



INTRODUCTION
In the last 10 years, the eosinophilic esophagitis has become an emergent entity 1 due to a better diagnosis of some clinical entities previously misdiagnosed as gastroesophagic reflux 2. Landres et al used the term eosinophilic esophagitis for the first time in 1978 3, being Attwood et al who described it as a new entity in 1993 4.
The disease is characterised by an intense infiltration of eosinophils in the esophagus mucosa. The main symptoms are dysphagia, abdominal pain and vomiting, and less frequently eating disorders and food impaction 1, which do not respond to antireflux treatment.
Its incidence is greater among the children population, males, with personal and family background of atopy, with proven food allergy 5. Recent studies have reported aeroallergens as possible trigger 6,7.
CASE REPORT
We report the case of a 37 year old male patient diagnosed of rhinoconjunctivitis with sensitisation to dust mite and grass pollen with a good evolution at present, with no food allergy symptoms, and requiring nasal topic corticosteroids and oral antihistamines occasionally. The patient had a history of gastroesophagic reflux (grade I/IV) and esophagitis since 2002, undergoing regular revisions by the Gastroenterology Service of our Clinic. The patient related dysphagia for solid foods, selflimited diarrhea episodes and intolerance to alcoholic drinks due to epigastric pain. He was treated with antiacid drugs, proton bomb inhibitors, prokinetics, as well as ansiolitics, without complete remission of the symptoms.
Two times (September 2002 and April 2004), the patient underwent endoscopy with biopsy which demonstrated the esophagus inflammation. The esophagic-manometry (April 2004), was normal, and the pharyngo-esophagic study, a showed lack of primary waves and contrast medium emptying by gravity.
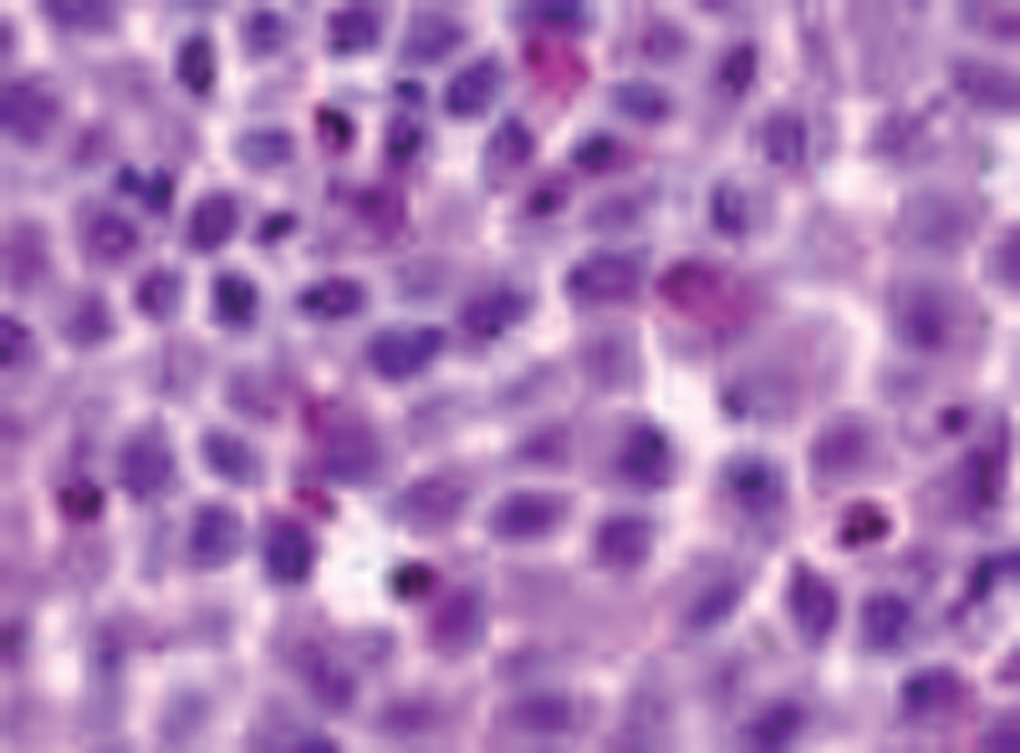
Due to the persistence of the symptoms, new manometry, gastroscopy (fig. 1) and biopsy (fig. 2) were performed in December 2004, resulting in motor esophageal dysfunction, bamboo like esophagus and multiple fibrin formations, with an anatomopathologic diagnosis of eosinophilic esophagitis. In January 2005, a study of food allergy is requested.

Figure 1.--Endoscopic study. December 2004. Whitish lesions of fibrinoid aspect, compatible with eosinophilic esophagitis.
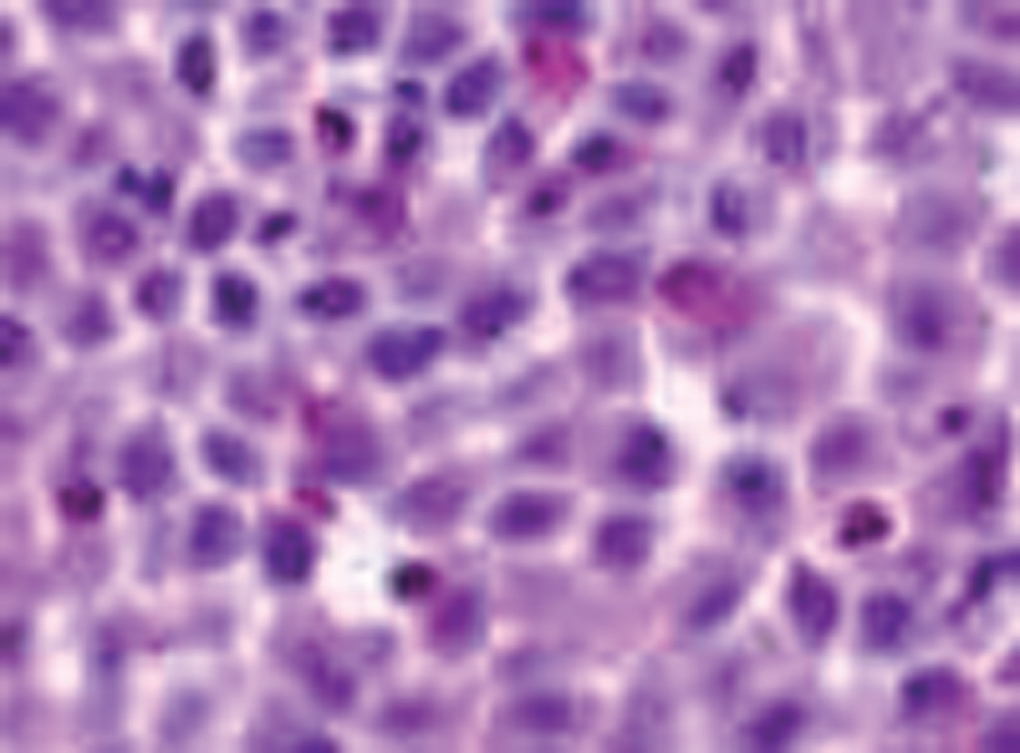
Figure 2.--Biopsy of esophagus mucosa (eosinophilic esophagitis). Infiltration of eosinophils is observed.
Allergic study
Skin prick test with the most frequent food and inhalant allergens (fish, shell-fish, nuts, legumes, wheat flour, egg, milk, dog and cat dander, Dermatophagoides pt, Alternaria, Aspergillus, grass pollen, tree pollen, weed pollen, olive pollen, cypress pollen, latex and Anisakis) and some rosacea fruits (almond, apple peel, apple pulp and pear). The known positivity to D pteronyssinus, grass and olive pollens is observed. Prick-prick test with egg white and yolk, milk and apple (peel and pulp) was also performed, being positive only to egg white (14 x 10 mm).
Total serum IgE was 95 kU/l, within normal range; specific IgE was 0.80 kU/l (class 2) to egg white and negative to egg yolk and apple. Histamine release test (basal 4.56 ng/ml; anti IgE 2.56 %; total histamine 41.10 ng/ml; egg white 20.51 %, egg yolk 23.08 %; apple 0 %), and basophil activation test (negative control 1.8 %; anti IgE 56.8 %; egg white 1st dilution 81.7 % and 2nd dilution 63.3 %; egg yolk 1st dilution 85.5 % and 2nd dilution 68.9 %; apple 1st dilution 8.3 % and 2nd dilution 3.5 %), were positive to egg white and yolk.
In the blood test, an increase of eosinophils since 2004 stood out, being at the moment of the revision the values 9.1 % (0.52 10E9/L) (fig. 3).
Figure 3.--Evolution of our patient's peripheral eosinophilia since 1998 to 2005.
With these results, the patient was diagnosed of eosinophilic esophagitis. He was recommended egg-free diet and treatment with montelukast, 10 mg/day, and Ketotifen, 1 mg/b.d. In April 2005 the symptoms had remitted, and the patient improved the weight and the alcoholic drinks were well tolerated.
DISCUSSION
The eosinophilic esofagitis is an increasingly diagnosed entity 1. Patients with symptoms of gastroesophagic reflux, dysphagia, vomiting or abdominal pain with no response to the treatment could be suffering from this disease 3-5. In its pathogenesis, mainly food allergens have been observed, although recently aeroallergens have also been involved 6,7. That is why it is important to perform an allergologic study by means of in vivo and in vitro tests. The food commercial extracts are obtained from their natural source by the extraction of the allergenic materials, and therefore there is a great variability in their composition. This, together with their instability due to the fact that their allergens are sensitive to the change of temperature, pH, and other factors, can make these extracts lose biological activity and false positive results can be reached in prick. We agree with other authors who state that the skin prick-prick test with natural food, technique recommended by Dreborg and Foucard for the first time in 1983 8, is more sensitive than the prick test performed with commercial extracts. Our patient did not relate symptoms with any food, but considering his history of rhinoconjunctivitis due to pollen allergy, prick with rosaceae fruits and prick-prick with apple were performed, with negative result. Because the patient's usual diet included milk and egg, prick with both commercial extracts was performed, with negative result, and prick-prick with whole milk, and egg white and yolk, with positive result to egg white. In order to confirm this finding, the in vitro test available in our Department, specific IgE, histamine release test and basophil activation test, were performed, being all of them positive to egg. With these results, and even though the patient did not connect his symptoms with eating egg, we decided to take it out of his diet and observe the evolution. Treatment with 10 daily mg of Montelukast and 2 daily mg of Ketotifen is also started. Some authors postulate that these clinical entities must be treated with daily maintained dosages of Montelukast 20-30 mg, since this treatment seems to be effective for the control of the symptoms in most patients and seems to be better than other treatments such as corticosteroids, antihistamines and inhibitors of the proton bomb, although more controlled clinical trials are still necessary 9. In our case, and considering the good clinical evolution of the patient with the egg-free diet and the treatment, we did not consider necessary to increase the dosage of Montelukast.
In our opinion, the clinical remission obtained after eliminating the egg from the diet confirms the important etiological role played by the egg proteins in this disease and the importance of performing an allergological study in these patients.
Finally, we emphasise the usefulness of new in vitro techniques, such as the basophil activation test, in the diagnosis of the allergologic diseases 10.
Correspondence:
Judith Antón Remírez
Department of Allergology and Clinical Immunology
University Clinic of Navarra
Apartado 4209
31080 Pamplona. Spain.
E-mail: janton@unav.es
