




This article analyses the burden of disease in adolescents and young people in Spain in 2008.
Materials and methodsA cross-sectional population-based study. We estimated disability-adjusted life years (DALYs) by sex and cause for subjects aged 15-29 years. Data sources were used: (1) National death records by age, sex and cause; (2) population data (both in July 2008); and (3) estimates of the disability pattern for European countries with very low mortality.
ResultsIn 2008, adolescents and young people lost 786,479 DALYs (414,346 in males). Non-communicable diseases generated 661,282 DALYs (84% of the total). The main specific causes of disease burden were: unipolar depression (16% of DALYs), alcohol use disorders (11%), migraine (9%), bipolar disorder (7%), schizophrenia (6%), road traffic accidents (5%) and drug addiction disorders (5%).
ConclusionsThe burden of disease expressed in DALYs can define the loss of health in adolescents and young people. At these ages, health promotion and protection are essential to prevent the onset of disease in adulthood.
Se analiza la carga de enfermedad de los adolescentes y jóvenes en España en el año 2008.
Material y métodosEstudio transversal de base poblacional. Se estiman los años de vida ajustados por discapacidad (AVAD) por sexo y causa específica en personas de 15-29 años. Las fuentes de información fueron: 1) Defunciones por edad, sexo y causa; 2) Estimaciones de la población a julio de 2008; y 3) Estimaciones del patrón de discapacidad para países europeos con baja mortalidad.
ResultadosEn 2008, los adolescentes y jóvenes perdieron 786.479 AVAD (414.346 en varones). Las enfermedades no transmisibles causaron 661.282 AVAD (84% respecto al total). Las principales causas específicas de carga de enfermedad fueron: depresión (16% de AVAD), abuso de alcohol (11%), migrañas (9%), trastorno bipolar (7%), esquizofrenia (6%), accidentes de circulación (5%) y adicción a drogas (5%).
ConclusionesLa carga de enfermedad expresada en AVAD permite definir las pérdidas de salud en adolescentes y jóvenes. A estas edades, la promoción y protección de la salud son fundamentales, para prevenir la aparición de enfermedades en el adulto.
In Spain, the adolescents and young people aged 15-29 years old represent 20% of the population.1 Although most adolescents and young people are healthy globally,2 over 3,400,000 annual deaths are estimated in the world population of those between 15 and 29 years old.3 In addition, a significant number of young people suffer diseases that cause losses in human capital with accumulative long-term socioeconomic costs or adopt behaviours that put their health at risk.2 In fact, almost 2/3 of premature deaths and 1/3 of the world-wide burden of adult disease are associated with diseases or behaviours that began in the adults’ youth.2,3
Among public policies, health is one of the priorities in actions on youth and childhood.4 However, national studies that have attempted to specifically estimate the importance of the various health problems in this group are rare.
Study on the burden of disease makes it possible to measure and compare the magnitude of health losses from different causes, considering their deadly and non-deadly consequences together.5,6 The key, most used indicator in burden of disease studies are the disability-adjusted life years (DALY), which have been employed to guide debates on establishing health priorities.6
The objective of this study was to analyse the burden of disease for the adolescents and young people in Spain in 2008, calculating the DALY by gender and disease cause.
Material and methodStudy typeThis was a transversal study of a population base. The object of study was the population of 15- to 29-year olds resident in Spain in 2008.
Calculation methodWe followed the methodology proposed in the study on world burden of disease from the World Health Organisation (WHO),5 the main reference for studies on calculating DALYs. The DALY consist of the sum of the years of life lost from premature death (YLL) and the years lived with disability and poor health (YLD).3,5 The YLL were calculated by estimating the loss of years due to premature death by gender, age and cause as the difference between the age at death and the expected lifespan for that age defined according to a model life table of high life expectancy (Princeton Level West 26 modified).5 The YLD were calculated indirectly, applying to the YLL obtained YLL/YLD ratio by gender, age and cause calculated from the values estimated for the set of European countries with high life span and low mortality, which includes Spain.3 We also applied social assessments with a discount rate (3%) and weighted by age (factor K=1).5
Information sourcesPopulation data came from our National Statistics Institute (INE in Spanish), based on the current population estimates on 1 July 2008, yielding 8,645,287 people aged from 15 to 29 years.1 Deaths by sex and cause were taken from the anonymised file of the INE's individual records. Information on disability or poor health came from estimations for the 15-29 year old population in European countries with low mortality from the WHO study on global burden of disease.3
Statistical analysisWe performed a descriptive analysis, calculating DALY by sex and cause expressed in absolute (total numbers) and relative (rates per 100,000 inhabitants and proportions) values. The GesMor and Epidat 4.0 programs were used.
ResultsIn 2008, a burden of disease for the population of adolescents and young people is estimated as equivalent to 786,479 DALY (16.0% of the total for the Spanish population). By sex, 52.7% of the DALY corresponds to males. The global DALY rate is 9097.2 per 100,000 inhabitants 15-29 years old.
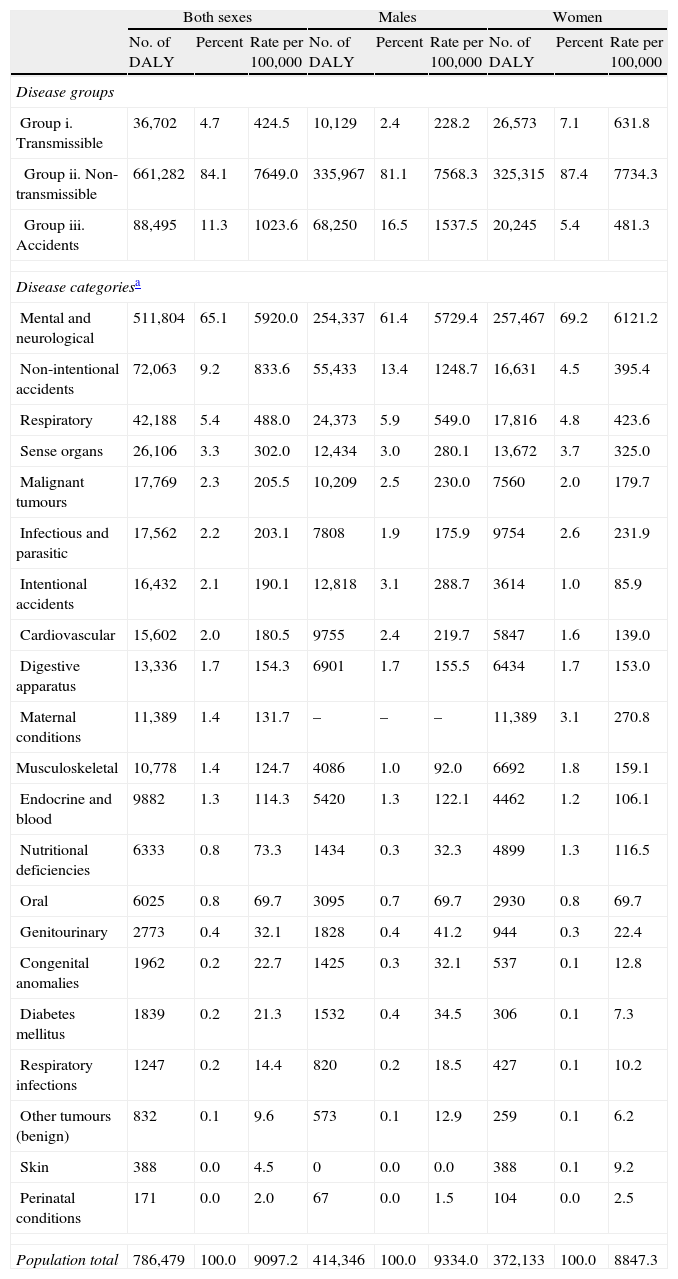
In Table 1, you can see the burden of disease by sex, groups and disease categories. Non-transmissible diseases represent 84.1% of the total DALY. Mental and neurological diseases are the main cause by number of DALY (511,804), with higher rates for women than for men (6121.2 and 5729.4 per 100,000, respectively). Next are non-intentional accidents (72,063 DALY), respiratory diseases (42,188 DALY) and sense organ diseases (26,106 DALY).
Burden of disease in adolescents and young adults (aged 15-29 years) by sex, disease group and disease category. Spain, 2008.
| Both sexes | Males | Women | |||||||
| No. of DALY | Percent | Rate per 100,000 | No. of DALY | Percent | Rate per 100,000 | No. of DALY | Percent | Rate per 100,000 | |
| Disease groups | |||||||||
| Group i. Transmissible | 36,702 | 4.7 | 424.5 | 10,129 | 2.4 | 228.2 | 26,573 | 7.1 | 631.8 |
| Group ii. Non-transmissible | 661,282 | 84.1 | 7649.0 | 335,967 | 81.1 | 7568.3 | 325,315 | 87.4 | 7734.3 |
| Group iii. Accidents | 88,495 | 11.3 | 1023.6 | 68,250 | 16.5 | 1537.5 | 20,245 | 5.4 | 481.3 |
| Disease categoriesa | |||||||||
| Mental and neurological | 511,804 | 65.1 | 5920.0 | 254,337 | 61.4 | 5729.4 | 257,467 | 69.2 | 6121.2 |
| Non-intentional accidents | 72,063 | 9.2 | 833.6 | 55,433 | 13.4 | 1248.7 | 16,631 | 4.5 | 395.4 |
| Respiratory | 42,188 | 5.4 | 488.0 | 24,373 | 5.9 | 549.0 | 17,816 | 4.8 | 423.6 |
| Sense organs | 26,106 | 3.3 | 302.0 | 12,434 | 3.0 | 280.1 | 13,672 | 3.7 | 325.0 |
| Malignant tumours | 17,769 | 2.3 | 205.5 | 10,209 | 2.5 | 230.0 | 7560 | 2.0 | 179.7 |
| Infectious and parasitic | 17,562 | 2.2 | 203.1 | 7808 | 1.9 | 175.9 | 9754 | 2.6 | 231.9 |
| Intentional accidents | 16,432 | 2.1 | 190.1 | 12,818 | 3.1 | 288.7 | 3614 | 1.0 | 85.9 |
| Cardiovascular | 15,602 | 2.0 | 180.5 | 9755 | 2.4 | 219.7 | 5847 | 1.6 | 139.0 |
| Digestive apparatus | 13,336 | 1.7 | 154.3 | 6901 | 1.7 | 155.5 | 6434 | 1.7 | 153.0 |
| Maternal conditions | 11,389 | 1.4 | 131.7 | – | – | – | 11,389 | 3.1 | 270.8 |
| Musculoskeletal | 10,778 | 1.4 | 124.7 | 4086 | 1.0 | 92.0 | 6692 | 1.8 | 159.1 |
| Endocrine and blood | 9882 | 1.3 | 114.3 | 5420 | 1.3 | 122.1 | 4462 | 1.2 | 106.1 |
| Nutritional deficiencies | 6333 | 0.8 | 73.3 | 1434 | 0.3 | 32.3 | 4899 | 1.3 | 116.5 |
| Oral | 6025 | 0.8 | 69.7 | 3095 | 0.7 | 69.7 | 2930 | 0.8 | 69.7 |
| Genitourinary | 2773 | 0.4 | 32.1 | 1828 | 0.4 | 41.2 | 944 | 0.3 | 22.4 |
| Congenital anomalies | 1962 | 0.2 | 22.7 | 1425 | 0.3 | 32.1 | 537 | 0.1 | 12.8 |
| Diabetes mellitus | 1839 | 0.2 | 21.3 | 1532 | 0.4 | 34.5 | 306 | 0.1 | 7.3 |
| Respiratory infections | 1247 | 0.2 | 14.4 | 820 | 0.2 | 18.5 | 427 | 0.1 | 10.2 |
| Other tumours (benign) | 832 | 0.1 | 9.6 | 573 | 0.1 | 12.9 | 259 | 0.1 | 6.2 |
| Skin | 388 | 0.0 | 4.5 | 0 | 0.0 | 0.0 | 388 | 0.1 | 9.2 |
| Perinatal conditions | 171 | 0.0 | 2.0 | 67 | 0.0 | 1.5 | 104 | 0.0 | 2.5 |
| Population total | 786,479 | 100.0 | 9097.2 | 414,346 | 100.0 | 9334.0 | 372,133 | 100.0 | 8847.3 |
DALY: disability-adjusted life years. Note: Some percent sums may not add up to 100% due to decimal rounding.
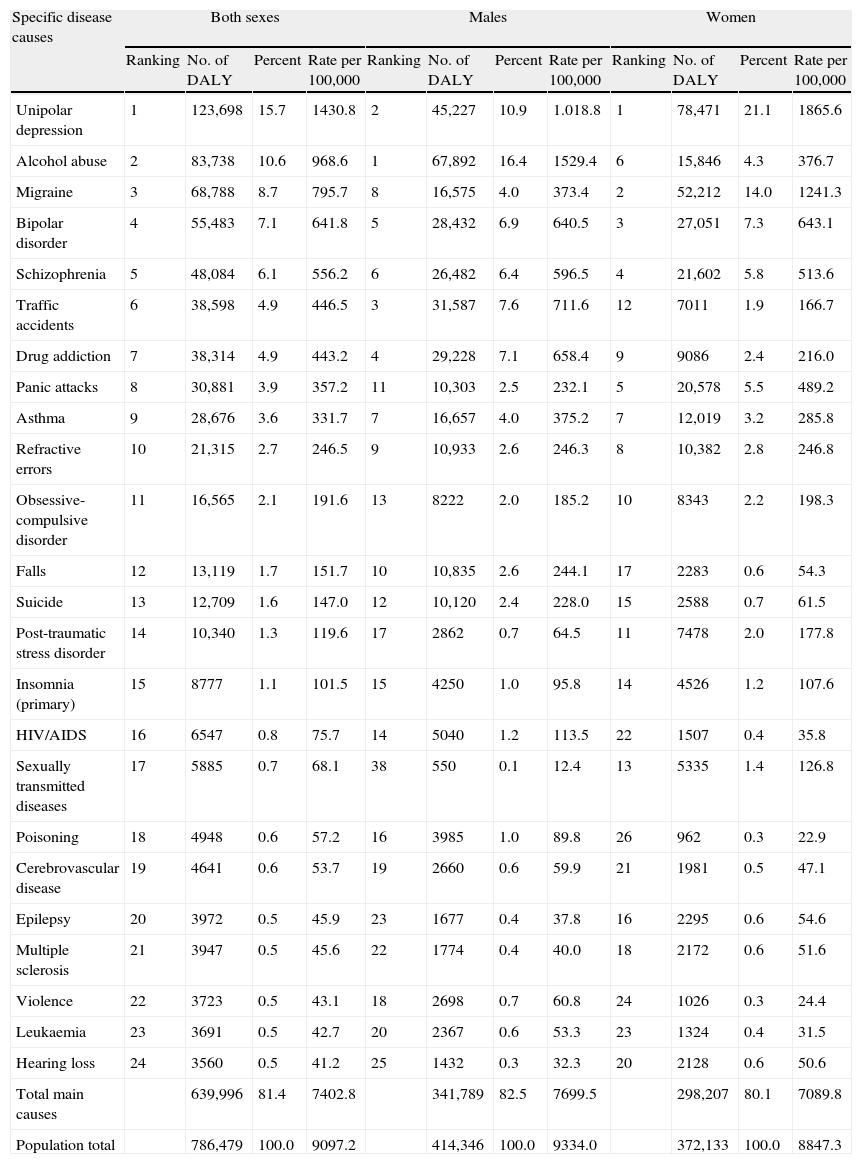
The main specific causes of burden of disease by sex can be seen in Table 2. In adolescents and young people (both sexes), depression (15.7% of the total DALY) is the leading cause of burden of disease, followed by alcohol abuse (10.6%), migraine (8.7%), bipolar disorder (7.1%), schizophrenia (6.1%), traffic accidents (4.9%) and drug addiction (4.9%). The ranking for disease causes varied according to gender (Table 2). In the males, alcohol abuse was the leading cause (16.4% DALY), ahead of depression (10.9%), traffic accidents (7.6%), drug addiction (7.1%), bipolar disorder (6.9%), schizophrenia (6.4%) and asthma (4.0%). Among the females, depression continues as the main cause by number of DALY (21.1%), followed by migraine (14.0%), bipolar disorder (7.3%), schizophrenia (5.8%), panic attacks (5.5%), alcohol abuse (4.3%) and asthma (3.2%) (Table 2).
Burden of disease in adolescents and young adults (aged 15-29 years) by sex and main specific disease causes. Spain, 2008.
| Specific disease causes | Both sexes | Males | Women | |||||||||
| Ranking | No. of DALY | Percent | Rate per 100,000 | Ranking | No. of DALY | Percent | Rate per 100,000 | Ranking | No. of DALY | Percent | Rate per 100,000 | |
| Unipolar depression | 1 | 123,698 | 15.7 | 1430.8 | 2 | 45,227 | 10.9 | 1.018.8 | 1 | 78,471 | 21.1 | 1865.6 |
| Alcohol abuse | 2 | 83,738 | 10.6 | 968.6 | 1 | 67,892 | 16.4 | 1529.4 | 6 | 15,846 | 4.3 | 376.7 |
| Migraine | 3 | 68,788 | 8.7 | 795.7 | 8 | 16,575 | 4.0 | 373.4 | 2 | 52,212 | 14.0 | 1241.3 |
| Bipolar disorder | 4 | 55,483 | 7.1 | 641.8 | 5 | 28,432 | 6.9 | 640.5 | 3 | 27,051 | 7.3 | 643.1 |
| Schizophrenia | 5 | 48,084 | 6.1 | 556.2 | 6 | 26,482 | 6.4 | 596.5 | 4 | 21,602 | 5.8 | 513.6 |
| Traffic accidents | 6 | 38,598 | 4.9 | 446.5 | 3 | 31,587 | 7.6 | 711.6 | 12 | 7011 | 1.9 | 166.7 |
| Drug addiction | 7 | 38,314 | 4.9 | 443.2 | 4 | 29,228 | 7.1 | 658.4 | 9 | 9086 | 2.4 | 216.0 |
| Panic attacks | 8 | 30,881 | 3.9 | 357.2 | 11 | 10,303 | 2.5 | 232.1 | 5 | 20,578 | 5.5 | 489.2 |
| Asthma | 9 | 28,676 | 3.6 | 331.7 | 7 | 16,657 | 4.0 | 375.2 | 7 | 12,019 | 3.2 | 285.8 |
| Refractive errors | 10 | 21,315 | 2.7 | 246.5 | 9 | 10,933 | 2.6 | 246.3 | 8 | 10,382 | 2.8 | 246.8 |
| Obsessive-compulsive disorder | 11 | 16,565 | 2.1 | 191.6 | 13 | 8222 | 2.0 | 185.2 | 10 | 8343 | 2.2 | 198.3 |
| Falls | 12 | 13,119 | 1.7 | 151.7 | 10 | 10,835 | 2.6 | 244.1 | 17 | 2283 | 0.6 | 54.3 |
| Suicide | 13 | 12,709 | 1.6 | 147.0 | 12 | 10,120 | 2.4 | 228.0 | 15 | 2588 | 0.7 | 61.5 |
| Post-traumatic stress disorder | 14 | 10,340 | 1.3 | 119.6 | 17 | 2862 | 0.7 | 64.5 | 11 | 7478 | 2.0 | 177.8 |
| Insomnia (primary) | 15 | 8777 | 1.1 | 101.5 | 15 | 4250 | 1.0 | 95.8 | 14 | 4526 | 1.2 | 107.6 |
| HIV/AIDS | 16 | 6547 | 0.8 | 75.7 | 14 | 5040 | 1.2 | 113.5 | 22 | 1507 | 0.4 | 35.8 |
| Sexually transmitted diseases | 17 | 5885 | 0.7 | 68.1 | 38 | 550 | 0.1 | 12.4 | 13 | 5335 | 1.4 | 126.8 |
| Poisoning | 18 | 4948 | 0.6 | 57.2 | 16 | 3985 | 1.0 | 89.8 | 26 | 962 | 0.3 | 22.9 |
| Cerebrovascular disease | 19 | 4641 | 0.6 | 53.7 | 19 | 2660 | 0.6 | 59.9 | 21 | 1981 | 0.5 | 47.1 |
| Epilepsy | 20 | 3972 | 0.5 | 45.9 | 23 | 1677 | 0.4 | 37.8 | 16 | 2295 | 0.6 | 54.6 |
| Multiple sclerosis | 21 | 3947 | 0.5 | 45.6 | 22 | 1774 | 0.4 | 40.0 | 18 | 2172 | 0.6 | 51.6 |
| Violence | 22 | 3723 | 0.5 | 43.1 | 18 | 2698 | 0.7 | 60.8 | 24 | 1026 | 0.3 | 24.4 |
| Leukaemia | 23 | 3691 | 0.5 | 42.7 | 20 | 2367 | 0.6 | 53.3 | 23 | 1324 | 0.4 | 31.5 |
| Hearing loss | 24 | 3560 | 0.5 | 41.2 | 25 | 1432 | 0.3 | 32.3 | 20 | 2128 | 0.6 | 50.6 |
| Total main causes | 639,996 | 81.4 | 7402.8 | 341,789 | 82.5 | 7699.5 | 298,207 | 80.1 | 7089.8 | |||
| Population total | 786,479 | 100.0 | 9097.2 | 414,346 | 100.0 | 9334.0 | 372,133 | 100.0 | 8847.3 | |||
DALY: disability-adjusted life years. Note: Some percent sums may not add up to 100% due to decimal rounding.
In our study, we have analysed the burden of disease in ages from 15 to 29 years, which represents 16% of the total population burden. Non-transmissible diseases, specifically the neurological and mental, constitute the main category in number of DALY. In particular, mental disorders as a group comprise the most frequent cause of burden of disease in Europe, due to their high prevalence and strong impact on patient quality of life, with significant economic and social repercussions.7–9 Coinciding with previous studies,10,11 depression is still the leading specific cause of burden of disease in adolescents and young people, while drug abuse is also notable (alcohol consumption held 2nd place and drug addiction was in 7th place), as well as some accidents and lesions (traffic accidents, falls and suicides). Gore et al.10 recently estimated that, for the world-wide adolescent population, depression (8.2%), traffic accidents (5.4%) and schizophrenia (4.1%) were the main causes of global burden of disease. In Spain, these 3 causes are also found among the main conditions that bring about poor health.
As in other studies,6,11–14 it is important to emphasise the lack of clinical records for most of the diseases analysed. This has led to using disability data for countries with an epidemiological pattern similar to our country's, assuming that morbidity in Spain behaves similarly to the European reference population. Some advances involve improving these estimations as the records with clinical-administrative information increase, along with growth in data from longitudinal attention programmes for young people such as information from social services and/or electronic clinical records. Even so, it is highly probably that some conditions or health problems continue under-reported and, consequently, underestimated. Examples are those that are not included in either questionnaires or statistics through apprehension, fear of social rejection or being stigmatised, such as suicides–which represent the 2nd cause of death in these ages, coming behind only traffic accidents in the mortality statistics.
Our results show that the burden of disease expressed in DALY makes it possible to define health losses in young people, where the principal causes of burden of disease rarely lead to death (except for accidents) or whose lethality is less than in other ages (such as cardiovascular disease or cancer in older people).12,13 For example, the poor mental health in young people is related to high prevalence in the adult and the vast majority of mental disorders in adults become chronic diseases that begin in adolescence.15
We did not analyse the burden of disease attributable to risk factors, but other authors10 suggest that it is low among young people. However, it is seen that alcohol abuse, drug addiction and sexually transmitted diseases (in women) weigh heavily in the burden of disease in young people. Other risk factors that generally begin in youth (e.g., smoking, obesity and high blood pressure) have great social and health impact in adults. In this sense, the health of adolescents and young people should also be analysed bearing in mind the acquisition of habits that may affect future health.
In summary, estimating DALY specifically for the adolescents and young people in Spain offers a systematic analysis of the burden of disease and is an important component in identifying the health problems needing greater attention from those who decide and plan health policies. The burden of disease in adolescents and young people in Spain is basically attributable to neurological and mental diseases. We hope that our study results contribute to more balanced health agenda in the National Health System, with appropriate investment in health research programmes, activities, specialised training programmes for professionals and early detection and intervention aimed at reducing health losses. Likewise, promoting and protecting young people's health are fundamental to guarantee a social structure and prevent the appearance of diseases in adults. Consequently, ensuring and improving the health of youngsters should continue to be a priority for those responsible for policies and for health professionals.
Ethical disclosuresProtection of people and animalsThe authors declare that no experiments have been performed on human beings or animals for this research.
Data confidentialityThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingThe authors received funding as research grants from the Instituto de Salud Carlos III-Fondo de Investigación Sanitaria (File No.: PS09/00086).
Conflict of interestsThe authors have no conflict of interests to declare. The opinions expressed herein are those of the authors, so they do not necessarily reflect the points of view of the organisms in which they work.
The authors wish to thank the anonymous evaluators of the Revista de Psiquiatría and Salud Mental for their comments, which have helped to improve the article. FCL and RGM contributed equally in this study and are the ones responsible for the article.
Please cite this article as: Catalá-López F, et al. Carga de enfermedad en adolescentes y jóvenes en España. Rev Psiquiatr Salud Ment (Barc.). 2013;6:80–5.