




During the COVID-19 pandemic, healthcare facilities have implemented contingency plans to minimize the consequences of this pathology however, the deployment and results of these contingency plans are scarcely shared.
ObjectivesTo describe the implementation of the contingency plan in the social and health care in the COVID-19 pandemic in the Public Hospital of Monforte (Lugo, Spain) and to evaluate the effectiveness of the measures included in this plan.
MethodPhenomenological sampling conducted between March 10 and May 15, 2020. Evaluation qualitative assessment by an external quality improvement team of the Galician Health Service (SERGAS), based on the Practicum Direct rapid structured checklist in risk management, organizational management, and evaluation of decision making. As outcome indicators, we assessed the number of hospital admissions, number of PCRs performed, telephone attention to social and health social-healthcare patients, number of hospitalizations avoided and estimation of their direct cost.
ResultsAfter assessing and managing the risks, an information security plan was developed and solutions to minimize complications in our patients derived from this pandemic. An emergency decision making team was created, as well as an employee communication mechanism for employees through standardized documents and documentation channels.
ConclusionsThe adaptation of the Practicum Direct rapid model to the healthcare setting is a useful and easy-to-apply tool that allows us to identify weak points and areas for improvement in our Service and thus to strengthen patient care in all clinical areas, improving the quality of care.
Durante la pandemia de la COVID-19 los centros sanitarios han puesto en marcha planes de contingencia para minimizar las consecuencias de esta enfermedad. Sin embargo, el despliegue y los resultados de estos planes de contingencia son escasamente compartidos.
ObjetivosDescribir la implantación del plan de contingencia en la atención sociosanitaria en la pandemia de la COVID-19 en el Hospital Público de Monforte (Lugo, España) y evaluar la efectividad de las medidas incluidas en dicho plan.
MétodoMuestreo fenomenológico realizado entre el 10 de marzo y el 15 de mayo de 2020. Evaluación cualitativa por un equipo externo de mejora de la calidad del Servicio Gallego de Salud, basada en la lista de verificación rápida estructurada Practicum Direct en gestión de riesgos, gestión organizativa y evaluación de la toma de decisiones. Como indicadores de resultado se valoraron el número de ingresos hospitalarios, el número de PCR realizadas, la atención telefónica a pacientes sociosanitarios, el número de hospitalizaciones evitadas y la estimación de su coste directo.
ResultadosTras evaluar y gestionar los riesgos se elaboró un plan de seguridad de la información y soluciones para minimizar las complicaciones en nuestros pacientes derivadas de esta pandemia. Se creó un equipo de toma de decisiones de emergencia, así como un mecanismo de comunicación para los empleados a través de documentos y canales de documentación estandarizados.
ConclusionesLa adaptación del modelo Practicum Direct rapid al ámbito sanitario es una herramienta útil y de fácil aplicación que nos permite identificar puntos débiles y áreas de mejora en nuestro servicio, y así reforzar la atención al paciente en todas las áreas clínicas, mejorando la calidad asistencial.
Spain was one of the countries most affected by the COVID-19 pandemic and many healthcare centers implemented contingency plans to minimize its consequences.1 However, neither the deployment of these contingency plans nor their results are hardly shared, depriving other health care services or hospitals of references to refute, compare or emulate the aforementioned plans. Our study could be useful for all those health areas with high rates of patients with chronic diseases in an aging, rural setting with high comorbidity. Galicia was the first region in Spain to reach the stage 4 level, related to the lower incidence of the coronavirus. During the pandemic, social and health care was one of the key issues in the deployment of contingency plans.
The objective is to evaluate the effectiveness of the measures included in the contingency plan developed by the team of COVID-19 experts of our health district and perform an external audit through the Practicum Direct rapid.2,3
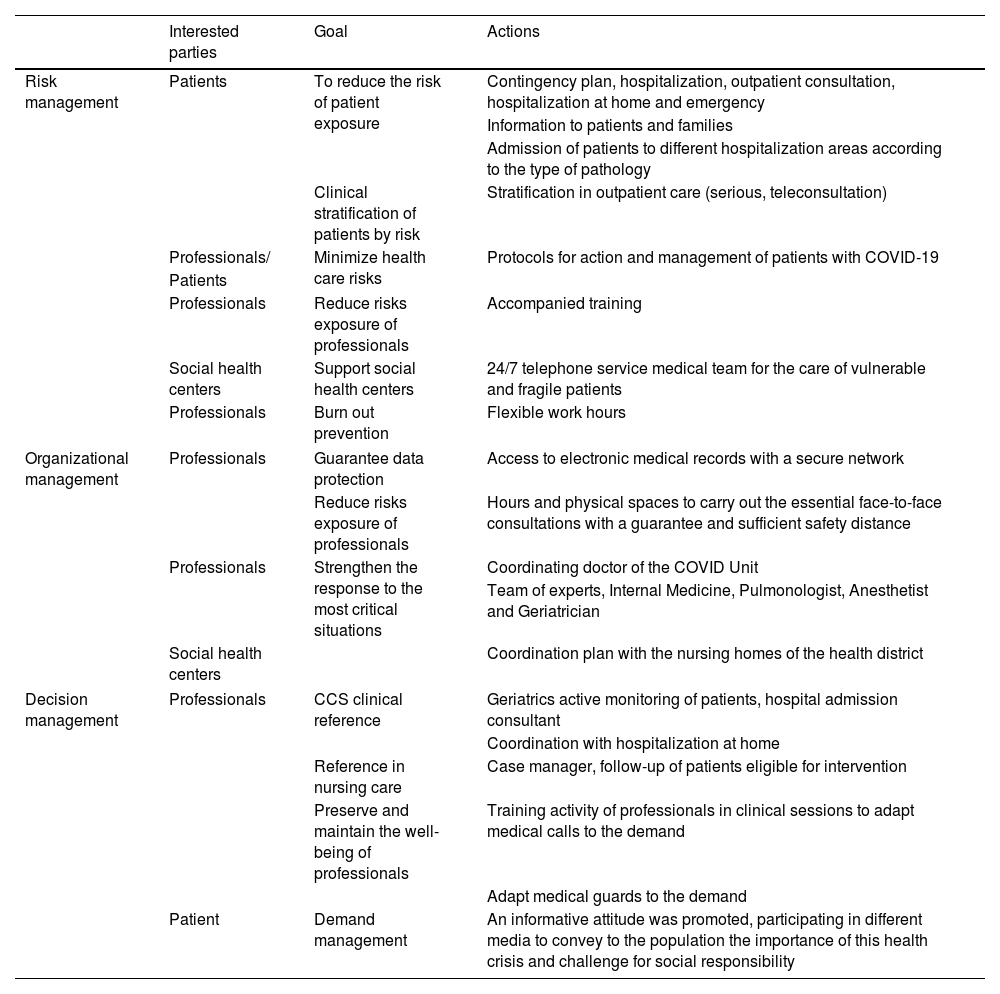
MethodsThe Servicio Galego de Saúde (SERGAS), located in the northwest of Spain, is a health care system that provides public health care to the population. SERGAS is a service of public provision of health structured in 7 health areas formed by health districts. Monforte Public Hospital is a regional hospital with a capacity of 141 beds, located in northwestern Spain and serves a population of approximately 42,250 inhabitants, characterized by a predominantly rural, aging and with high comorbidity. More than 35% of the population is over 65 years of age, being the area with the highest rate of comorbidity population and, therefore, with the highest number of social and health centers (n=11) in relation to its reference population.4 During the period from March 10 to May 15, 2020 a qualitative assessment under the phenomenological design with Practicum Direct rapid,2 by an external quality improvement team of the Servicio Galego de Saúde has been implemented. Practicum Direct rapid evaluates3 with a checklist, how the risk management, organizational management and pandemic decision making has been performed. The first phase is the discovery phase, in which themes are identified and concepts or ideas are developed. The second phase includes the classification and systematization of the data and the refinement of the understanding of the phenomenon studied. In the final phase, the analyst seeks to relativize his or her conclusions, seeking to understand the data in the context in which they were collected and in the eyes of the informants themselves (Table 1).
Interested parties identification, actions implemented according to risk management, organizational management and decision management at the Hospital de Monforte de Lemos (Lugo – Galicia).
| Interested parties | Goal | Actions | |
|---|---|---|---|
| Risk management | Patients | To reduce the risk of patient exposure | Contingency plan, hospitalization, outpatient consultation, hospitalization at home and emergency |
| Information to patients and families | |||
| Admission of patients to different hospitalization areas according to the type of pathology | |||
| Clinical stratification of patients by risk | Stratification in outpatient care (serious, teleconsultation) | ||
| Professionals/ | Minimize health care risks | Protocols for action and management of patients with COVID-19 | |
| Patients | |||
| Professionals | Reduce risks exposure of professionals | Accompanied training | |
| Social health centers | Support social health centers | 24/7 telephone service medical team for the care of vulnerable and fragile patients | |
| Professionals | Burn out prevention | Flexible work hours | |
| Organizational management | Professionals | Guarantee data protection | Access to electronic medical records with a secure network |
| Reduce risks exposure of professionals | Hours and physical spaces to carry out the essential face-to-face consultations with a guarantee and sufficient safety distance | ||
| Professionals | Strengthen the response to the most critical situations | Coordinating doctor of the COVID Unit | |
| Team of experts, Internal Medicine, Pulmonologist, Anesthetist and Geriatrician | |||
| Social health centers | Coordination plan with the nursing homes of the health district | ||
| Decision management | Professionals | CCS clinical reference | Geriatrics active monitoring of patients, hospital admission consultant |
| Coordination with hospitalization at home | |||
| Reference in nursing care | Case manager, follow-up of patients eligible for intervention | ||
| Preserve and maintain the well-being of professionals | Training activity of professionals in clinical sessions to adapt medical calls to the demand | ||
| Adapt medical guards to the demand | |||
| Patient | Demand management | An informative attitude was promoted, participating in different media to convey to the population the importance of this health crisis and challenge for social responsibility | |
As outcome of hospital admissions an inappropriate admission was considered to be that which, having been indicated by a professional and communicated to the admissions coordinator, is finally referred to another level of care.
ResultsPandemic risk managementIn relation to the Outpatients’ Departments, patients were stratified according to their clinical and two groups of patients were defined, which made it possible to differentiate the less severe patients who were candidates for telecare4,5 patients, who were candidates for teleconsultation (by telephone or e-mail), from the group of patients for whom face-to-face consultation would be essential due to the complexity of their pathology.6 At the same time, a specific plan was established to intensify support to the social and health centers in our area (institutions for the elderly and dependents) and a 24-hour hotline was set up for the medical team to handle queries related to the most vulnerable and fragile patients. Measures were put in place to provide flexible working hours for healthcare professionals and to reinforce medical on-call duty, in addition to and alternative duty rosters in the event of multiple medical leaves of absence. The area for improvement identified was related to risk assessment and the establishment of emergency response mechanisms by means of a systematic evaluation system using the standard risk management tools.
Organizational management of the pandemicTelematic access to the electronic medical records with a secure network was authorized, the risk of SARS-CoV-2 infection was monitored and telephone assistance to patients and family members was intensified to resolve doubts, questions and clinical information. The timetables and physical spaces were organized to carry out the necessary face-to-face consultations with sufficient guarantee and safety distance. A COVID Unit Coordinating Physician was appointed and a team of experts was set up, including Internal Medicine Specialists, a Pneumologist, an Anesthesiologist and a Geriatrician, to make decisions and interact with professionals from other specialties with the aim of reinforcing the response to the most critical situations.7–9 A decision algorithm with readily available clinical parameters was adopted to assist the medical ward physicians in choosing the appropriate supplemental oxygen therapy and ventilatory support.10 In addition, clear indications were provided for safe tracheal intubation and protective pulmonary ventilation, and, if necessary, the transfer of such patients to the appropriate Intensive Care Units for our health area where specific protocols would be applied.11,12
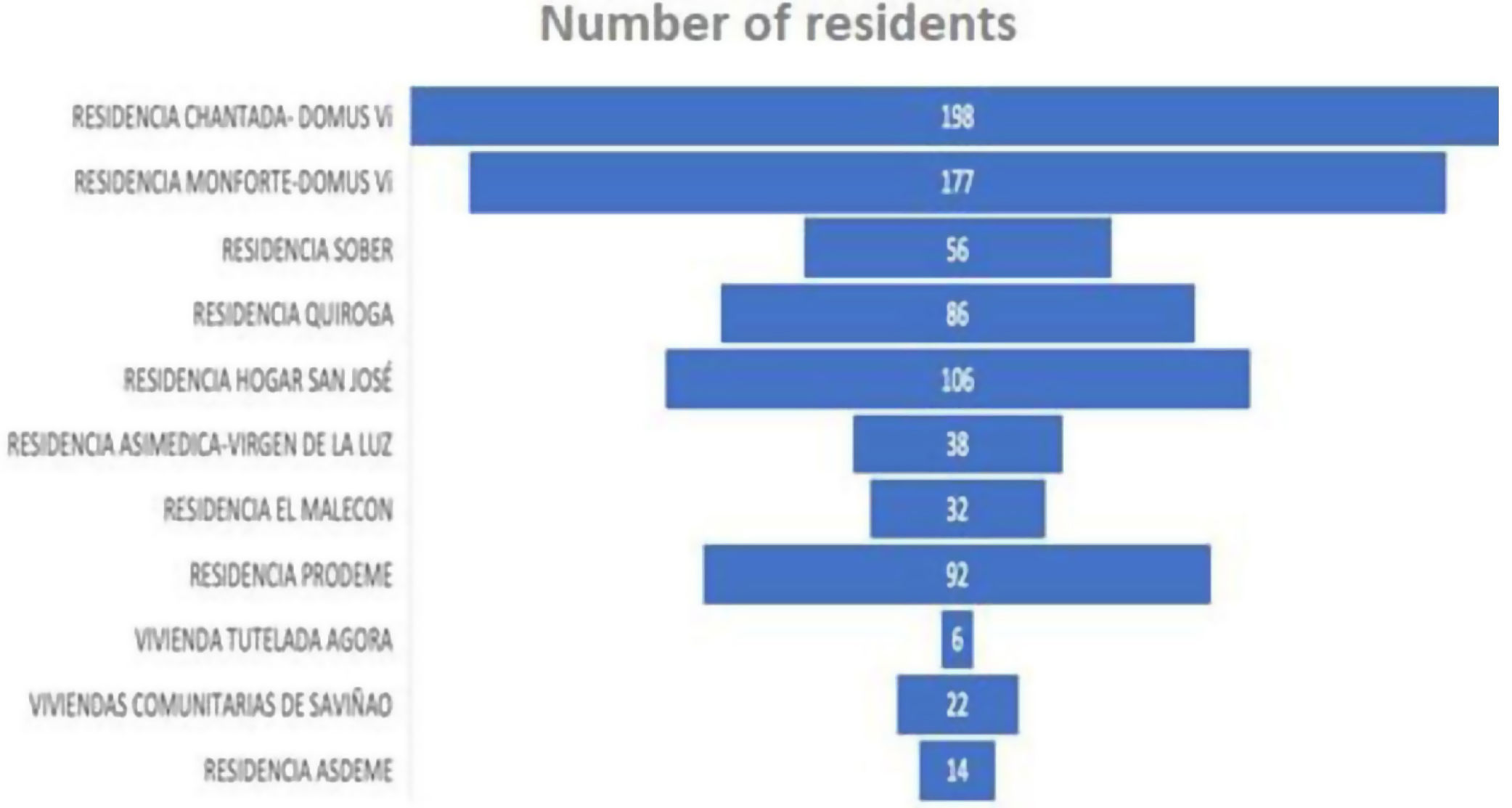
Decision-making in the face of the pandemicThe specialist in Geriatrics was the reference person for the social-health centers, providing continuous telephone attention and was not satisfied with being only a mere reference for information on pathologies, but frequently participated in the decision making and proactive follow-up of patients, recommending if necessary the transfer to the hospital or the visit of the nursing team and home hospitalization doctor. A coordination plan was structured with the geriatric residences of the health district, a total of 11 centers (which also included sheltered housing and residences for people with disabilities) in order to identify COVID-19 positive patients who could benefit from a referral to hospital centers to improve the prognosis of survival and quality of life in the short and long term, minimizing the spread of the disease, protecting both the other residents and the staff caring for these patients and ensuring access to protective equipment and medication for hospital use in residential facilities (Fig. 1). To this end, an active daily telephone follow-up was carried out with the residences through a case manager nurse identifying those patients in need of intervention. An attempt was made to optimize and make schedules more flexible with the aim of preserving and maintaining the well-being of the professionals, trying to optimize and make schedules more flexible trying to prevent burn-out syndrome as far as possible,7,8 training of professionals was reinforced in brief daily multidisciplinary meetings and the establishment/facilitation and communication mechanisms with institutions, patients and family members. An informative attitude was promoted, with participation in different media to inform the public about the media to convey the importance of this health crisis to the population and to call for social responsibility.13

In the 9 weeks included in the audit, of the 827 residents belonging to the 11 centers in the district residents 50 patients were included in the program. Of which 4 (0.48%) were positive for COVID. During program follow-up, 1044 telephone calls were made and 36 hospital admissions were avoided. A total of 821 PCRs were performed on residents and 429 PCRs on workers.4,5 With the application of preventive and organizational actions (Table 1), we consider that we have had a low incidence of infected patients.
DiscussionThe following website protocols for action and management of patients with COVID-19 were drawn up and a strategy was defined to distribute the patients admitted to different hospitalization areas according to the type of pathology, in order to minimize the risk of exposure of patients and healthcare professionals.4,5 Galicia has been the territory with the best vaccination data and has been the first region to reach the zero level of the pandemic in Spain.14 After the risk analysis and management, the organizational phase, where alternatives were proposed that influenced effective decision making. In March 2020, the COVID Unit was created at the Hospital de Monforte, and in a separate circuit was established for the diagnosis and management of patients with suspected or confirmed COVID and a team of experts was set up to draw up a contingency plan to respond to the specific health care needs arising from the pandemic. The measures instituted have been modified according to the improvement and action plans are dynamic, with the aim of adapting our response to the healthcare needs of our patients according to the unpredictable evolution of the pandemic by adopting a method that allows us to provide the best response in the shortest possible time.15,16
In the Internal Medicine Department of the Public Hospital of Monforte de Lemos, the possible risks of the COVID-19 pandemic were analyzed and a contingency plan for the areas of hospitalization, outpatient, home hospitalization and emergency. We promoted the training of professionals and reinforced information to patients and family members in order to avoid risks related to SARS-CoV-2 infection in the center. Although measuring the quality and safety of medical care is a laborious process, once these results have been obtained, they have been brought to the attention of medical and out-of-hospital staff, and have been presented to the public through the usual means of communication, since it is known that quality measurement is essential both in times of stability as well as in times of crisis; when extra effort is required from health care workers (and in any other professional field), the need for them to understand the quality and safety of that care and the result of the extra effort made in the face of the proposed challenge, becomes extremely relevant. Poor understanding of the quality of care provided, whether or not there is a public health crisis, should be systematically avoided11 and while similar models have been implemented in other centers, including in the surgical area,1 it is a matter of doing what is right, but adapted to each moment7 and learning to improve every day a little more. It is a matter of not repeating mistakes and taking advantage of the best practices that are discovered with this research. We cannot continue with the trial-and-error model for the deployment of contingency plans and transparency in decision making in situations of uncertainty.17 In short, sharing our contingency plans in order to find reference models in the management of the exceptional. Taking advantage of the situation experienced during the COVID-19 pandemic in our area, we have promoted a transparent analysis of what happened in order to prepare the center for a possible situation of the pandemic experience, in order to deal quickly and flexibly with any situation that may test the capacity of the health system, aligned with the hospital's strategic plan. Decision-making in situations of uncertainty is not uncommon. However, it would not be acceptable to repeat mistakes that we have already identified in this pandemic.17 In our setting, evaluations of the impact of the third wave have been carried out in health care centers, where the start of vaccination modified the results with respect to our experience.18
LimitationsIn our health district, the population over 65 years of age exceeds 35%, being the health district with the highest percentage of aging population in Galicia and with the highest number of social-health centers (n=11) in relation to its reference population (42,250 inhabitants). Our hospital was planned in a very difficult environment and with an extremely aging population and it would be unforgivable not to create information from the data to identify the key elements of the response to COVID-19 in the care of critically ill patients. Another strength, is a view from risk prioritization, organizational management and decision making. The value proposition we want to achieve with this assessment is to approach a systematic approach to identify best practices and ideally, an outcome metric for critical patient care in an epidemic environment. Given the phases in the COVID-19 pandemic, we should have learned from the different measures that have been implemented. Our experience can be a useful tool for immediate self-assessment of the deployment of contingency plans.
ConclusionsDefining a contingency plan to address the COVID-19 pandemic was crucial, as was systematically implementing the measures included in it. The application of the Practicum Direct rapid2,3 is a useful and easy-to-apply tool that allows us to identify weaknesses in order to improve inpatient and outpatient care, increase support to Primary Care and other socio-health institutions. Overall, in the first wave there was a low incidence of COVID-19 cases recorded in the residences of the Monforte Health District and among the main reasons were the multidisciplinary work and the focused and patient-centered care, carried out in a cross-cutting manner between the hospital and residential environment as well as the initial PCR screening test performed on all residents and workers in the residential centers. Thanks to this analysis, to date we can say that the impact of the pandemic in the health area was minimized, the consultations were favorably managed, creating a specific post COVID to follow up patients after hospital discharge and the COVID Team of the Monforte Public Hospital was consolidated, demonstrating that this tool can be applicable to small hospitals (less than 200 beds) and our center is a good example of this. From our hospital we believe that there is nothing better than sharing our contingency plans and pooling our problems to find reference models to manage exceptional situations such as the one that occurred during the SARS-CoV2 pandemic, since such mutualization could serve to improve our results in the management of COVID-19 patients and also in the event of similar situations in the future.16
FundingThis study has been funded by the Galician Agency of Innovation through project IN845D 2020/03, in the framework of the Feder Galicia 2014-2020 operational program (co-financed by the European Regional Development Fund, “A way to make Europe”) by the European Regional Development Fund, “A way of doing Europe”.
Conflict of interestNone declared.
We would like to thank Dr. Romina González Vázquez for her collaboration in the translation of this article.
