


Introducción: En México, la prevalencia de sobrepeso y obesidad en escolares es del 34.4% (ENSANUT 2012). Esta puede inducir un círculo vicioso ‘‘pie plano-plantalgia-sedentarismo-obesidad’’. Sin embargo, la presencia y grado de pie plano en escolares con obesidad no se ha descrito en la población mexicana. El objetivo del estudio fue determinar la prevalencia de pie plano y su asociación con obesidad en escolares de Tamaulipas, México.
Métodos: Se realizó un estudio analítico, transversal con 1,128 escolares de 9 a 11 años de edad, de los cuales el 48.8% correspondió al sexo masculino (H) y el 51.2% al femenino (M). Se realizaron mediciones antropométricas (peso, talla, perímetro de cintura y cadera). Se calculó el índice de masa corporal (IMC) y se consideró como obesidad cuando el IMC fue mayor del percentil 95. Se fotografió la huella plantar por medio de un podoscopio, utilizando la clasificación de Denis para diagnosticar los grados de pie plano.
Resultados: La prevalencia de sobrepeso-obesidad fue del 49.1% y de pie plano fue del 12.1% (H: 8.1%, M: 4%; p = 0.28). La asociación entre obesidad y pie plano fue significativa (p <0.001) y con un riesgo 2.5 veces mayor en los niños con sobrepeso-obesidad en comparación con los de peso normal.
Conclusiones: Existe una asociación entre la obesidad y el pie plano, por lo que se sugiere implementar medidas de prevención secundaria en la población.
Background: In Mexico, the prevalence of overweight and obesity is 34.4% in school-age children (ENSANUT 2012), which may induce a vicious cycle of flatfoot-plantalgia-sedentarism-obesity, although the presence and degree of flatfoot in school-age children with obesity has not yet been described in a Mexican population. The objective of the study was to determine the prevalence of flatfoot and its association with obesity in school-age children living in Tampico.
Methods: An analytical and cross-sectional study with 1128 students, 48.8% male and 51.2% female, 9- to 11-years of age. Anthropometric measurements (weight and height) were performed. Body mass index (BMI) was calculated and obesity was considered a BMI percentile > 95. Plantar footprint was photographed via a podoscope using Denis classification to diagnose flatfoot grades.
Results: The prevalence of overweight/obesity was 49.1% and of flatfoot was 12.1% (male: 8.1%, female: 4%, p = 0.28). The association between obesity and flatfoot was significant (p < 0.001) and there was a 2.5 times higher risk of overweight-obese children compared to those of normal weight.
Conclusions: There is an association between obesity and flatfoot. We suggest implementing secondary preventive measures in this population.
1. Introduction
Obesity is considered to be the epidemic of the 21st century. It can begin during infancy and is considered to be a serious public health problem, both in developed countries as well as in developing countries.1,2 The World Health Organization (WHO) calculates that for the year 2015 there will be ~2,300 million overweight adults and > 700 million who are obese, in addition to 42 million overweight pre-school children. Mexico ranks fourth in global prevalence of childhood obesity, with ~28.1% of boys and 29% in girls. It is surpassed by Greece, U.S. and Italy.3
Childhood obesity is defined as abnormal or excessive fat accumulation with respect to age and gender that is harmful to health. According to the National Survey of Health and Nutrition 2012 (2012 ENSANUT), Mexico has a prevalence of overweight and obesity in 5- to 11-year-old school-age children (19.8% and 14.6%, respectively, 34.4% in total). The first place in obesity is in the state of Campeche with 23.2%. On the other hand, the states of Chiapas and San Luis Potosí presented the lowest frequencies of overweight and obesity. The state of Tamaulipas occupies fourth place with prevalence of overweight and obesity of 18.6 and 20.3%, respectively (38.9% total).4
Among the functional anatomic modifications caused by obesity is flatfoot, which is a set of alterations in the elasticity of the ligaments because the bone structure loses the interarticular relationship between the hind foot and the mid-part of the foot, causing a muscular imbalance that is observed from 30 months of age. It is generally classified into two types: 1) physiological flatfoot (flexible, hypermobile or soft), which presents itself in children < 6 years, is asymptomatic and is of greater prevalence; and 2) pathological or hard flatfoot, which manifests itself between the 6 to 12 years of age and presents plantar pain.5-7
The presence of pathological flatfoot is modified according to age due to several factors such as the maturation of osteoligamentous structures, laxity of ligaments, over-weight-obesity and adipose package on the plantar side of the foot.5,7-9 However, obesity causes a vicious cycle in which plantar pain makes it difficult to abandon the sedentary lifestyle. In turn, children tend to progressively have increase in weight with little participation in sports which, in turn, impedes weight loss, favoring the presence of flatfoot.7,10
The purpose of the present study was to determine the prevalence of flatfoot and its association with overweight/ obesity in school-age children of the city of Tampico, Tamaulipas, Mexico.
2. Methods
2.1. Study subjects
A cross-sectional analytical study was conducted. It was carried out in 14 primary public schools of the city of Tampico, Tamaulipas randomly during the months of January to May 2014. It included a sample of 1128 children of both genders from 9 to 11 years of age. Excluded from the study were students with spinal diseases, walking disorders and alterations of the lower extremities including orthopedic diseases other than flatfoot (valgus foot, pes equinus, club foot, pes cavus, etc.). Also excluded were students whose parents refused their children’s participation in the study. The study was approved by the ethics committee of the Faculty of Medicine of Tampico, Autonomous University of Tamaulipas (registry number FMT-SA-008/11). Information about the study was provided to the parents, participating children and school authorities. Parents provided written informed consent authorizing their child’s participation in the study. The variables taken into consideration were age, gender, weight, height, waist and hip diameters, body mass index (BMI), waist-hip ratio (WHR), waist-height index (WHI) and the Denis classification for flatfoot.
2.2. Characteristics, anthropomorphic measurements and evaluation of pes planus of the population
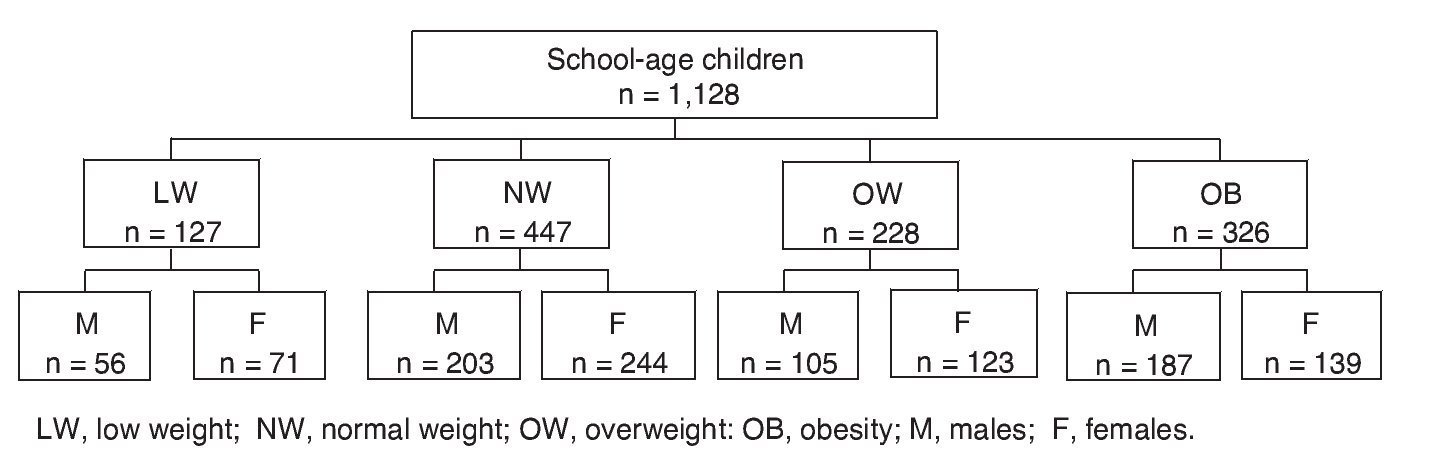
Anthropomorphic measurements were carried out (weight, height, waist and hip diameters) by conventional methods and standardized by researchers trained for data collection. BMI was calculated using the Quetelet index [weight in kilograms divided by height in meters squared (kg/m2)], WHR (ratio of waist/hip measurement), and WHI (waist/height in centimeters). Subsequently, measurements were classified by groups—with percentile tables of BMI for gender and age of the World Health Organization 2007—as low weight (LW) < 5, normal weight (NW) 6-84, overweight (OW) 85-94 and obesity (OB) > 95 (Figure 1).
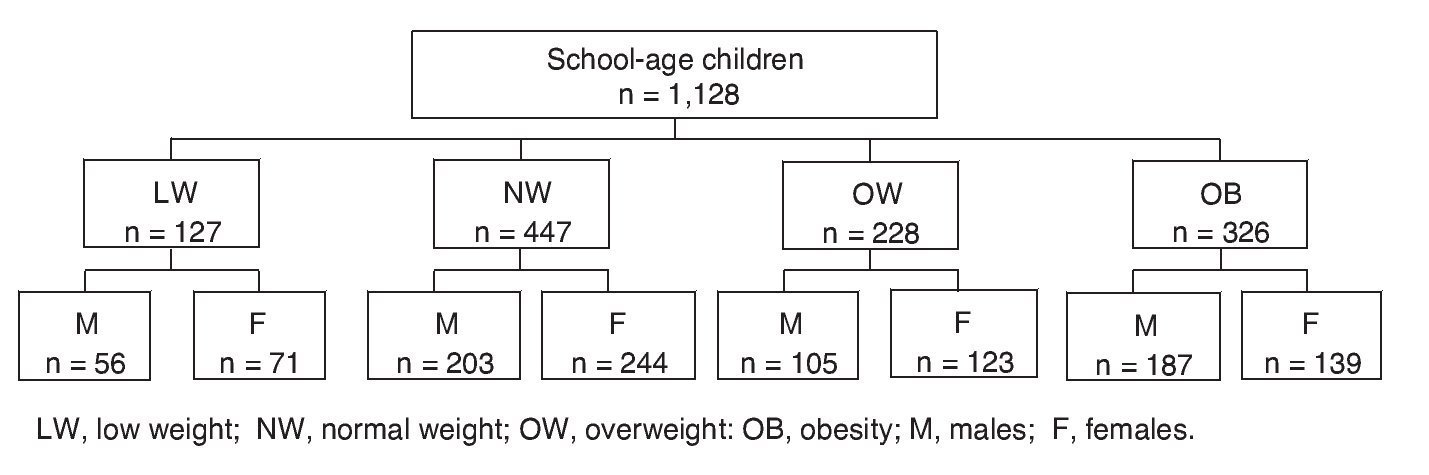
Figure 1 Study population with distribution by groups according to body mass index and gender.
For diagnosis of pes planus, the student was placed without shoes on a classic wooden podoscope (60 x 40 x 40 cm) and the position of the shoulders, pelvis, knees and feet was evaluated. The test of extension of the first toe of the foot (Jack) was done; this maneuver allows for observation of the internal longitudinal arc in a flexible pes planus. Next, a photograph of the footprints was taken with the weight being distributed to both feet. Clinical evaluation of the pedigraph was done by a trauma physician and orthopedist. The plantar print was classified according to Denis into three degrees of pes planus: Grade 1, the support of the lateral border of the foot is half of the metatarsal support; Grade 2, the support of the central and front areas are equal; and Grade 3 in which the support in the central area of the foot is greater than the width of the metatarsal support.11
2.3. Statistical analysis
Data are represented by the mean 6 standard deviation (SD) with 95% CI. Statistical analysis was done with the SPSS v.20 and GraphPad Prism 6 packages. Frequencies were determined and for group comparison the ANOVA test was used with Dunnett post hoc test (considering the NP group as control). For the association between variables, pes planus-obesity and grade of pes planus-obesity, χ2 test was applied as well as for the calculation of risks (odds ratio of ORP prevalence) between the OB group and NP group; p < 0.05 with 95% CI was considered statistically significant.
3. Results
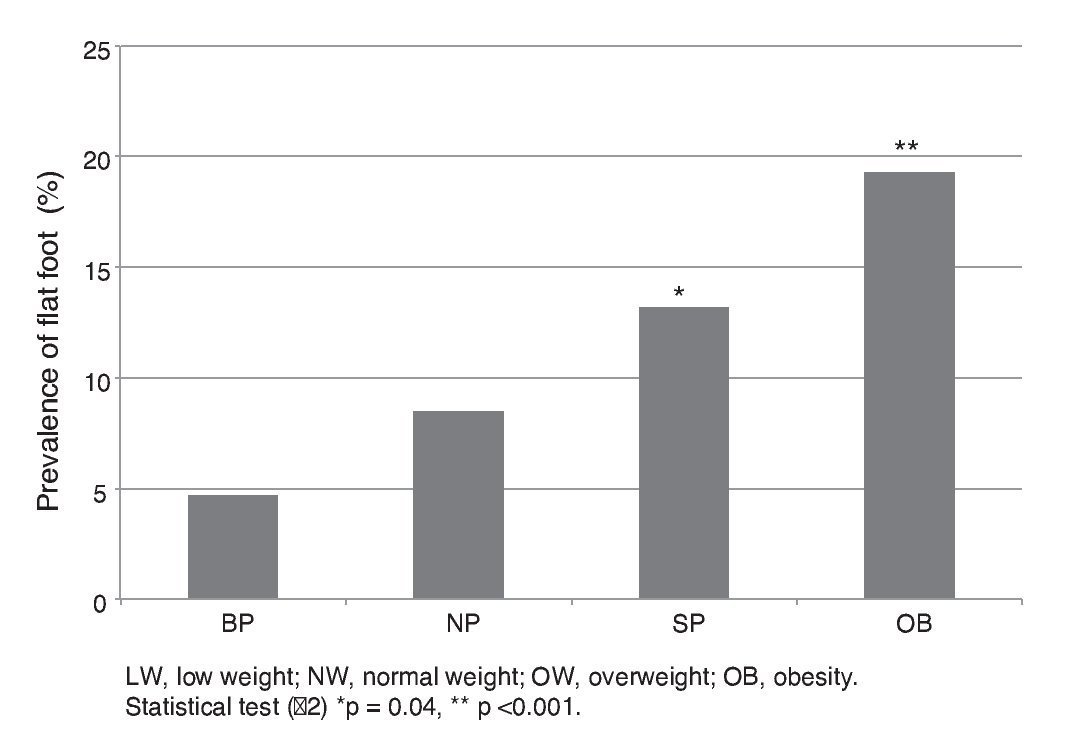
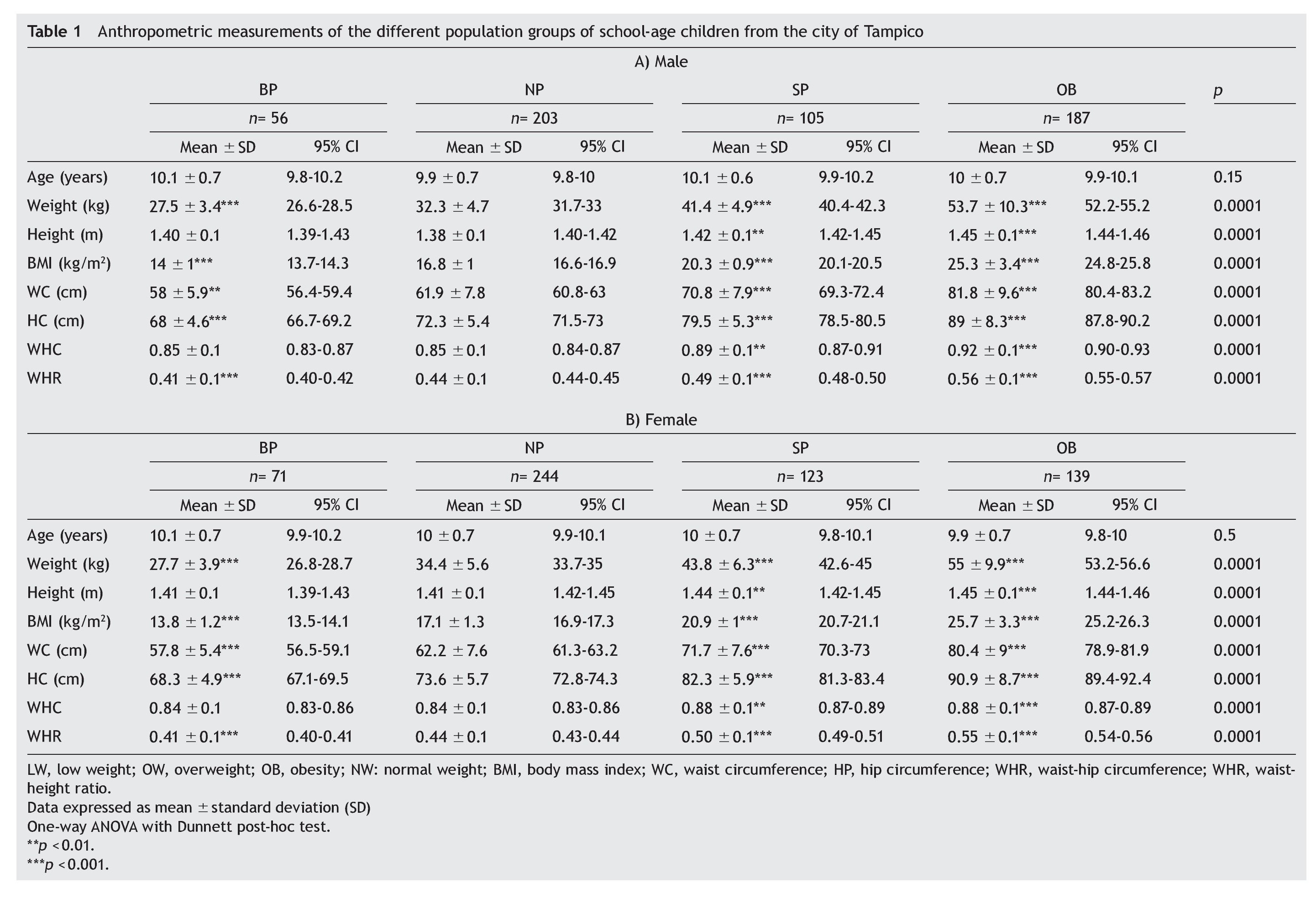
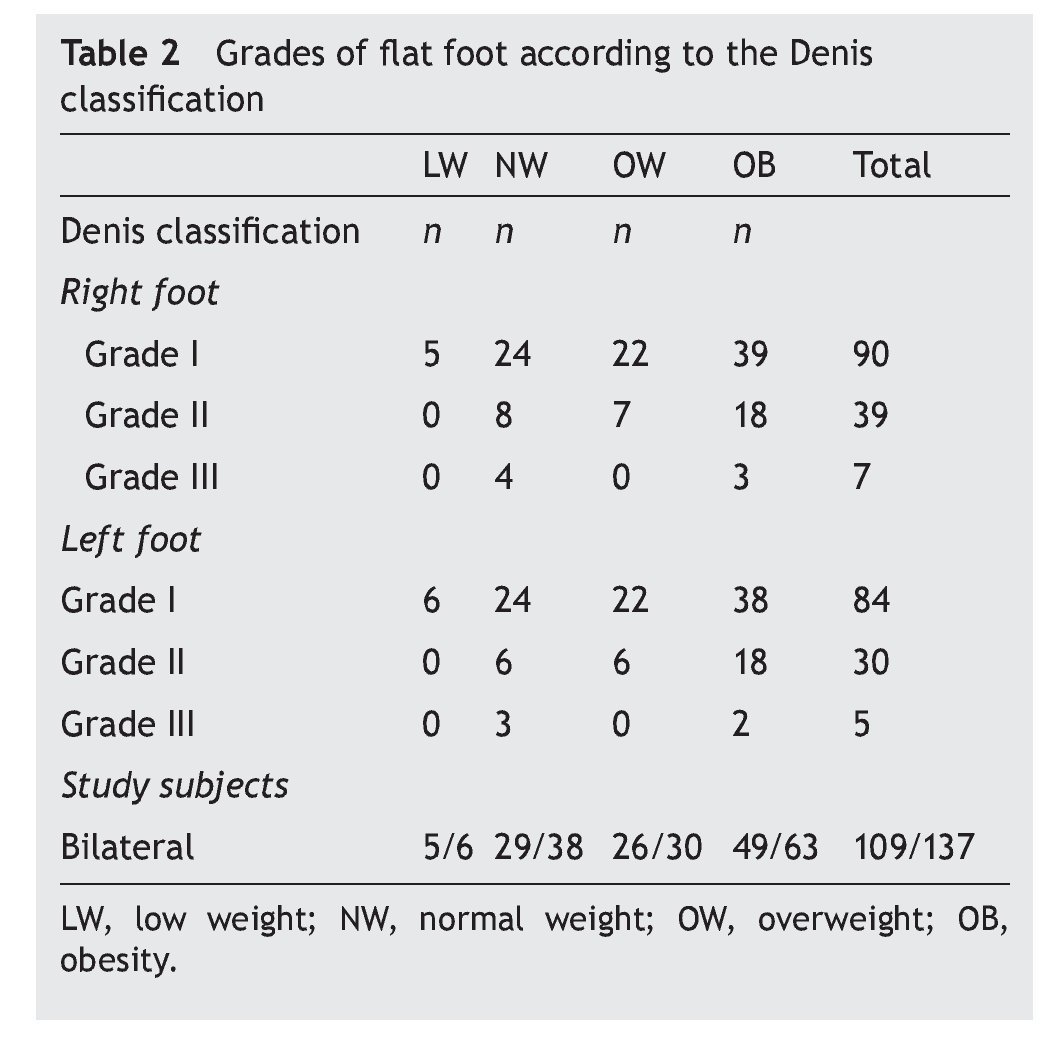
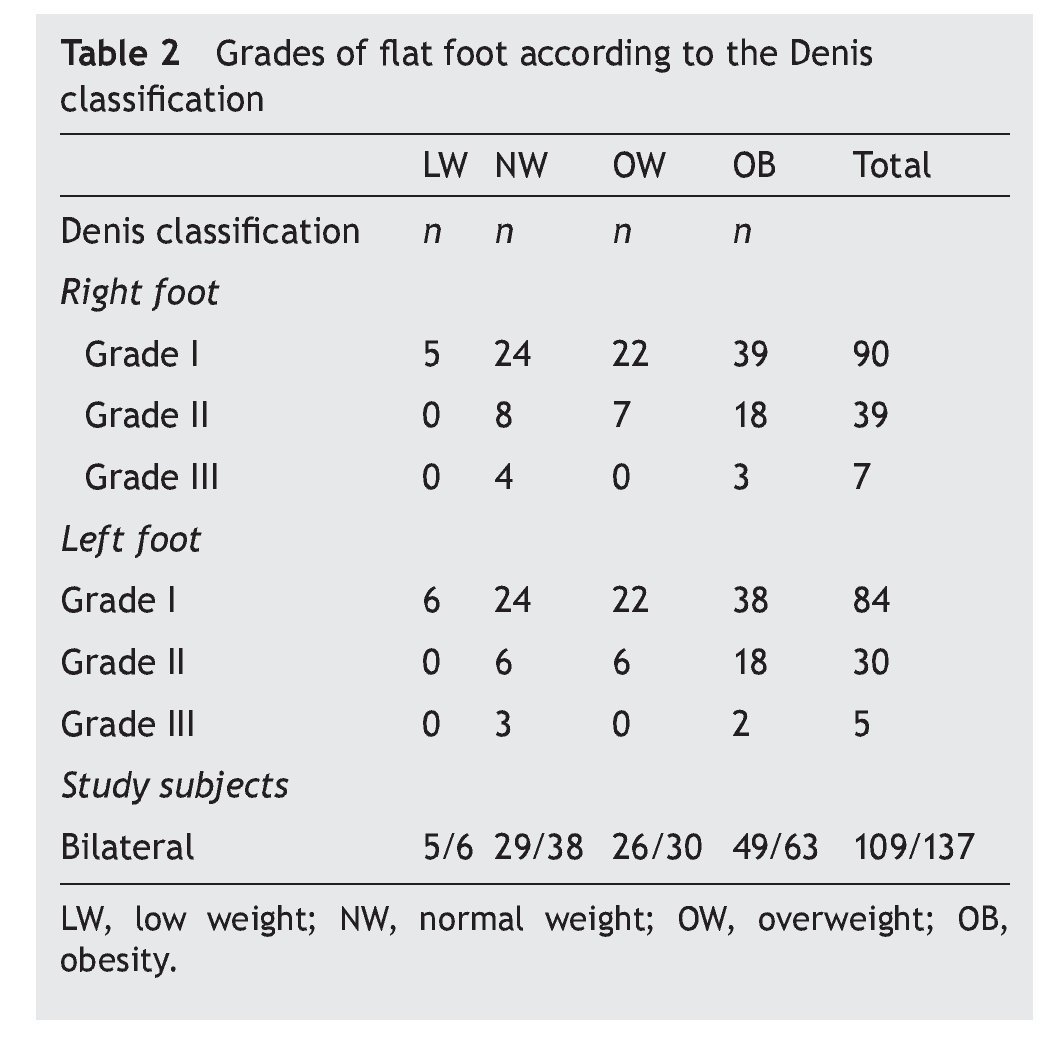
The sample was comprised of 1128 students, 551 males (M) and 577 females (F) (51.15%). Mean age was 10.02 6 0.7 years; p = 0.15 (M) and p = 0.50 (F). Study groups were classified according to BMI and the calculation of prevalence in SP and OB was obtained (20.2 and 28.9%, respectively, total 49.1%). Anthropometric measurements are shown in Table 1. With regard to the results of pes planus, the general prevalence was 12.1%, higher in males than in females (M: 8.1%, F: 4%; p = 0.28) up to the age of 10 years (14.9%), without difference in prevalence rates with respect to age (p = 0.74). The frequency of pes planus in the four study groups is shown in Figure 2. The OB group had the greatest frequency (19.3%) (Figure 3). The association between obesity and pes planus was significant (p < 0.001). Odds ratio (OR) for pes planus of the OB group compared with the NP group was 2.5 (95% CI 1.6-3.9; p < 0.001). Distribution of the grades of pes planus in the different groups is shown in Table 2. In the population with pes planus there was bilateralism in 109 cases; grade I was observed with greater frequency, 90 cases in the right foot and 84 in the left foot, predominating in the OB group. An association between the grades of pes planus and obesity was observed (p < 0.0001).
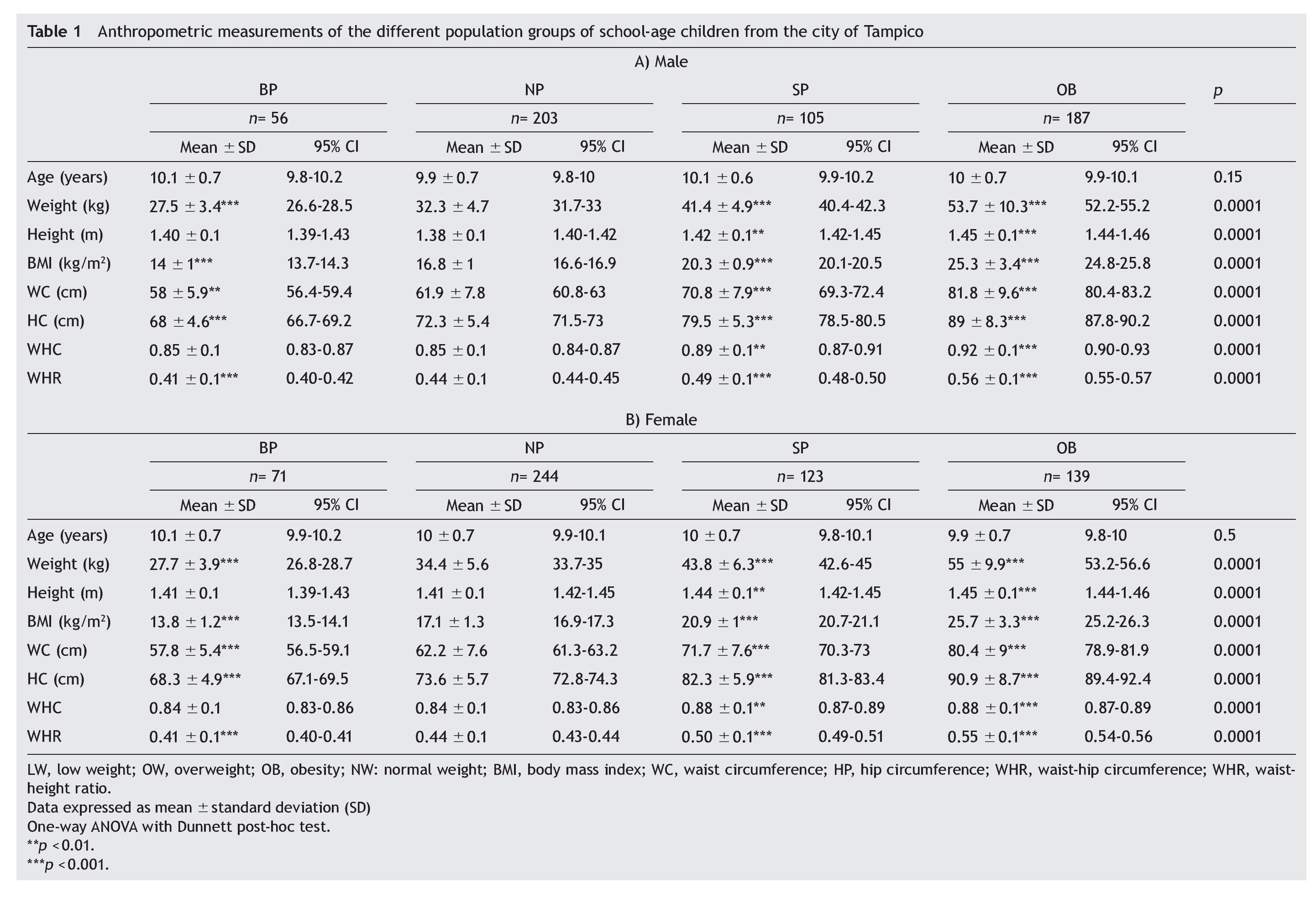
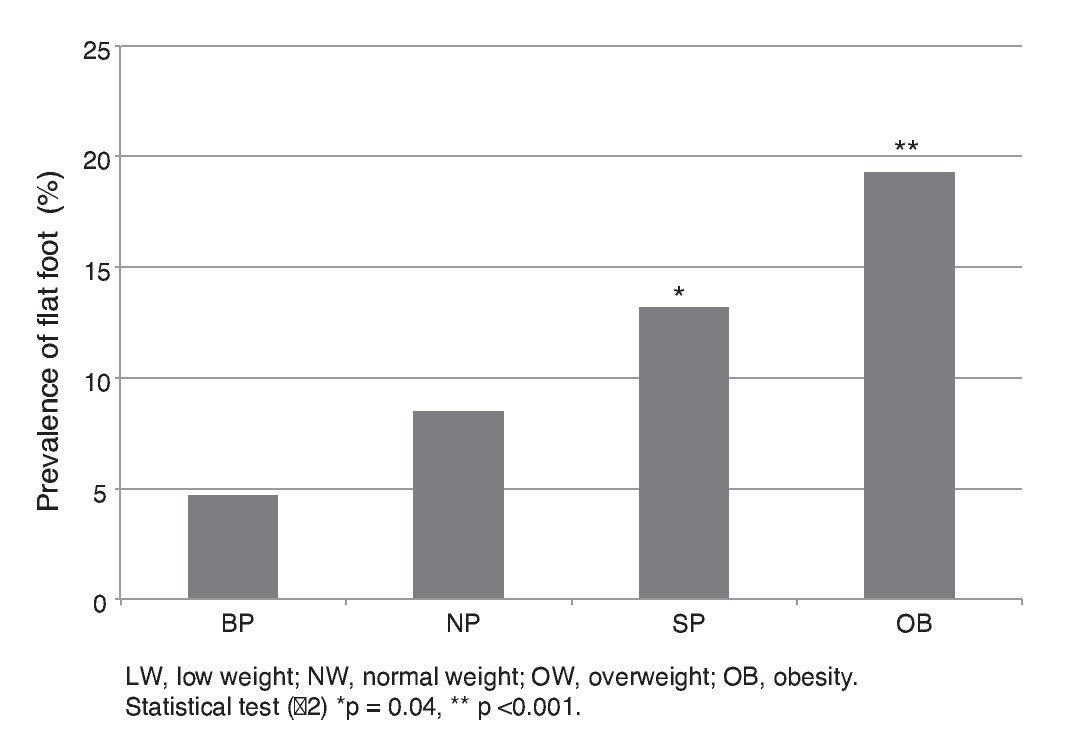
Figure 2 Prevalence of pes planus in the different groups.
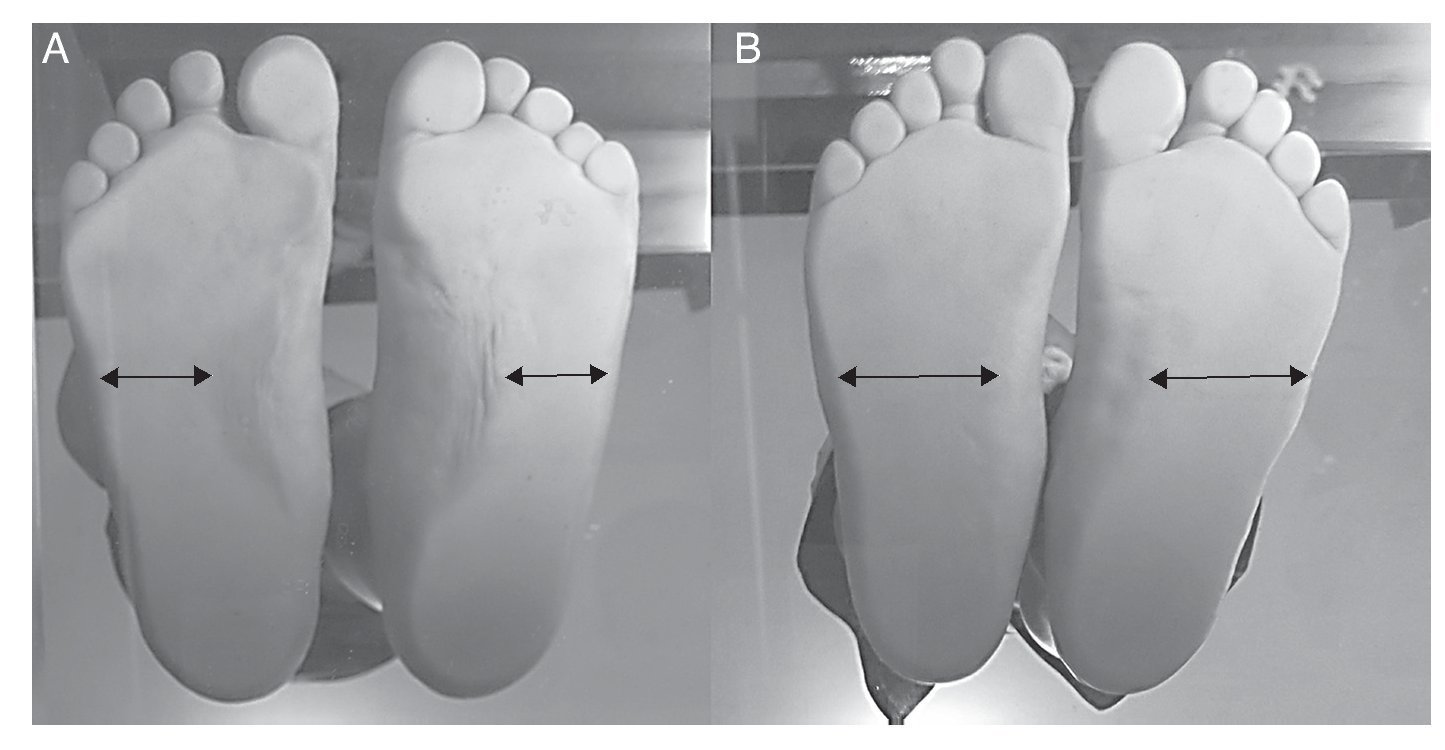
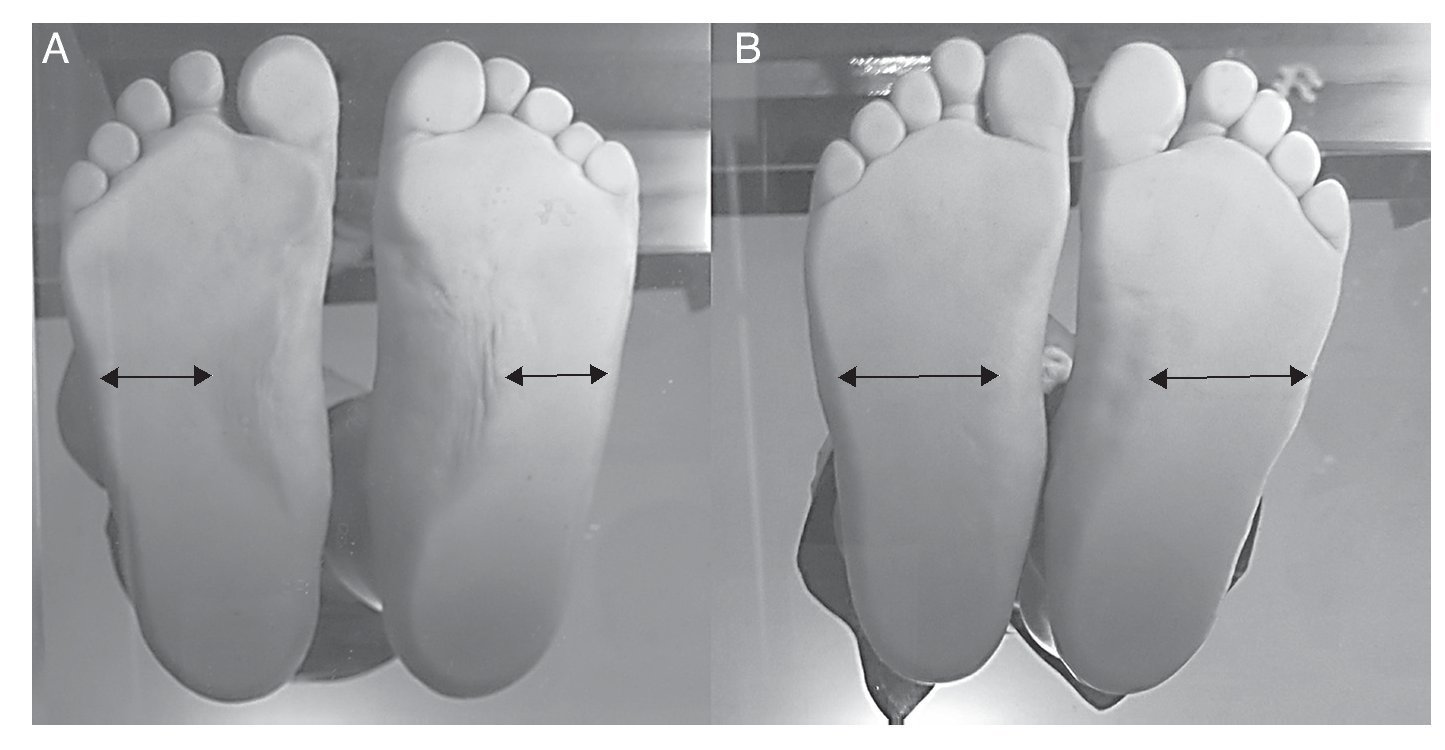
Figure 3 Representation of a footprint of a student with normal weight (A) and pes planus grade II of the Denis classification of an obese student (B).
4. Discussion
In Mexico, the reference survey in regard to population nutrition is the ENSANUT. However, data are reported every 6 years. In 2012, ENSANUT reported that for the student population (5-11 years of age) the combined national prevalence for overweight and obesity was 34.4% (19.8 and 14.6%, respectively), indicating that these
ures have not increased in the last 6 years. It should be mentioned that the ENSANUT 2012 also reported data according to federal entity. In Tamaulipas, the reported increase was 10.2 pp. However, in this study, the regional prevalence combined of SP and OB was 49.1% (20.2 and 28.9%), with an observed increase of 14.7 pp. It should also be mentioned that the study population was urban. When the results of this study are compared with the ENSANUT Tamaulipas 2012, which reported a decrease of 2 pp for overweight and 1.4 pp for obesity during the period 2006-2012, this contradicts an increase of 2.1 pp for overweight and 8.4 pp for obesity. However, it needs to be reinforced that this study was carried out 2 years later.
The increase in obesity in the population will have health consequences for biopsychosocial development as well as for the socioeconomic structure of the country. Costs generated due to the complications of obesity, such as type 2 diabetes mellitus type, represent 15% of overall health expenses.12
The identification of a school-age child with overweight and especially with obesity commonly involves the use of preventive measures for short-, medium- and long-term complications. Nevertheless, in conventional clinical practice, these measures are geared towards metabolic disorders. However, other complications exist such as psychological and structural. Among the structural complications is identification of pes planus, which should be carried after 6 years of age because before that physiological pes planus may be present. In addition, at this age the maturation of the median longitudinal arch concludes.13,14 For this reason, in this study it was opted to include students 9 to 11 years of age when maturation of the plantar arch is complete, thereby avoiding false positive results. Together with this, the Denis classification was chosen for the diagnosis as it is adequate for school-age children as well as to clinically differentiate the grades of pes planus.5
In this study, an overall prevalence of pes planus of 12.1% in the study population was demonstrated, lower with respect to the results of Pfeiffer et al. who reported a frequency of 44%.13 However, the percentage was high compared with that reported by García-Rodríguez et al. (2.7%).15 This disparity in percentages could be due to differences in age, ethnicity and pes planus classification used in these studies. 16 It should be noted that the prevalence of pes planus in obese school-age children was 19.3% in our study, which was 3 pp higher compared with the frequency reported by Bordin et al. where a similar study design was considered.17
In regard to gender, the frequency of pes planus was greater in males. This variation has been reported by different authors,13,17,18 although its etiology is not clear. Based on the results of the present study, this event cannot be attributed to obesity as its cause because the frequency of obesity was similar in both genders.
The prevalence of pes planus increased with BMI and was greater in the OB group as well as the fact that the association between these variables was significant. These results are consistent with the conclusions by Dowling et al. who studied a similar population.19,20 The classification of pes planus observed in this study must be highlighted where grades I and II were greater in the OB group and the number of cases of grade III was lower. However, grade III was present in the NP group. This could be due to genetics playing an important role in the presentation of pes planus, and the fact that epigenetics of the individual prevents or induces its appearance and development.7,13
In conclusion, it was established in the present study that the presence of overweight and obesity was associated with the appearance of pes planus in a population of school-age children. The results suggest that male gender is a risk factor for developing this alteration. It is suggested that studies in overweight and obese school-age children be carried out to evaluate for collateral disorders and to evaluate the long-term consequences. Implementation of secondary preventive measures is suggested for this population to avoid medium- and long-term complications that affect the physical and occupational life of these individuals.
Conflict of interest
The authors declare that there are no conflicts of interest related to this study.
Acknowledgments
The authors extend their appreciation to Dr. Enrique Álvarez Viaña and Dr. Leticia Manuel Apolinar for their invaluable help with this project.
Received for publication: 12-4-14;
Accepted for publication: 2-3-15
http://dx.doi.org/10.1016/j.bmhimx.2015.02.003
Correspondence:
Dr. Pedro Pérez Rodríguez
E-mail:investigacionmedicinauat@gmail.com