




Laparoscopic sacral colpopexy (LSC) is the gold standard treatment for apical pelvic organ prolapse (POP). Artificial urinary sphincter (AUS) is highly effective in the treatment of recurrent stress urinary incontinence (rSUI).
ObjectiveTo describe, for the first time, the technique of LSC and laparoscopic AUS implantation through a vesicovaginal approach to the posterior aspect of the bladder neck.
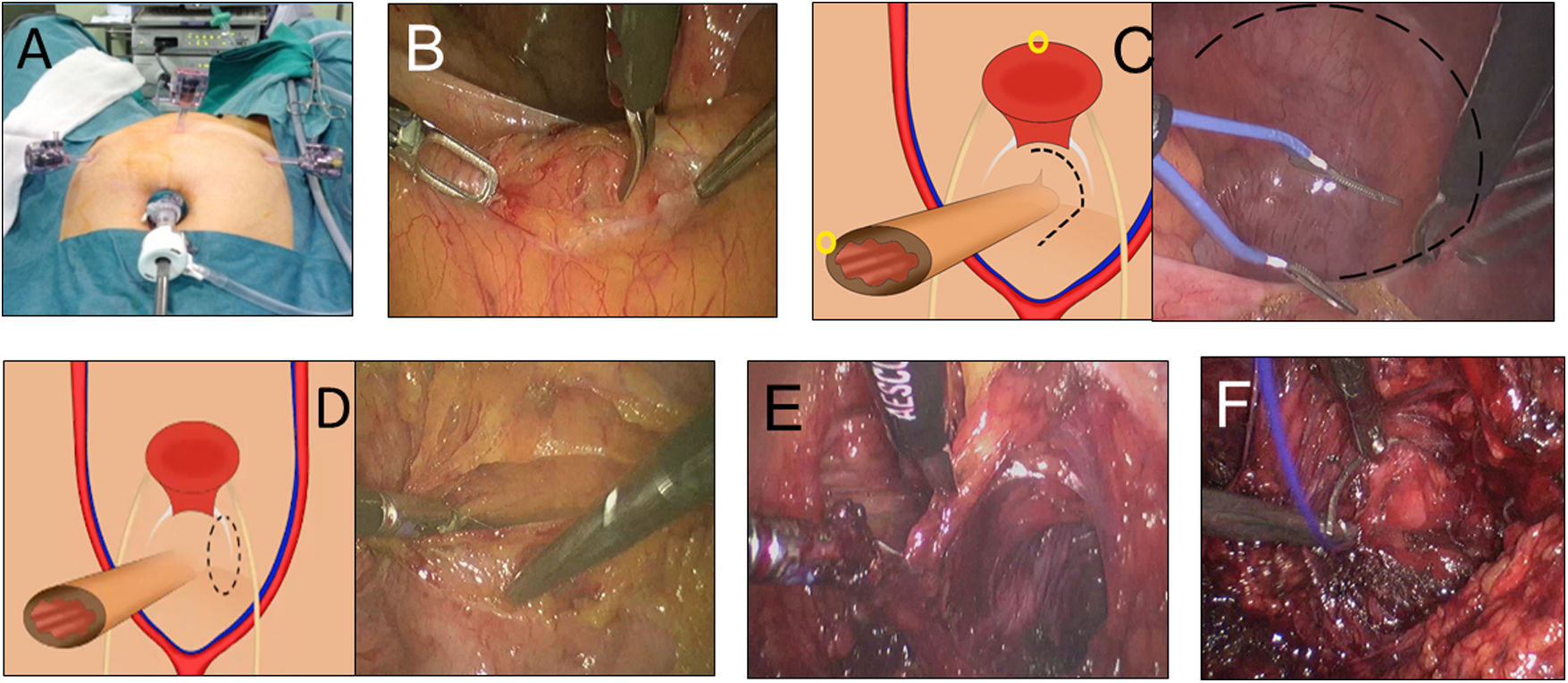
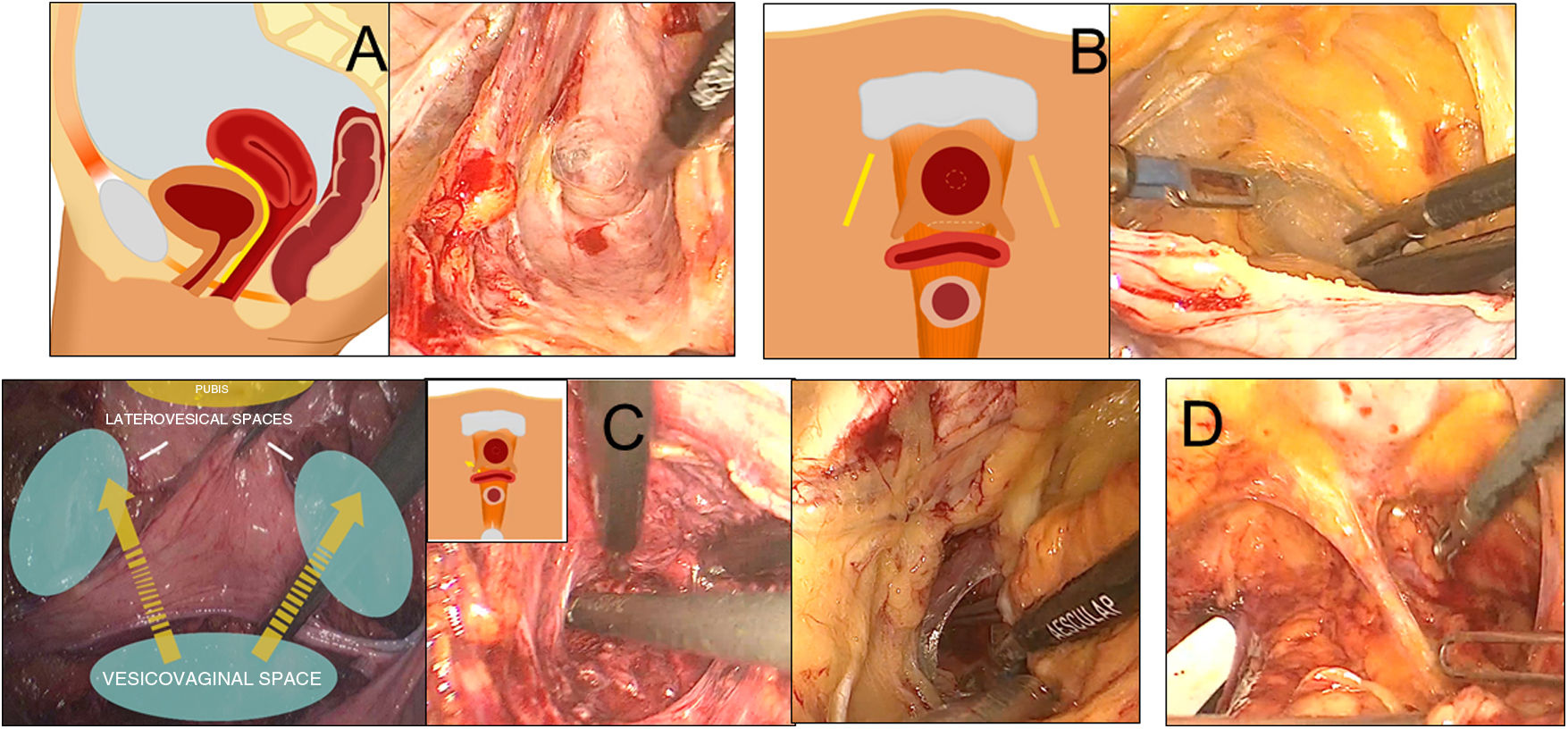
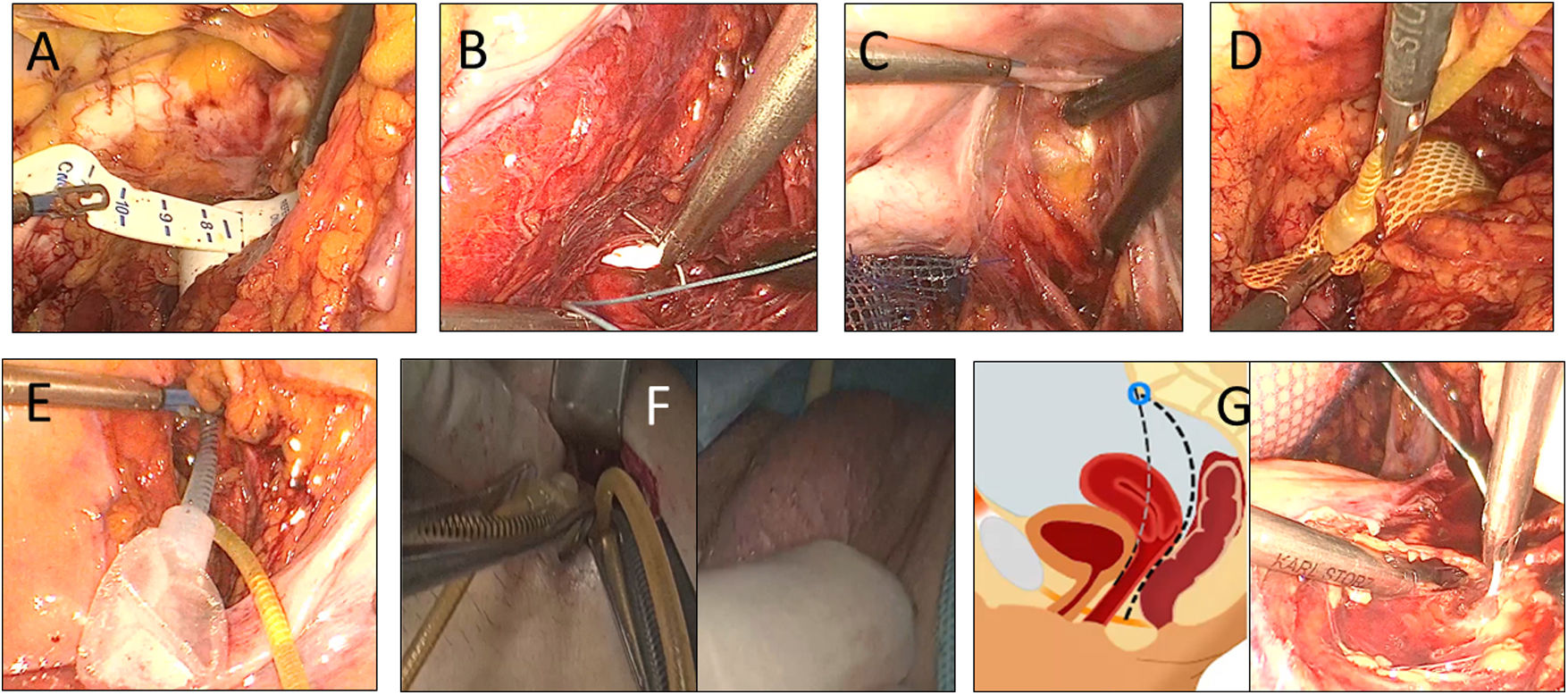
Material and methodsSurgery is performed by a transperitoneal approach. The rectovaginal space is created and the posterior mesh is fixed. The vesicovaginal space and both laterovesical spaces are dissected. The vesicovaginal space is connected to both lateral spaces. This is main step of the procedure because it let us place the cuff around the bladder neck in a non-blind fashion. The anterior mesh is fixed to the vagina. The anterior side of the neck is dissected and the cuff is placed. Both meshes are fixed to the promontory. The pressure-regulating balloon is inserted, the pump is placed in the labia majora and connections are made as usual. Finally, the peritoneum is closed.
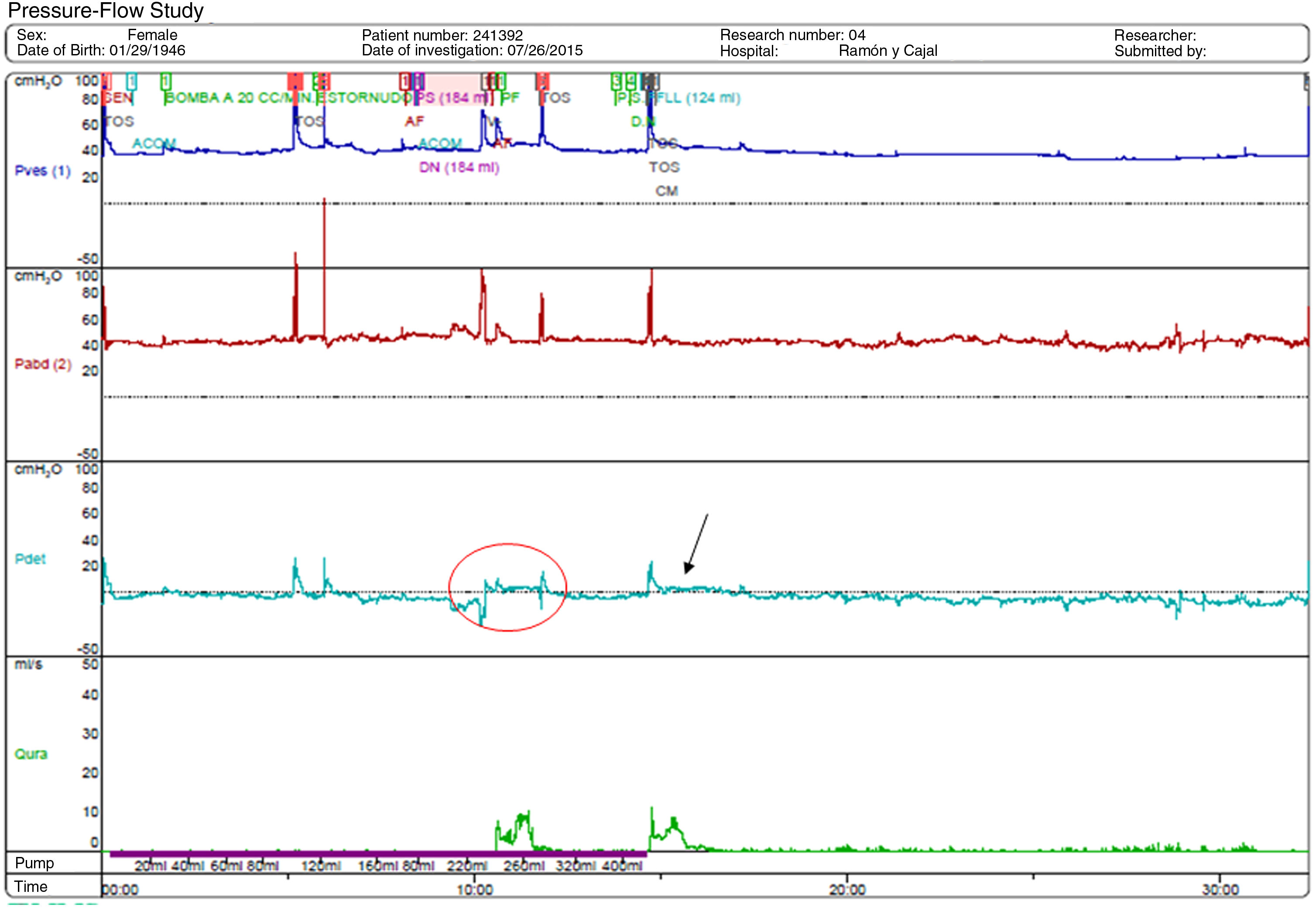
ResultsOperative time was 180 min; bladder catheter was removed on the 5th. postoperative day and hospital stay was 5 days. AUS was activated after 6 weeks. There were no perioperative complications. After 12 months, the patient achieved complete continence and objective and subjective POP repair.
ConclusionsVesicovaginal dissection is a shared step in LSC and in this technique of AUS placement Direct vision of the bladder neck would reduce the risk of erosion. We recommend this technique in selected cases of POP and rSUI.
La colposacropexia laparoscópica (CL) es el tratamientogold standard del prolapso de órganos pélvicos (POP) apical. El esfínter urinario artificial (EUA) presenta elevada eficacia en el tratamiento de la incontinencia urinaria de esfuerzo recidivada (IUEr).
ObjetivoDescribir por primera vez la técnica de CL e implante laparoscópico de EUA mediante un abordaje vesicovaginal a la cara posterior del cuello vesical.
Material y métodosLa cirugía se realiza por un abordaje transperitoneal. Se crea el espacio rectovaginal y se fija la malla posterior. Se realiza la disección del espacio vesicovaginal con ayuda de una valva vaginal, se crean los espacios laterovesicales y se comunican ambos con el espacio vesicovaginal. Se fija la malla anterior. Se diseca la cara anterior del cuello y se coloca el manguito. Se fijan ambas mallas al promontorio. Se introduce el reservorio, se coloca el botón de activación en el labio mayor y se realizan las conexiones de forma habitual. Finalmente, se cierra el peritoneo.
ResultadosEl tiempo quirúrgico fue 180 minutos, la sonda vesical se retiró al 5º día y la estancia fue de 5 días. El EUA se activó a la 6ª semana. No hubo complicaciones perioperatorias. Tras 12 meses la paciente presenta continencia completa y curación objetiva y subjetiva del POP.
ConclusionesLa disección vesicovaginal es un paso común en esta técnica de CL y colocación de EUA. La visión directa del cuello vesical permitiría disminuir el riesgo de erosión. Recomendamos esta técnica en casos seleccionados de POP e IUEr.

