




Mammary hamartoma was first described by Arrigoni et al.1 in 1971 and is a rare benign tumor, although presumably underdiagnosed.2 Usually present as painless, well-circumscribed and mobile breast lump. Histologically consist of various amounts of glandular tissue, fat, fibrous tissue, and occasionally muscle, hyaline cartilage and a thin capsule.2,3 We present a case of breast hamartoma in male.
A thirty-two year old male was observed in our consultation for a slowly growing and painless right breast lump. The patient denied nipple discharge or other symptoms. Examination revealed a well-defined, soft and mobile lump in the external upper quadrant of the right breast. There were no inflammatory signals or palpable lymph nodes.
Ultrasound study showed no specific alterations, with a nonspecific and ill-defined area of increased density in the right breast. By the persistence of this pseudonodular area on palpation and discomfort mentioned by patient, and according to the patient's will, surgical treatment was proposed, with excision of small densification of breast tissue from the right breast.
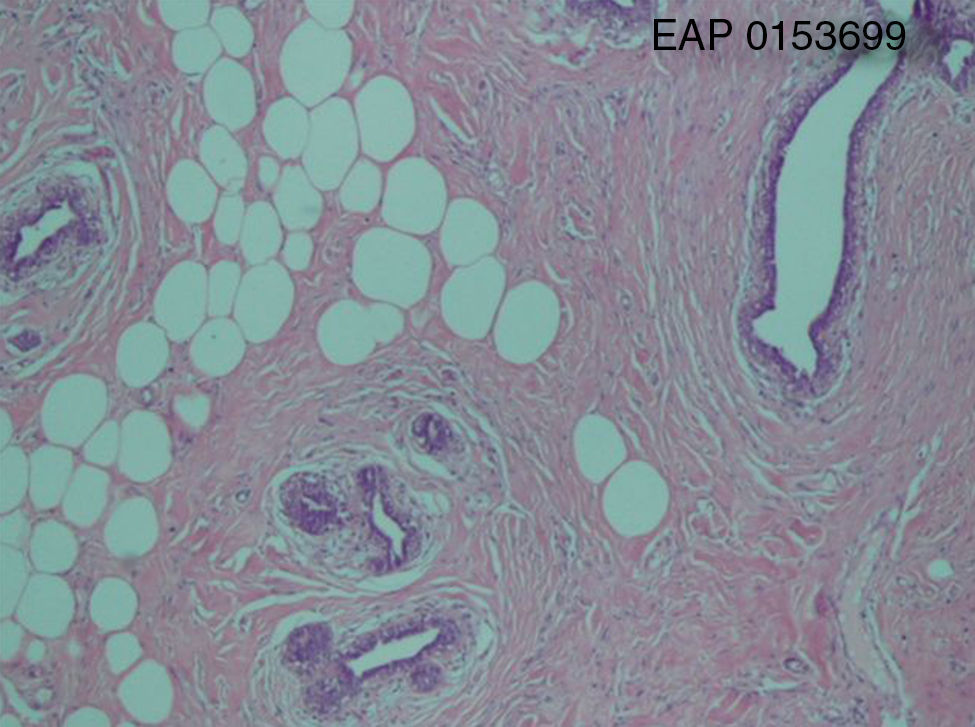
Histological examination of the nodular fragment of 3.2cm×2.5cm showed a disorganized overgrowth of mammary tissues with variable amounts of fatty tissue, fibrotic stroma and epithelial elements with mild epithelial hyperplasia. Without a typical capsule, the nodule was well demarcated from the adjacent breast tissue by fibrous tissue (Fig. 1).
, showing disorganized overgrowth of mammary tissues with variable amounts of fatty tissue, fibrotic stroma and epithelial elements.")
Mammary hamartoma has an incidence of 0.1–0.7% in the literature,2,3 and only 4 cases described in males, 2 in adults4,5 and another 2 in pediatric age.6,7 Hamartomas presents at any age group but are more common in premenopausal and perimenopausal women. It is a benign lesion, although it has already been described in association with carcinoma in situ and lobular carcinoma.8 The diagnosis is difficult and relies on the correlation between the clinical and typical radiological findings (oval-shaped masses with heterogeneous density, ill-defined limits and occasionally a radiolucent halo).3,9 The ultrasound has no utility in the diagnosis of this entity as descriptions show variable and non-specific sonographic appearance.10
Previous reports have shown variable cytological and histological characteristics of breast hamartoma and some attempts have been made to subclassify hamartomas, although none of them has been widely accepted. Jones et al. suggested a four category classification of encapsulated fibrocystic changes, fibroadenoma with fibrous stroma, fibroadenoma-like and circunscribed adenolipoma based on hystological parameters.11 The main interest of fine-needle aspiration cytology was the exclusion of malignancy, regarded the similarities of other benign lesions as fibroadenoma.12 Although both represent a benign fibroepitelial growth of breast tissues, some studies have been pointing out differences in cytological aspects. Herbert et al. showed that the finding of intact lobular units and various amounts of adipose tissue favored a diagnosis of breast hamartoma over fibroadenoma. The most common histological pattern, as seen in this case, is that of a lesion with well demarcation from adjacent breast tissue, intact lobules and interlobular adipose tissue and fibrotic stroma. Other frequent characteristics are epithelial hyperplasia and pseudo-angiomatous stroma hyperplasia.13
As the differential diagnosis it is important to consider not only frequent benign lesions such as fibroadenoma or fibrocystic disease but also diseases as the breast adenomyoepithelioma, diabetic mastopathy, intramammary lipoma or breast lesions associated with Cowden's disease, usually with multiple hamartomas and pathognomonic mucocutaneous lesions.12
The breast hamartoma does not require surgical treatment when the diagnosis is previously established, the lesion is small and the patient is young. In this case it is only indicated a radiological surveillance.

