrils to compensate for the decrease in volume inside the mask |
| - IOP Elevation | ||
| Decompression Syndrome | Gas embolism that produces vascular occlusion by: | - Upgrade to 9m/min |
| - Retinal vascular occlusion and choroid | - Nitrogen micro-bubbles | - Safety stops during ascent |
| - Retinal pigment epithelium alteration | - Add-on cascade activation | - Check in and check out |
| - Coagulation cascade activation | - Treatment: hyperbaric chamber | |
| It occurs during the ascent | ||
| Myopization | Hyperoxygenation: | - Proper equipment and preparation |
| Cataratogenesis | - Gas bottle | - Ophthalmological check-ups in professionals |
| Corneal endothelium thinning | - Hyperbaric Chamber | |
| Corneal epithelial damage | ||
| Keratoconus | ||
| Retinal vasculature narrowing | ||
The most frequent ocular alterations related to diving are hyperoxic myopia and the development of nuclear cataract. Both could be secondary to the hyperoxygenation of the gas cylinder, use of the hyperbaric chamber and activity in closed circuits. These patients usually preserve good VA after cataract surgery. We recommend regular ophthalmological checkups for people who regularly dive.
FinancingThis research has not received specific support from public sector agencies, commercial sector or non-profit entities.
Conflict of interestNone.
Please cite this article as: Marín-Martínez S, Rocha-de-Lossada C, Chang-Sotomayor M, Batlle-Ferrando S, Miguel L, Corretger X. Alteraciones oculares en submarinistas: Presentación de 2 casos clínicos y revisión de la literatura. Arch Soc Esp Oftalmol. 2021;96:102–105.
