




Ureteroileal anastomosis stricture is a frequent complication after radical cystectomy and ileal conduit or orthotopic neobladder formation. We analyze their incidence based on the technique for urinary diversion and on the surgical approach (open, laparoscopic or robot-assisted). Stricture management is described, along with surgical outcomes.
Material and methodsDescriptive retrospective study over 6 years in patients who underwent urinary diversion using ileum (ileal conduit or orthotopic neobladder). Demographic data, comorbidities, surgical approach, complications, and outcomes were collected. Minimum follow-up of 1 year. Comparison between groups using Chi-square test for dichotomous variables. Quantitative variables were compared using the Student’s t-test for independent groups or Mann-Whitney test. Statistical significance if P < .05.
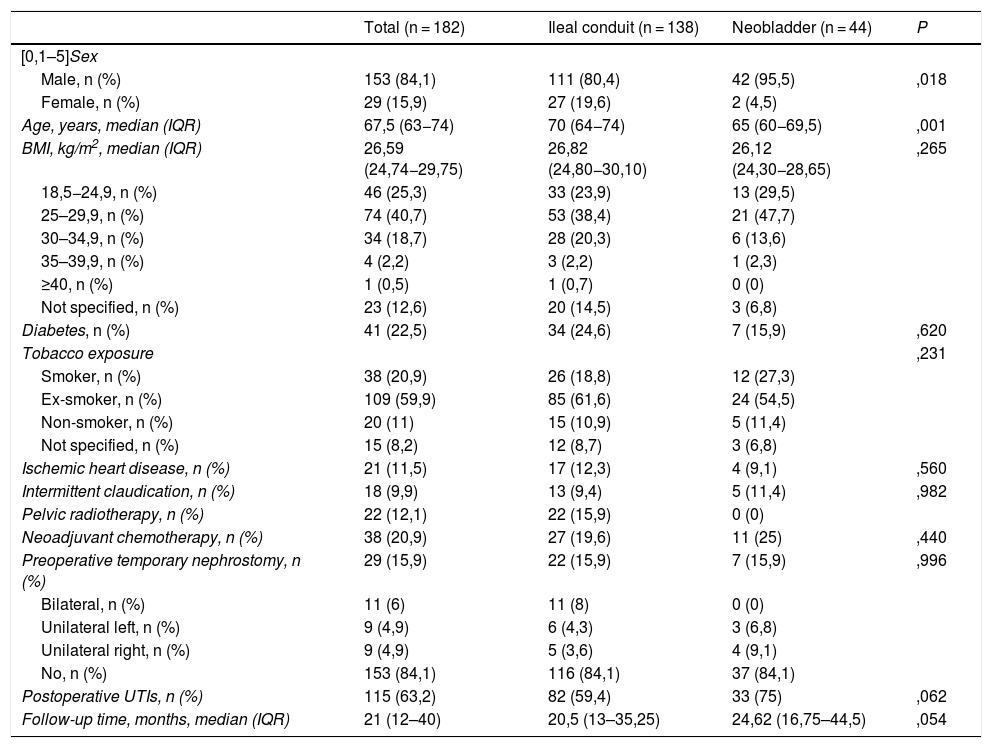
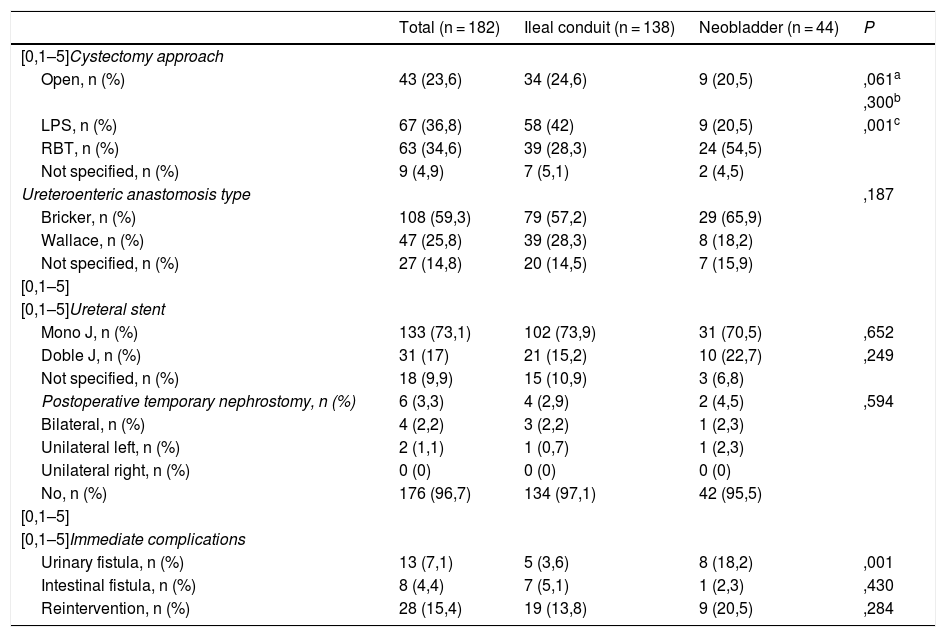
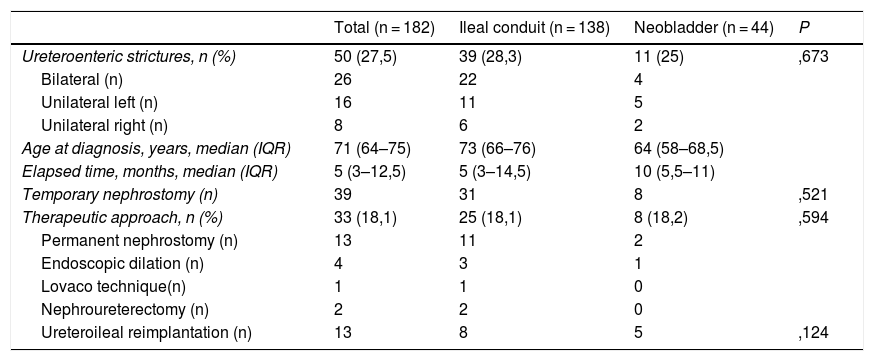
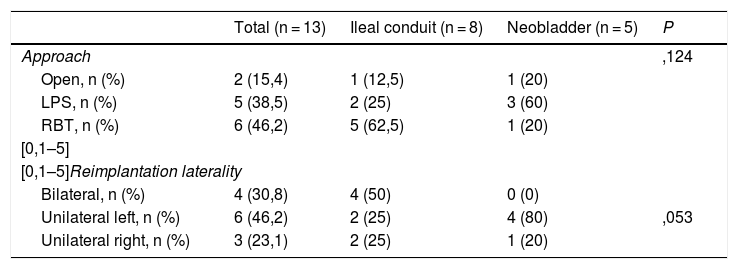
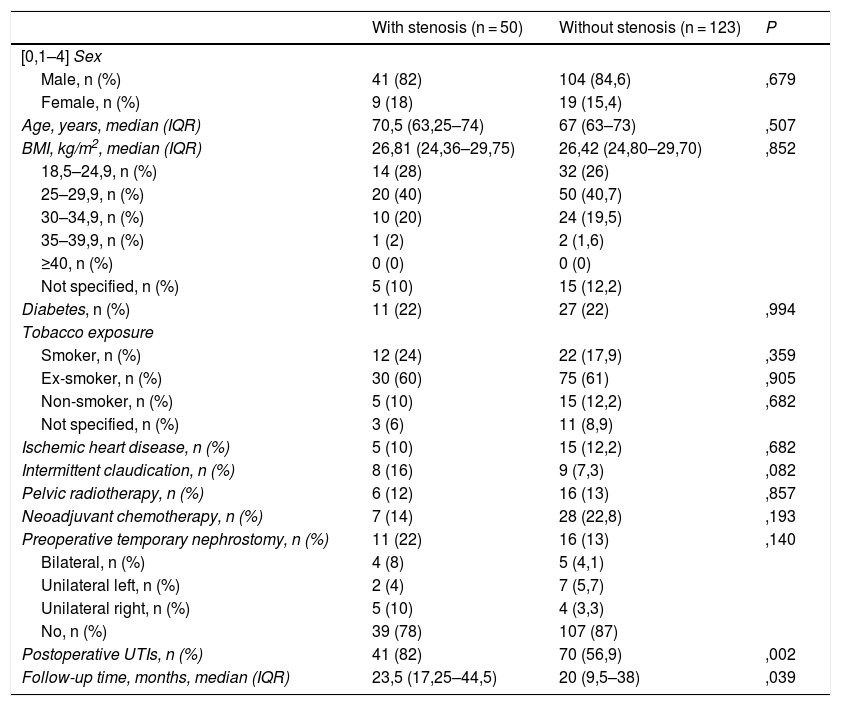
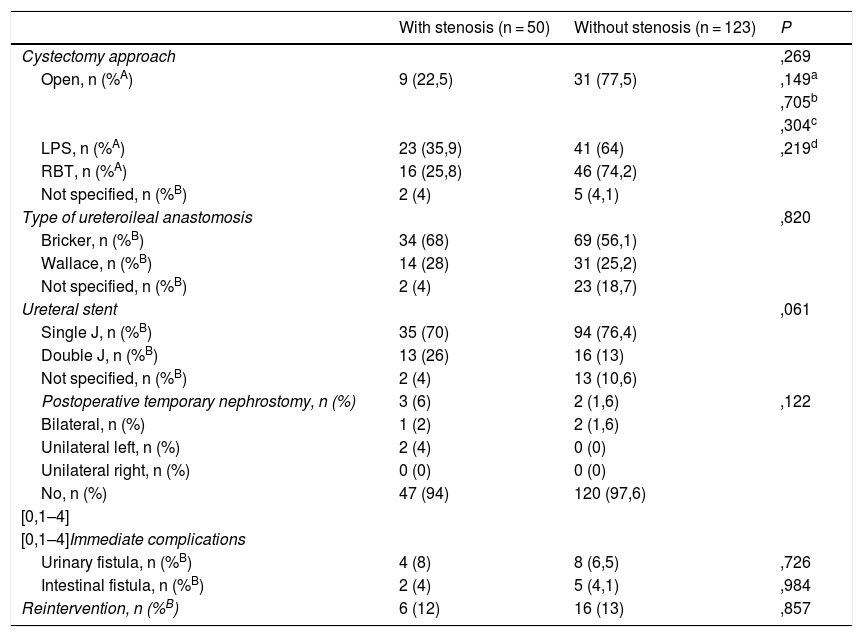
ResultsThe study included 182 patients (84% males and 16% females). Mean age 68 years. Cystectomy approach: laparoscopic (67/37%), robot-assisted (63/35%), open (43/24%). Urinary diversion: ileal conduit (138/76%) and orthotopic ileal neobladder (44/24%). Uretericre implantation technique: Bricker (108/59%) and Wallace (47/26%). Ureteroileal anastomosis strictures (50/27%): bilateral (26), left (16) and right (8). Strictures according to cystectomy approach: laparoscopic (23/46%), robot-assisted (16/32%), open (9/18%). Treatment of strictures (33/18%): ureteric reimplantation (13), indwelling nephrostomy (13), endoscopic dilatation (4), nephroureterectomy (2), endoureterotomy (1). Ureteroileal reimplantation approach: laparoscopic (5/38%), robot-assisted (6/46%), open (2/15%). Outcomes after reimplantation: restenosis (0/0%), reintervention (3/23%), contralateral ureteroileal stricture (1/8%).
ConclusionSurgical approach in cystectomy does not influence future development of ureteroileal strictures. Laparoscopic and robot-assisted ureteroileal reimplantation achieves high success rates.
Las estenosis de anastomosis uréteroileal son complicaciones frecuentes en conductos ileales y neovejigas ortotópicas. Analizamos su incidencia en función del tipo de derivación urinaria y del abordaje quirúrgico (abierto, laparoscópico o robótico). Describimos su manejo y los resultados obtenidos.
Material y métodosEstudio retrospectivo descriptivo durante 6 años en pacientes con derivación urinaria empleando íleon (conducto ileal o neovejiga ileal). Se recogen datos demográficos, comorbilidades, datos quirúrgicos (abordaje, complicaciones) y resultados. Seguimiento mínimo de 1 año. Comparación entre grupos, mediante test de Chi cuadrado en variables dicotómicas. Variables cuantitativas comparadas empleando T de Student para grupos independientes, o prueba de Mann-Whitney. Consideramos significación estadística P < .05.
ResultadosIncluimos 182 pacientes (84% varones y 16% mujeres). Edad media 68 años. Abordaje de cistectomía: laparoscópica (67/37%), robótica (63/35%), abierta (43/24%). Tipo de derivación: conducto ileal (138/76%) y neovejiga ileal ortotópica (44/24%). Tipo de reimplante: Bricker (108/59%) y Wallace (47/26%). Estenosis de anastomosis uréteroileal (50/27%): bilateral (26), izquierda (16) y derecha (8). Estenosis según abordaje de cistectomía: laparoscópica (23/46%), robótica (16/32%), abierta (9/18%). Tratamiento de estenosis (33/18%): reimplante uréteroileal (13), nefrostomía permanente (13), dilatación endoscópica (4), nefroureterectomía (2), endoureterotomía (1). Abordaje del reimplante: laparoscópico (5/38%), robótico (6/46%) y abierto (2/15%). Resultados tras reimplantes: reestenosis (0/0%), reintervención (3/23%), estenosis uréteroileal contralateral posterior (1/8%).
ConclusiónEl tipo de abordaje empleado en la cistectomía no parece influir en la aparición de estenosis uréteroileales. Abordajes laparoscópicos y robóticos permiten su reparación con resultados favorables en un porcentaje elevado de pacientes.

