




Mathematical algorithms 3D-reconstruction techniques and artificial intelligence are a current line of innovation in colorectal surgical oncology.
The objective of this study is to show the initial experience of a 3D image processing and reconstruction system to perform complete mesocolic excision and D3-lymphadenectomy in colon cancer.
It is applied to a splenic flexure neoplasm and in a right colon cancer with suspected retroperitoneal infiltration.
3D image processing and reconstruction was employed to delimit 10 cm proximal and distal intestinal margins to the tumor and define its corresponding vascularization. In right colon cancer it showed position and exact dimensions of D3-lymphadenectomy area and possible retroperitoneal fascia infiltration.
3D image processing and reconstruction allows to obtain valuable information from computerized tomography scan. It could be employed during surgical strategy planification to improve oncological results and reduce intraoperative complications.
Las técnicas de reconstrucción 3D basadas en algoritmos matemáticos y la inteligencia artificial son una línea de innovación actual en cirugía oncológica colorrectal.
El objetivo es mostrar la experiencia inicial de un sistema de procesamiento de imagen y reconstrucción 3D en la planificación de escisión completa de mesocolon y linfadenectomía D3 en cáncer de colon.
Se aplica en un caso de neoplasia de ángulo esplénico así como en neoplasia de colon derecho con sospecha de infiltración retroperitoneal.
Se empleó el procesamiento de imagen y reconstrucción 3D para delimitar un margen intestinal de 10 cm proximal y distal al tumor y delimitar la vascularización correspondiente a la tumoración. En el cáncer de colon derecho se mostró la posición y dimensiones exactas del área de linfadenectomía D3 y posible infiltración de la fascia retroperitoneal.
El procesamiento de imagen y reconstrucción 3D permite obtener información valiosa a partir de la tomografía computarizada. Esta podría emplearse en la estrategia quirúrgica y así mejorar los resultados oncológicos y disminuir las complicaciones intraoperatorias.
In recent years, we have witnessed an increase in publications about the application of 3D reconstruction technology in cancer surgery based on conventional imaging techniques1. These studies highlight the advantages of 3D reconstruction of the vascular supply using computed tomography (CT) scans to design the surgical strategy for central ligation or D3 lymphadenectomy in colon cancer2.
Recently, a 3D-image processing and reconstruction system (3D-IPR) based on mathematical algorithms has been used in locally advanced rectal cancer to assess tumor invasion of neighboring structures3.
The objective of this article is to show the first cases in which 3D-IPR has been used to plan complete excision of the mesocolon and D3 lymphadenectomy in colon cancer.
Surgical techniqueThe complete excision of the mesocolon shown is based on the following technical details: intestinal margins proximal and distal to the tumor of 8−10 cm, dissection by embryological plane and central ligation of the feeder vessels of the tumor. In addition, invasion-free surgical margins must be achieved4. The following two real clinical cases will show the usefulness of 3D-IPR for each of these points.
Splenic flexure colon cancerThree surgical techniques have been described for this type of tumors, finding no differences in the oncological results: segmental resection of the splenic flexure, subtotal colectomy and extended left hemicolectomy5.
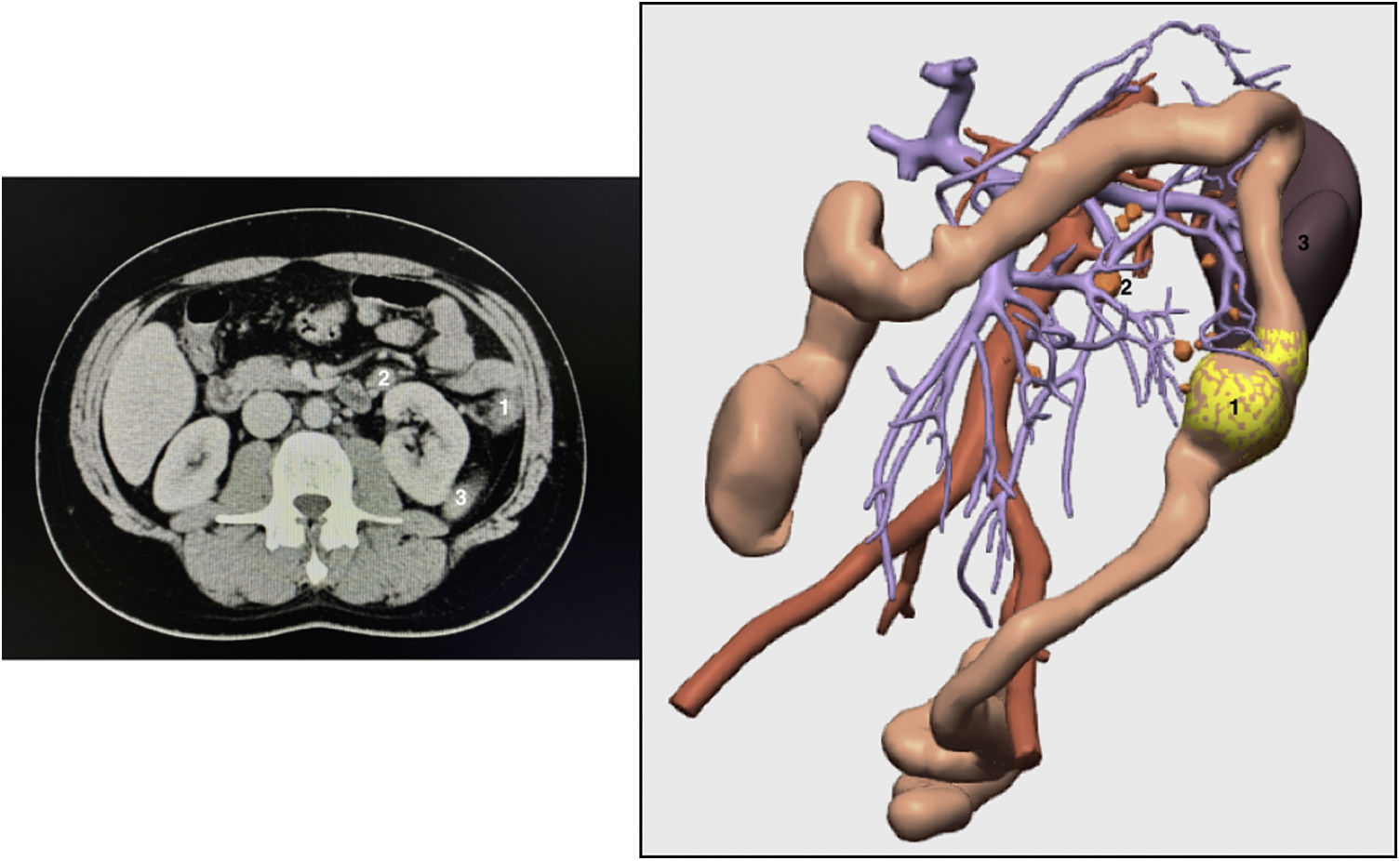
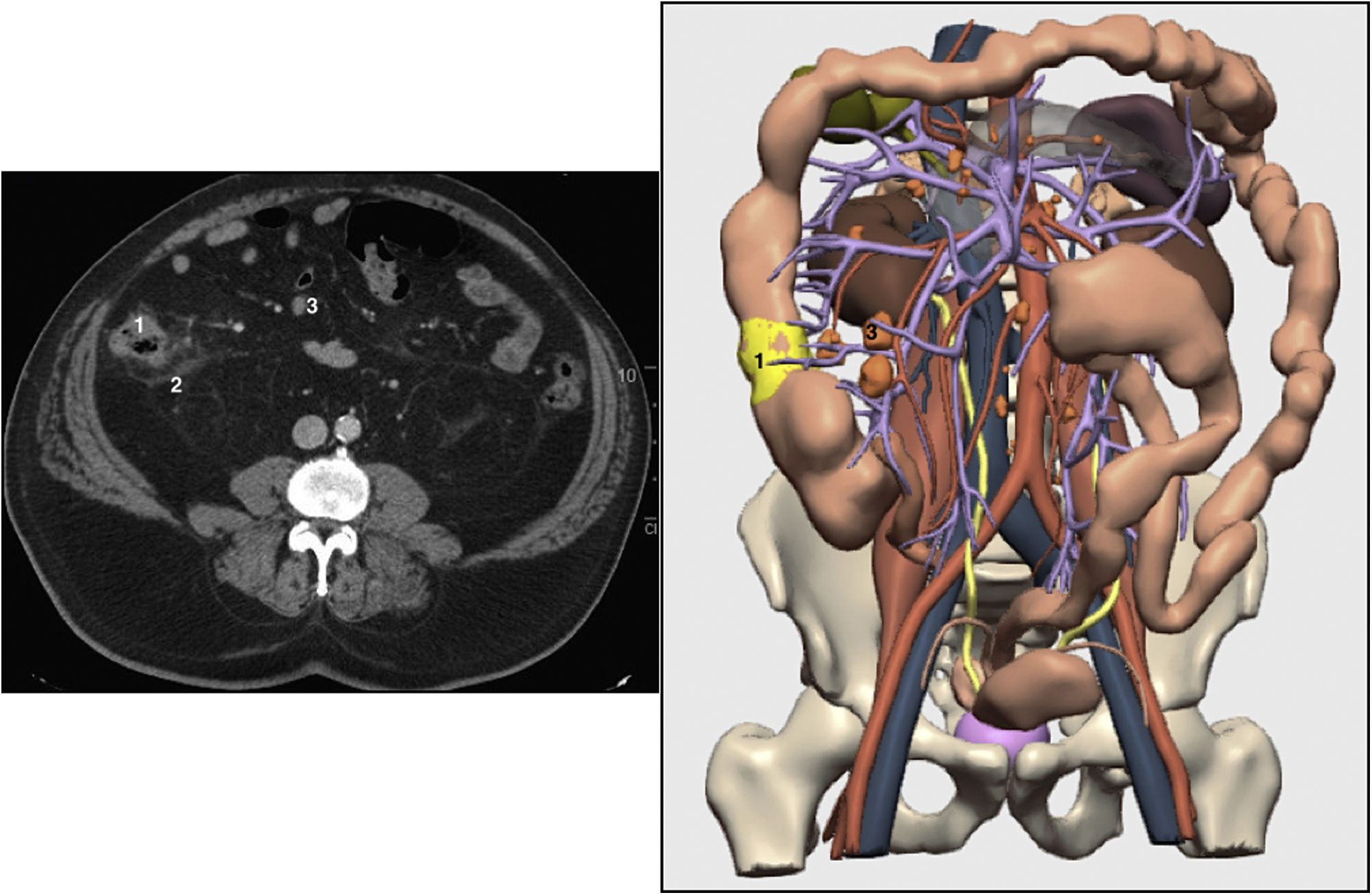
We present the case of a 42-year-old patient diagnosed with colon adenocarcinoma of the splenic flexure by colonoscopy and CT scan; preoperative stage T3N+M0 (Fig. 1). 3D-IPR was used to delimit the 10-cm intestinal margin and thus identify the feeder vessels of the tumor, which in this case was the left colic artery (Fig. 2A,B).
 Tumor; 2) Lymphadenopathy in the region of the inferior mesenteric vein; 3) Spleen.")
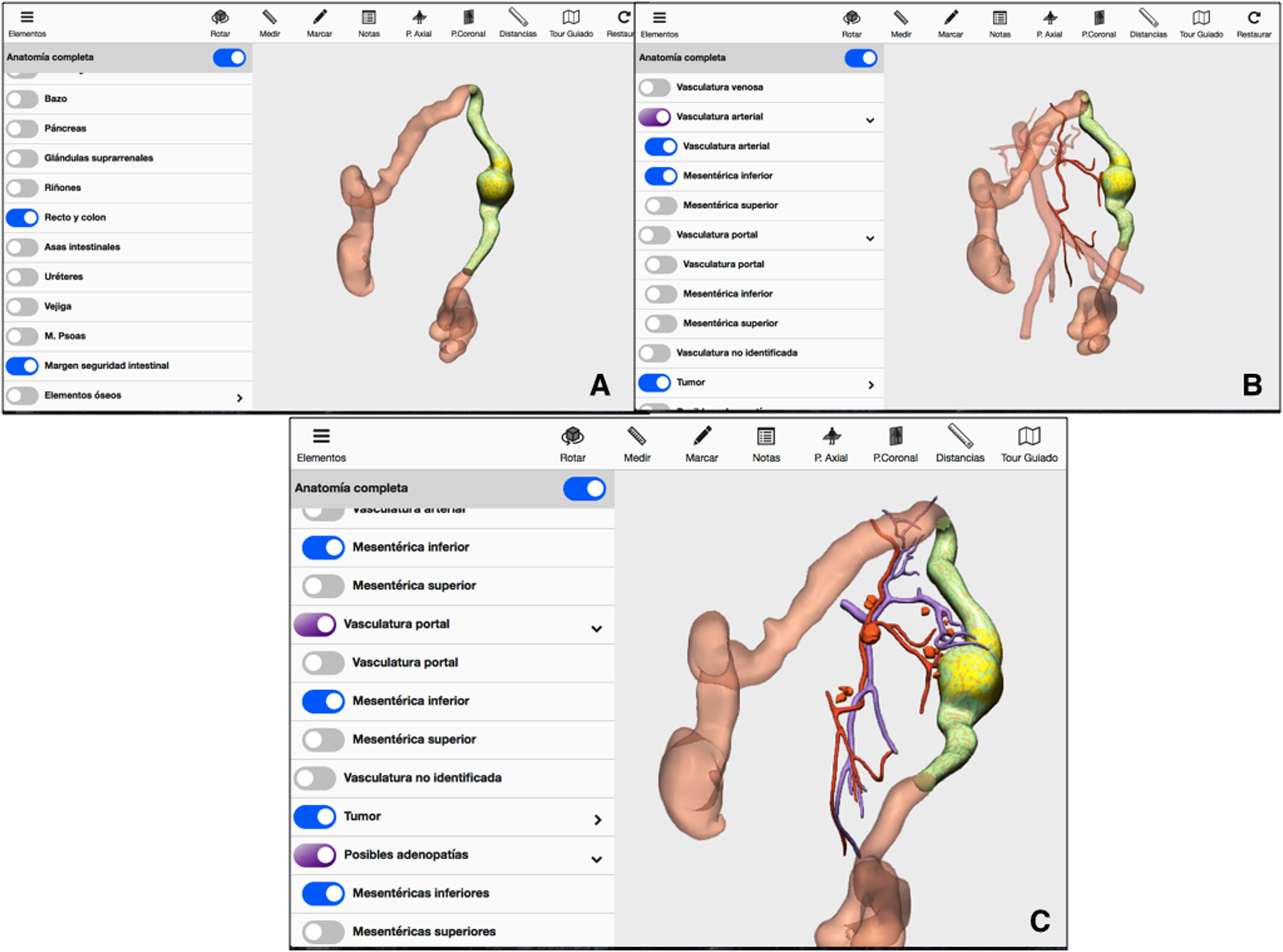
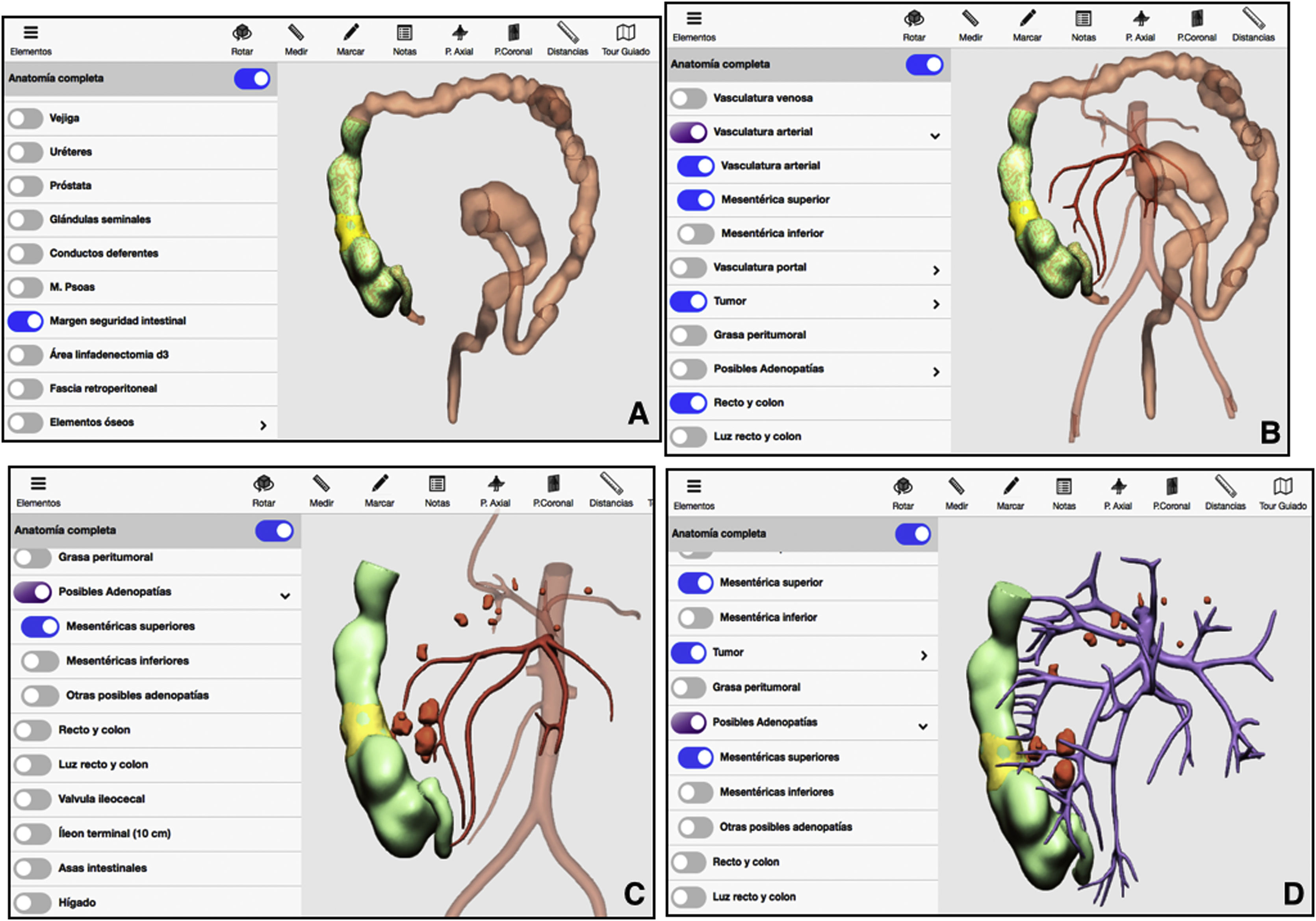
 Mathematical delimitation of the intestinal margin 10 cm proximal and distal to the tumor; B) Feeder vessels of the area established in A/C; Location of possible lymphadenopathies in the arterial and venous region of the area established in A.")
3D-IPR method used to establish surgical strategy in neoplasm of the splenic flexure: A) Mathematical delimitation of the intestinal margin 10 cm proximal and distal to the tumor; B) Feeder vessels of the area established in A/C; Location of possible lymphadenopathies in the arterial and venous region of the area established in A.
The 3D technique also located possible pericolic lymphadenopathies at the origin of the left colic artery and in the territory of the inferior mesenteric vein near the lower edge of the pancreas (Fig. 2C).
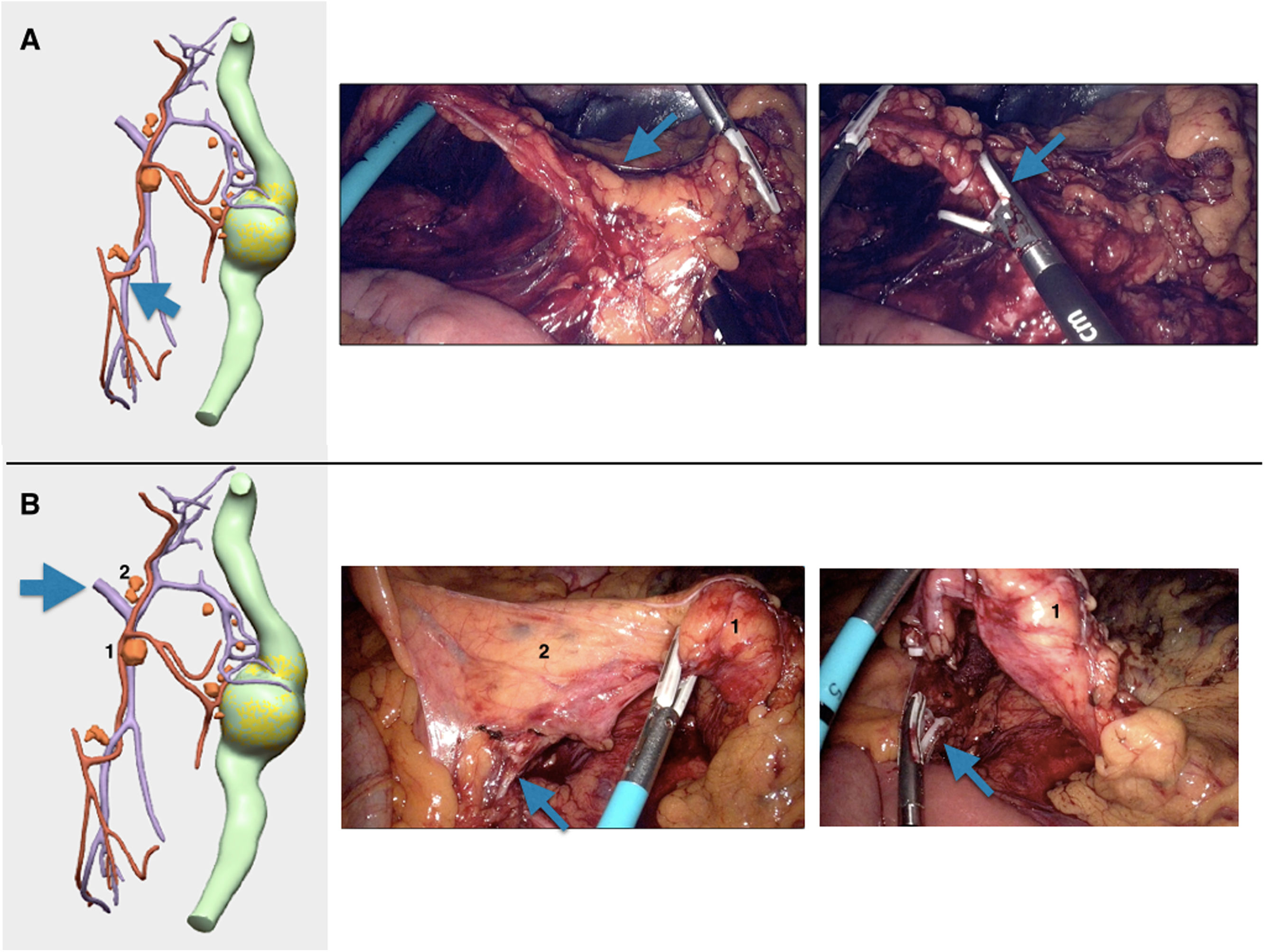
Due to all these findings, we performed laparoscopic segmental resection of the colon with central ligation of the left colic artery and the left branch of the middle colic vessels (Fig. 3A). The territory of the inferior mesenteric vein between the origin of the inferior mesenteric artery and its outlet in the splenic vein was also included (Fig. 3B).
 Blue arrow – high ligature of the left colic artery; B) Blue arrow – ligature of the inferior mesenteric vein at the lower edge of the pancreas; 1 and 2) possible lymphadenopathies in the region of the inferior mesenteric vein.")
Different surgical steps of the procedure, represented with 3D-IPR images and photos of the procedure: A) Blue arrow – high ligature of the left colic artery; B) Blue arrow – ligature of the inferior mesenteric vein at the lower edge of the pancreas; 1 and 2) possible lymphadenopathies in the region of the inferior mesenteric vein.
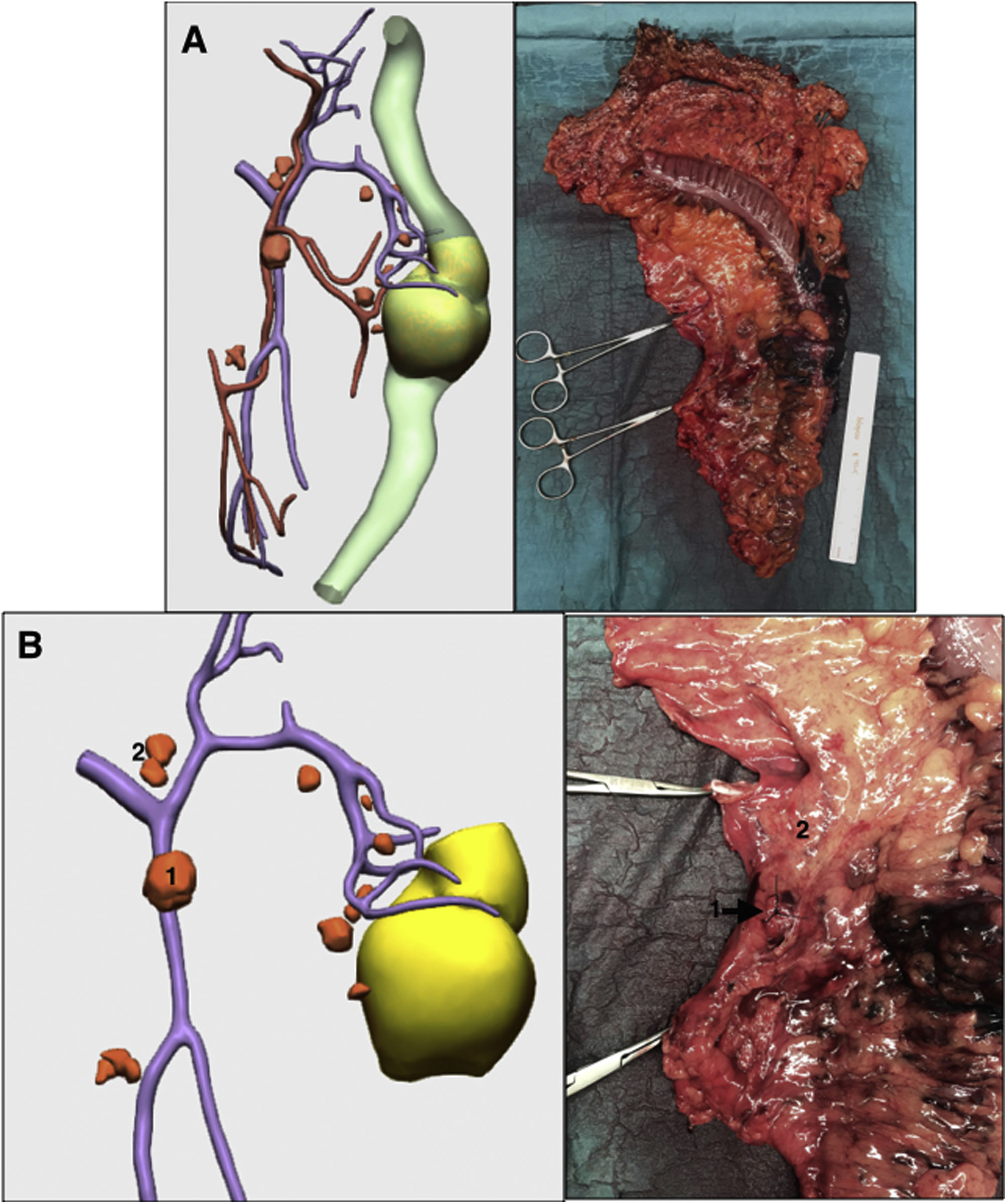
The pathological result was T3N1b(3/18). One of the 2 positive lymph nodes was located in the territory of the inferior mesenteric vein (Fig. 4A,B).
 Complete surgical specimen; B) Surgical specimen of the region of the inferior mesenteric vein; 1 and 2) Possible lymphadenopathies in the region of the inferior mesenteric vein. Surgical specimen is marked 1. The final study of the lymphadenopathy was positive for tumor invasion.")
Comparison of the surgical specimen simulated by 3D-IPR and actual surgical specimen: A) Complete surgical specimen; B) Surgical specimen of the region of the inferior mesenteric vein; 1 and 2) Possible lymphadenopathies in the region of the inferior mesenteric vein. Surgical specimen is marked 1. The final study of the lymphadenopathy was positive for tumor invasion.
According to the Japanese clinical guidelines, D3 lymphadenectomy in colon cancer is indicated in patients with suspected positive lymph nodes on the preoperative CT scan6.
Furthermore, if the retroperitoneal margin of the surgical specimen is positive for tumor invasion, the risk of local recurrence increases7.
We present the case of a 56-year-old patient diagnosed with adenocarcinoma located in the ascending colon by colonoscopy and CT scan (T4bN+M0). The radiological report suggested possible retroperitoneal fat invasion (Fig. 5).
 Tumor; 2) Possible invasion of retroperitoneal fat; 3) Possible lymphadenopathies.")
3D-IPR was used to delimit the 10 cm intestinal margin and thereby identify the feeder vessels, which in this case were the ileocolic artery and the right colic artery (Fig. 6A,B). Laparoscopic right hemicolectomy was performed with central ligation of the ileocolic vessels and right branch of the middle colic vessels. 3D-IPR located possible pericolic lymphadenopathies in the territory of the ileocolic vessels and close to the gastrocolic trunk of Henle (Fig. 6C,D).
 Mathematical delimitation of the intestinal margin 10 cm proximal and distal to the tumor; B) Feeder vessels of the area established in A; C) Location of possible lymphadenopathies in the arterial region of the area established in A; D) Location of possible lymphadenopathies in the venous territory of the area established in A.")
3D-IPR method used to establish surgical strategy in right colon cancer: A) Mathematical delimitation of the intestinal margin 10 cm proximal and distal to the tumor; B) Feeder vessels of the area established in A; C) Location of possible lymphadenopathies in the arterial region of the area established in A; D) Location of possible lymphadenopathies in the venous territory of the area established in A.
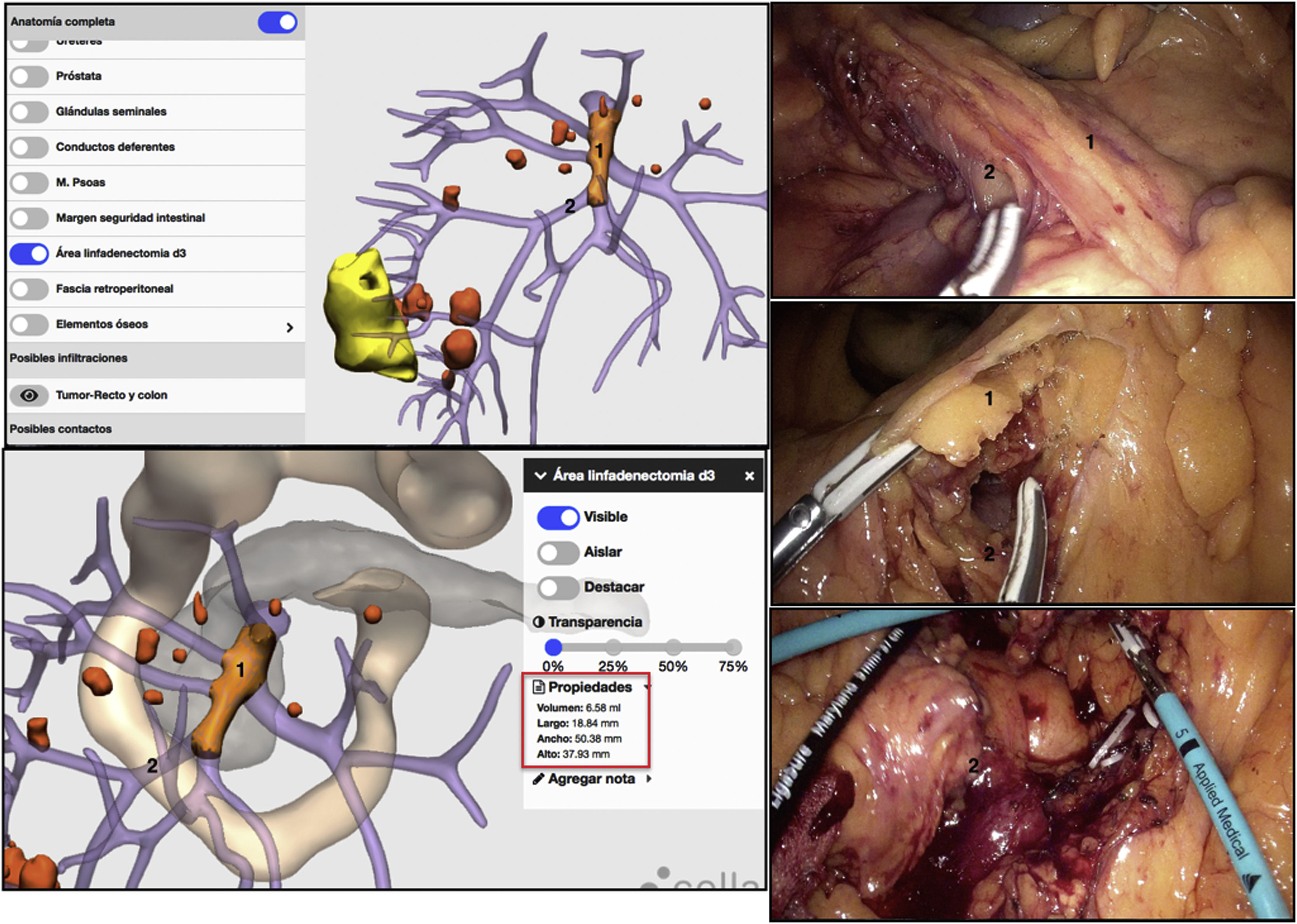
Using 3D-IPR, it was possible to locate the D3 lymphadenectomy area and calculate its volume mathematically. A D3 lymphadenectomy was performed with excision of the lymphatic-fatty tissue located on the superior mesenteric vein and high ligation of the right superior colic vein (Fig. 7).
 Area of the D3 lymphadenectomy; 2) Ileocolic vessels; Red square: dimensions of the volume, upper length and width of the D3 lymphadenectomy area.")
Different surgical steps of the D3 lymphadenectomy procedure, represented with 3D-IPR images and photos from the operation. The 3D-IPR image shows the mathematical identification of the dimensions of the D3 lymph node dissection area. The surgical photograms demonstrate the dissection of this area. 1) Area of the D3 lymphadenectomy; 2) Ileocolic vessels; Red square: dimensions of the volume, upper length and width of the D3 lymphadenectomy area.
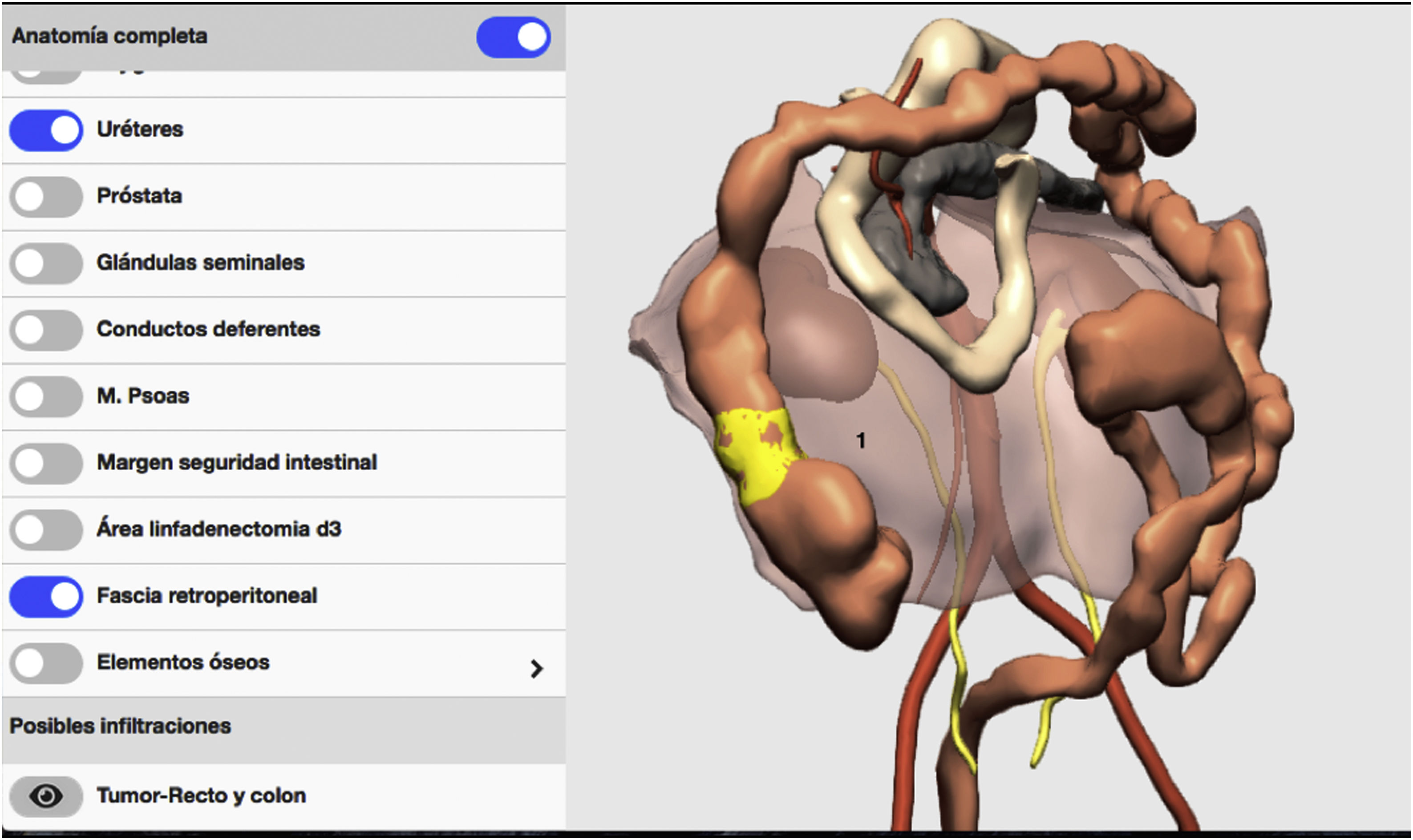
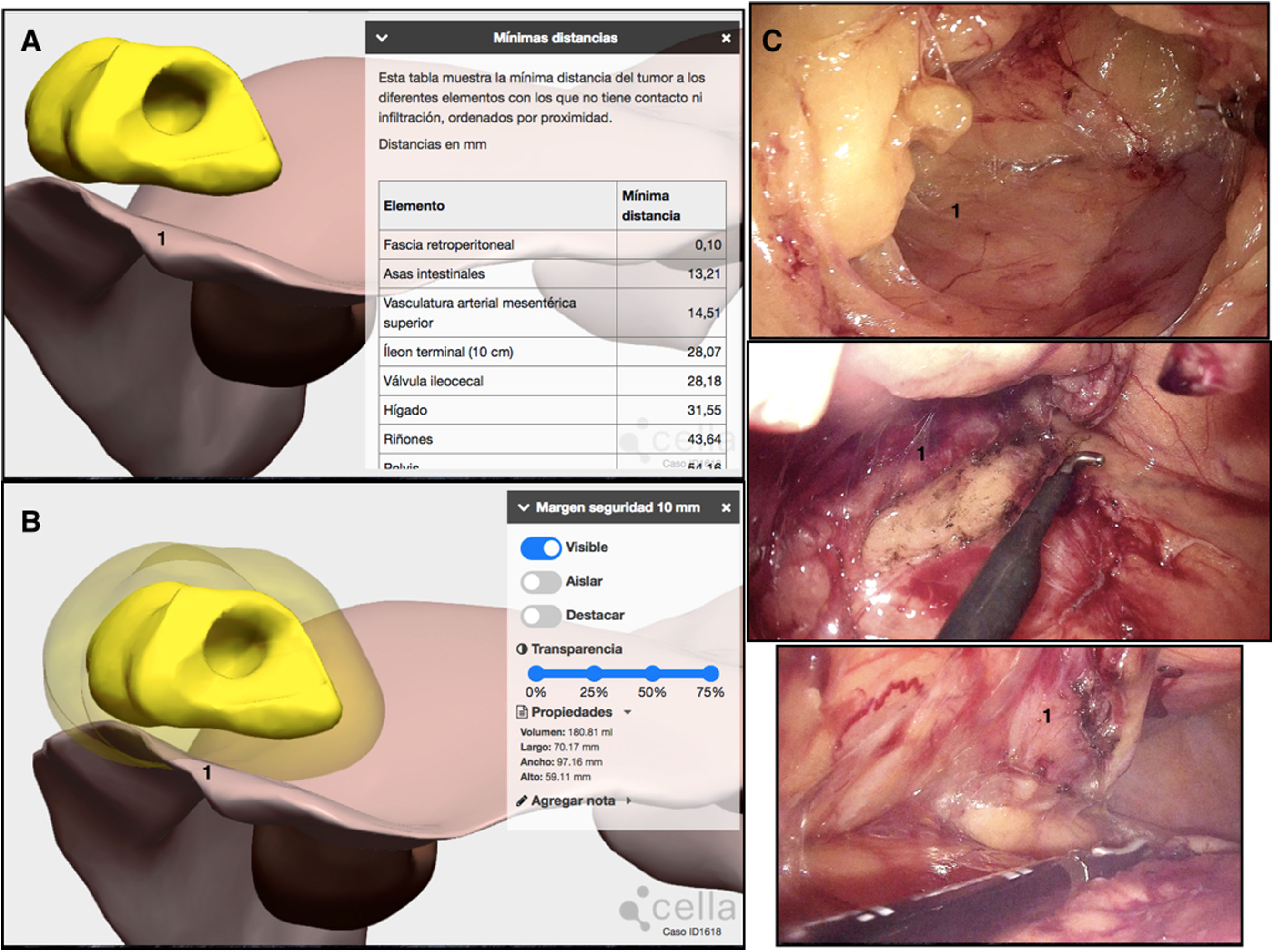
Lastly, given the suspected retroperitoneal fat invasion, a 3D reconstruction of the retroperitoneal fascia was performed (Fig. 8), and the minimum distance from the tumor to this fascia was measured. The result was 0.1 mm, so the conclusion was no retroperitoneal fat invasion (Fig. 9A). Even so, the surgical simulation using 3D-IPR showed that, to obtain a free surgical margin of 1 cm, the retroperitoneal fascia should be included in the surgical specimen (Fig. 9B). The embryonic dissection plane was Toldt’s and Fredet’s fascia, but the retroperitoneal fascia was included in the surgical piece in the area of possible tumor invasion (Fig. 9C).
 Retroperitoneal fascia.")
 Minimal distance obtained using 3D-IPR of the tumor to the retroperitoneal fascia: 0.1 mm; B) Simulation of the 1-cm invasion-free radial surgical margin that shows the need to incorporate the retroperitoneal fascia to the surgical piece; C) Incorporation of the retroperitoneal fascia in the surgical specimen; 1) Retroperitoneal fascia.")
3D-IPR method used to establish the relationship of the tumor with the retroperitoneal fascia and simulate and surgical specimen with a 1-cm invasion-free radial margin free. Demonstration of the surgery performed using photos: A) Minimal distance obtained using 3D-IPR of the tumor to the retroperitoneal fascia: 0.1 mm; B) Simulation of the 1-cm invasion-free radial surgical margin that shows the need to incorporate the retroperitoneal fascia to the surgical piece; C) Incorporation of the retroperitoneal fascia in the surgical specimen; 1) Retroperitoneal fascia.
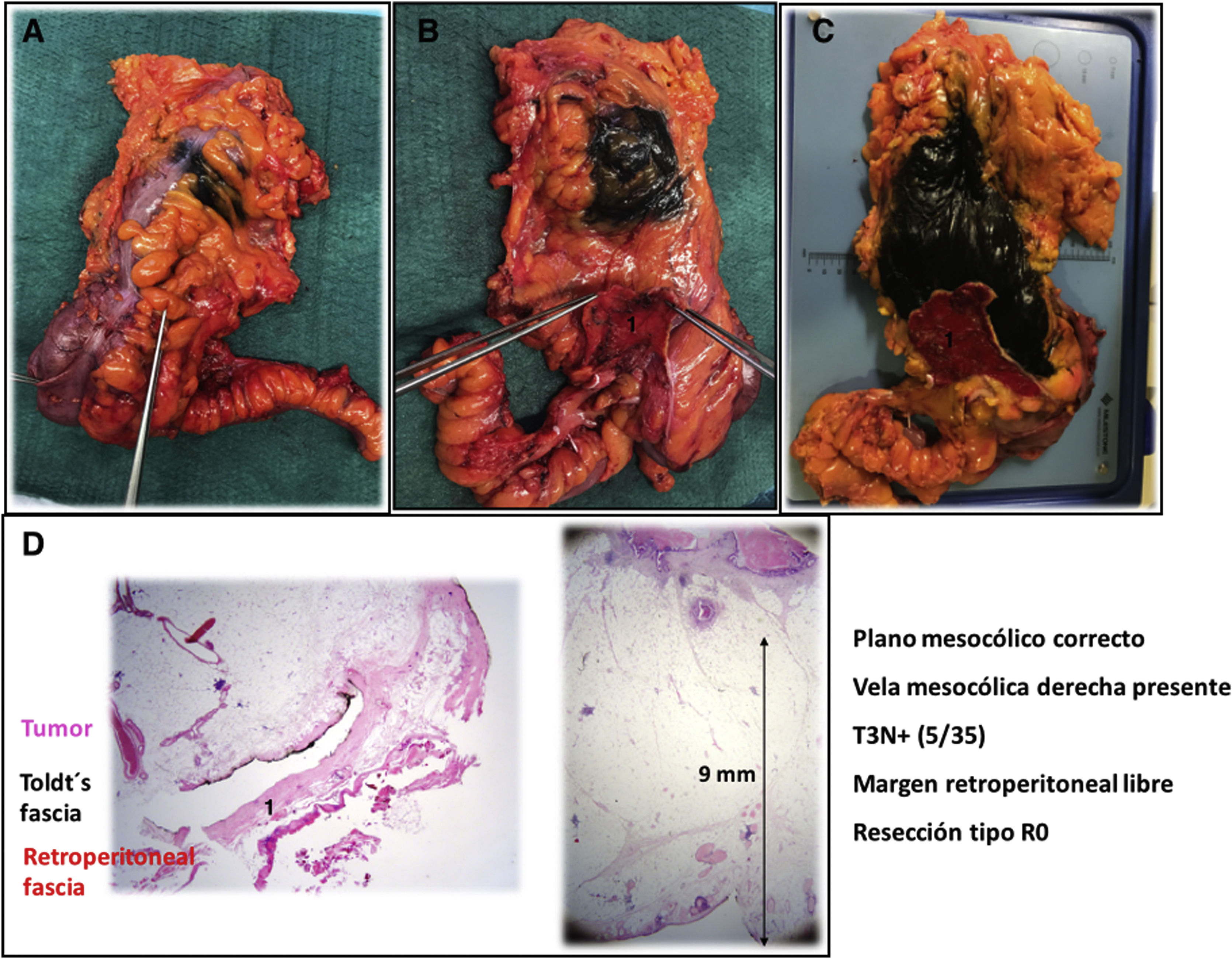
The macroscopic pathology report revealed a correct mesocolic plane, presence of the right mesocolic sail, confirming complete D3 lymphadenectomy (Fig. 10A–C). The microscopic pathology report was T3N+(5/35), negative retroperitoneal margin and a distance from the tumor to the retroperitoneal margin of 9 mm (Fig. 10D).
 Anterior view with tattoo of the tumor margin by endoscopy; B) Posterior view of the surgical specimen with retroperitoneal fascia indicated by the surgeon; C) Posterior view of the surgical specimen with retroperitoneal margin marked with black India ink and retroperitoneal fascia marked with red India ink; C) Microscopic vision of the relationship of the tumor with the retroperitoneal fascia and the tumor distance to the retroperitoneal margin; 1) Retroperitoneal fascia.")
Pathological study of the surgical specimen: A) Anterior view with tattoo of the tumor margin by endoscopy; B) Posterior view of the surgical specimen with retroperitoneal fascia indicated by the surgeon; C) Posterior view of the surgical specimen with retroperitoneal margin marked with black India ink and retroperitoneal fascia marked with red India ink; C) Microscopic vision of the relationship of the tumor with the retroperitoneal fascia and the tumor distance to the retroperitoneal margin; 1) Retroperitoneal fascia.
Diagnostic imaging studies (CT) are used in DICOM format. Images are fused between the phases of the CT, applying rigid co-registration techniques (related and unrelated), to correct deviations derived from movement, breathing, or patient position. The image is normalized and prepared with anisotropic diffusion filters for noise removal. The semiautomatic segmentation of anatomical elements of interest is performed based on the result of the execution of SesRegNet and UnetR type neural networks, followed by algorithms for adaptive region growing. The effect of slice thickness on the resulting 3D structures is attenuated by Laplacian smoothing. Boolean operators are used to determine the invasions or contacts of the pathological elements with other organs.
DiscussionThe preoperative surgical strategy based on imaging tests decreases the risk of intraoperative complications and improves oncological results2. Complete excision of the mesocolon is based on the central ligation of the feeder vessels of the tumor4. Tumors located in the splenic flexure range from those located in the distal part of the transverse colon to the proximal part of the descending colon. This variability causes 3 surgical techniques to be considered correct: subtotal colectomy, left hemicolectomy and segmental resection of the splenic flexure5. The choice of the technique type will depend on the feeder vessels; however, sometimes the 2D visualization of CT images is not enough to identify them. This difficulty could be resolved with 3-dimensional reconstruction and a mathematical calculation of a 10-cm intestinal margin proximal and distal to the tumor. This margin gives a 95% probability that all the pericolic lymph nodes involved by the tumor will be resected8.
In tumors located in the splenic flexure, there is a bibliographic discussion as to whether it is necessary to routinely include the inferior mesenteric vein. What does seem evident is that it should be included when there are lymph nodes suspected of invasion in said territory9. 3D-IPR could help locate these lymphadenopathies preoperatively.
In right colon cancer, recent meta-analyses conclude that tumors classified as stage III benefit from implementing a D3 lymphadenectomy to complete excision of the mesocolon10. This technique is based on the inclusion in the surgical specimen of the lympho-fatty tissue located on the superior mesenteric vein and in the area of the gastrocolic trunk of Henle11. These structures show great anatomical variety, and their visualization in the preoperative CT scan is usually complicated. For this reason, different publications have shown the advantage of creating 3D reconstructions of the vascularization from CT scans2. 3D-IPR has the ability to detect the location and volume of the D3 lymphadenectomy area in right colon cancer.
Complete excision of the mesocolon is based on dissection along the embryological plane between the mesocolon and the retroperitoneum. In the right colon, it is performed along Toldt’s and Fredet’s coalescence fascia12. However, in the case of suspected invasion of retroperitoneal structures, the dissection plane must be modified, and these structures incorporated into the surgical piece, either partially or completely. The reason is that a retroperitoneal margin that is positive for tumor invasion increases the risk of local recurrence and lowers overall and disease-free survival7.
3D-IPR allows us to calculate the minimum distance from the tumor to all anatomical structures. In addition, it shows that the retroperitoneal fascia is an independent anatomical structure, so this 3D model can identify whether there is invasion or not.
Recently, 3D-IPR has also been applied with the same methodology using magnetic resonance imaging to identify tumor invasion of neighboring structures in locally advanced rectal cancer13.
Lastly, 3D-IPR provides surgical simulation of a 1-cm free surgical tumor margin, suggesting which anatomical structures should be resected en bloc next to the tumor. This safety perimeter would be equivalent to the radial margin in colon tumors staged preoperatively as T4b14. In tumors located in the right colon, due to the partially retroperitoneal anatomical situation of the ascending colon, it would also be equivalent to the retroperitoneal margin.
In conclusion, the ability to extract the maximum information from the CT study using 3-dimensional virtual reconstruction based on mathematical methods and artificial intelligence could help improve oncological outcomes in colon cancer and reduce intraoperative complications.
Conflict of interestsGarcia-Granero A: Royalties for intellectual property and consulting fees for consulting from Cella Medical Solutions, PRIM.
