



The authors present the case of a 42-year-old man, smoker (90 pack-years) with a history of alcohol consumption and past use of illicit drugs, medicated for arterial hypertension, dyslipidemia, and gastroesophageal reflux, who went to the Emergency Department for suspected aspiration of a chicken bone (foreign body – FB). On admission, he was tachypneic, with cough and stridor, hemodynamically stable, without oxygen desaturation. Initial chest X-ray showed signs of hyperinflation of the left lung with a contralateral mediastinal shift (Fig. 1A). Chest computed tomography (CT) showed a FB in the left main bronchus (Fig. 1B). A chicken bone was removed using rigid bronchoscopy (Fig. 1C). The local bronchial mucosa showed inflammatory signs, but the procedure was performed without immediate complication. Three hours later, chest CT revealed a moderate pneumomediastinum, gas in the bronchovascular sheath to the left hilum, mild interstitial emphysema in the left lower lobe, and mild emphysema in the neck (Fig. 1D and E). The patient improved clinically and radiologically (Fig. 1F) and was discharged three days after the procedure, asymptomatic and without signs of infection.
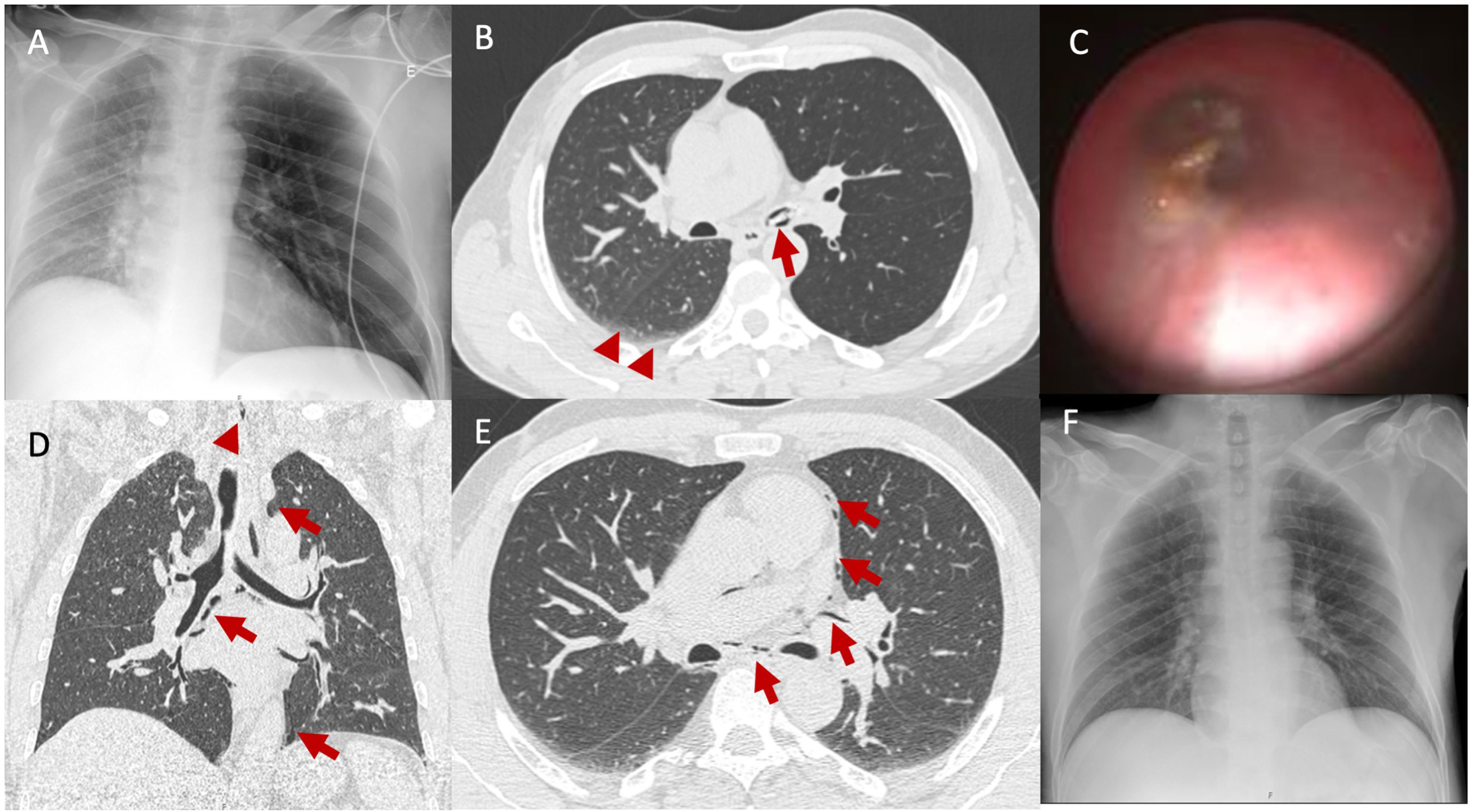
 Initial chest X-ray showing signs of left lung hyperinflation with a contralateral shift of the mediastinum and reduced right lung expansion. (B) Chest CT presenting the FB in the left main bronchus (arrow), signs of left lung hyperinflation, and areas of subsegmental atelectasis in the right lung (arrowheads) – complete chest CT available as supplemental material (video 1). (C) Bronchoscopic view of the FB (chicken bone) in the left main bronchus. (D and E) Post-procedure chest CT depicting a pneumomediastinum (arrows), presence of gas in the bronchovascular sheath to the left hilum, mild interstitial emphysema in the left lower lobe, and mild emphysema in the neck (arrowhead) – complete chest CT available as supplemental material (video 2). (F) Chest X-ray two days after the procedure showing normal lung expansion bilaterally, with centered mediastinum, already found in the CT 3h after the procedure.")
(A) Initial chest X-ray showing signs of left lung hyperinflation with a contralateral shift of the mediastinum and reduced right lung expansion. (B) Chest CT presenting the FB in the left main bronchus (arrow), signs of left lung hyperinflation, and areas of subsegmental atelectasis in the right lung (arrowheads) – complete chest CT available as supplemental material (video 1). (C) Bronchoscopic view of the FB (chicken bone) in the left main bronchus. (D and E) Post-procedure chest CT depicting a pneumomediastinum (arrows), presence of gas in the bronchovascular sheath to the left hilum, mild interstitial emphysema in the left lower lobe, and mild emphysema in the neck (arrowhead) – complete chest CT available as supplemental material (video 2). (F) Chest X-ray two days after the procedure showing normal lung expansion bilaterally, with centered mediastinum, already found in the CT 3h after the procedure.
FB aspiration is a rare but potentially life-threatening event in adults. Most accidental aspirations occur in children, with adults accounting for 25% of cases.1 This occurrence invariably leads to bronchoscopy. In adults, foreign body removal accounts for 0.16–0.33% of bronchoscopic procedures. FB aspiration can lead to air trapping and lung hyperinflation on the side of FB impaction due to a ball-valve phenomenon,2 which is more frequently observed in children and seldom reported in adults. While this phenomenon is associated with an increased risk of pneumothorax, the occurrence of pneumomediastinum after FB aspiration is rare, presenting an incidence of 1.5% in the pediatric population. In adults, its incidence has not yet been described. In this case, pneumomediastinum might have resulted from lung hyperinflation, increased alveolar pressure and rupture, or bronchial trauma. In fact, bronchial trauma might have happened during the bronchoscopic procedure or resulted from perforation by the foreign body, which acted as a plug while kept in place but was responsible for an air leak to the peribronchial sheat once removed.
The authors point out that the ball-valve phenomenon should be considered in cases of FB aspiration in adults, even if the entire presentation is atypical.
Informed consentInformed consent was obtained from the patient to publish this case report and any accompanying images.
FundingNone declared.
Authors’ contributionsAll authors participated in the patient's treatment, data collection, writing, and revising the manuscript. All authors read and approved the final manuscript.
Conflicts of interestAll authors declare that they have no conflicts of interest to disclose.
