


One of the most common congenital disorders that affect the face structures is the cleft lip palate (CLP). The aim of this study was to obtain the clinical-epidemiological profile of CLP patients from Hospital de Especialidades del Niño y la Mujer (HENM) Dr. Felipe Nuñez Lara, at Queretaro, Mexico, from 2011 to 2014. To provide interdisciplinary treatments for CLP patients based on the information from the pediatric records registered in that period.
MethodsRetrospective, cross-sectional, observational study using univariate analysis frequencies for qualitative variables; central statistical and dispersion for quantitative variables and clinical profile. One hundred records were reviewed, from which 15 were excluded for being syndromic cases. Epidemiological, clinical, and socio-demographic variables were studied.
ResultsThe epidemiological profile (variables associated with pregnancy, patient's health at birth, nutritional and psychomotor development, family medical records, and socioeconomic factors) and the clinical profile (disease classified by sex, structure, and affected side, surgeries classified and order in which they took place) of the treated population are presented.
ConclusionsThe results showed the need to standardize data registration on medical records for improved monitoring and treatment of patients and emphasize actions to maintain a low incidence of CLP in Queretaro.
El padecimiento de labio paladar hendido (LPH) es una de las alteraciones congénitas más comunes que afecta las estructuras de la cara. El objetivo de este trabajo fue generar el perfil epidemiológico y clínico de la población con LPH atendida en el Hospital de Especialidades del Niño y la Mujer (HENM) “Dr. Felipe Núñez Lara”, de la Secretaría de Salud del estado de Querétaro, México, en el periodo de 2011-2014, a través de la Clínica de Labio Paladar Hendido, para brindar tratamientos interdisciplinarios a los pacientes con esta afección con base en la información de los expedientes registrados en el periodo mencionado.
MetodologíaEstudio observacional, transversal, retrospectivo usando análisis univariado con frecuencias para variables cualitativas; estadísticas centrales y de dispersión para variables cuantitativas y perfil clínico. Se revisaron 100 expedientes, descartándose 15 por ser de casos sindrómicos. Las variables estudiadas fueron: socio-demográficas, epidemiológicas, y clínicas.
ResultadosSe presentan los perfiles epidemiológicos (variables relativas al embarazo de la madre y salud del paciente al momento de su nacimiento, desarrollo nutricional y psicomotor; antecedentes heredo-familiares y presencia de adicciones; datos socio-económicos familiares) y clínicos (clasificación del padecimiento por sexo, estructura y lado de afectación; clasificación de las cirugías y orden en que se efectuó el procedimiento) de la población considerada.
ConclusionesLos resultados del estudio muestran la necesidad de estandarizar el registro de datos en expedientes para mejorar el seguimiento y tratamiento de los pacientes y enfatizar en acciones preventivas que permitan mantener la baja incidencia del LPH en Querétaro.
Cleft lip palate (CLP) is among the most common congenital disorders affecting structures of the face.1 It can involve both soft and bony tissues, from the lip area to fissures that communicate the oral cavity with the nasal cavity, and affect the ear and eyes. In the case of palatine fissures, the patient presents with feeding and breathing difficulties, phonatory problems, lack of development of the alveolar processes, dental problems of form, number and eruption that affect not only the infant's teeth but also compromise the adult's teeth.
There are different classifications in the literature to designate the disease: when referring to the involved structures in development, it is classified as complete palatine cleft with lip involvement, cleft in the anterior palate (only limited to the anterior fossa) where the lip may be involved, cleft palate on the back (behind the pit) and submucous cleft, including a fissured uvula.2 There is another designation frequently used in surgical procedures to identify bone defects called the “Y” of Kernahan, which forms three zones. In these areas, the union is the origin of the primary palate, upper areas represent the right and left sides, and the bottom corresponds to the palate.3 Another way to classify CLP is using the exposed anatomy: by compromising the lip (CL), it is named unilateral (right or left) or bilateral; incomplete or complete if it involves nasal tissues (cleft lip and lip fissure); cleft palate (CP) complete or incomplete (one - third or two - thirds) or CLP when the condition involves palate and lip, and unilateral or bilateral cleft alveolus palatal lip.4
Patients need to receive immediate attention and integrated treatments (IT) to survive because, from the moment they are born, they are exposed to different health and infectious complications that other children their age would not present.5–7 Therefore, it is important to decrease and prevent oral and systemic diseases, as well as the formation and development of dental arches to produce an occlusion that achieves the good function of the stomatognathic apparatus. Another problem faced by both the patient and his parents throughout their lives is social integration.
Internationally, the daily intake of folic acid in doses of 400mg/day, especially three months before pregnancy until the twelfth week of gestation was established as a preventive measure.1,8 In Mexico, the Ministry of Health (MH) developed a handbook for patient care including preventive procedures, management, treatment and rehabilitation of children with CLP.4
Recognition of this condition at an intrauterine stage is very useful to the interdisciplinary team to minimize complications during childbirth and plan the need for surgical treatments, as well as for parents, to receive pre-delivery education. Thus, the nutritional status of the newborn, which may interfere with the development and growth as a result of insufficient suction, the presence of milk in the nasal cavity, aspiration and the small amount of food intake, would not affect his survival.1,2,9–12
Another challenge is to address the psychological impact for the parents when they are informed that their child has the condition.13,14 Timely actions reduce the time of treatment required for the patient to acquire the proper functionality and development of the affected structures.
Once the disorder is present, the goal is, for any patient with CLP not to know that he or she has been born with the condition. This can only be achieved with immediate attention at an early age, to stimulate the patient's development and the correction of the affected structures by bringing the displaced segments into place and shaping the nasal deformity through orthopedic treatments, including different surgeries and the combination of treatments.3,15–17
In most cases of CLP, injuries can be solved favorably by treating the involved structures in the condition to restore their functions. The treatments are given by a team of specialists, including plastic surgeons, orthodontists, dentists, otolaryngologists, speech therapists, psychologists, ophthalmologists, and pediatricians, who must be present throughout the entire process.
At the HENM, the Comprehensive Care Program for Prevention and Health Care (CCPPHC) dependent of the Health Care Services of the state of Queretaro is followed.18 Its purpose is the management of healthcare of the different disabilities of the population. This program, among others, has the CLP clinic where, due to the complexity of the injuries, the participation of a multidisciplinary team is necessary to establish the treatment plan according to the stage of development, restore the appropriate functionality and improve patient's quality of life. This hospital meets the needs of the population of the state that has no other type of social care.
The reported cases of CLP, although they are few in comparison with other problems faced by health institutions, are part of the medical and social problems of Mexican children, so it is necessary to carry out more research to decrease of its prevalence.
The prevalence of CLP for different human populations in non-syndromic isolated cases is 70% with lip and palate involvement, and 50% involving only the palate.19–22
Worldwide, the highest prevalence of CLP occurs in the Asian race and Native Americans (1/500); the Caucasian population has an average prevalence (1/1000), and the lowest is in the African population (1/2500).2,23
The cases of CLP in the state of Queretaro as reported by the HM, and according to the reported births show a prevalence of 0.33, 0.38 and 0.41 per 1000 cases in 2011, 2012 and 2013, respectively. An increase can be observed during this period.24,25
In 2009, the CLP was ranked first, with an incidence of 1.1 to 1.39 per 1000 live births in Mexico;1 among the risk factors that caused this illness, social, economic conditions and certain ethnic groups were found.1,20,26,27
In an ecological study of CLP associated with socio-demographic and socioeconomic factors and pollution, which was carried out in Mexico City between 2003-2009, it was reported at the national level, one case in every 1000 births.1
The prevalence of CLP reported from 2011 to 2013 in Mexico was of 0.59, 0.56 and 0.60 per 1000 live births, respectively. At the state of Queretaro, for the same period, it was 0.33, 0.38 and 0.41 per 1000 live births, respectively.28
The nationally reported incidence rates for 2011 and 2012 were 0.82 and 0.62 (per 1000 people), and for 2013, 1.26 (per 100,000 people). The highest rates were found at the states of Hidalgo and Jalisco. For the state of Queretaro, during the same period were 0.44, 0.43 (per 1000 people) and 0.87 (per 100 000 people), respectively, confirming an increase of this condition.25,28
Therefore, it is essential to have studies that systematize the available information and allow identifying and addressing the recurring problems of the population that demand these services. Considering the socioeconomic and cultural diversity that characterizes Mexico, the collection of data by geographical area is an urgent task to know the incidence of the disease, its evolution, and magnitude, since this information is not available, and to guide the campaigns of promotion and prevention measures.
The data obtained in this research allows us to know the epidemiological and clinical profile of the population that presented this disease and was treated at the HENM, in the city of Queretaro from 2011 to 2014. These data respond to the following objectives:
- -
Determine the characteristics of the cases with CLP in the HENM.
- -
Identify the known risk factors in patients with CLP in the HENM.
- -
Get the spectrum of affection of the patients with CLP in the HENM.
- -
Characterize the different surgical treatments carried out in patients with CL, CP, and CLP at the HENM.
A descriptive, observational, and retrospective study was conducted. We used univariate analysis with frequencies for qualitative variables, central and dispersion statistics for quantitative variables and bivariate analysis of the association between qualitative variables and clinical profile.
To carry out this research, authorization was obtained from the Research Committee and the corresponding authorities from the Universidad Autónoma de Querétaro and the Ethics Committee of the HENM; once authorized, the records of patients with CLP who went to the Pediatric Consultation of the CLP Clinic and who received treatment during 2011-2014 were reviewed.
One hundred and one files were reviewed. Fifteen cases were excluded because they were syndromic cases, and one because of misdiagnosis. A total of 85 cases were studied, 58 (68%) male and 27 female (32%).
Patient registration was based on the mother's surnames, in the case of newborns, and based on the patient's paternal and maternal surnames when enrolling them in the institution, which sometimes resulted in duplicate records (once detected, duplicity was eliminated).
Based on the pediatric clinical history obtained at the HENM, a registration form divided into two sections was designed for this research: the first section, for the registration of the epidemiological profile, and the second, for the clinical profile.
Epidemiological and clinical variables were recorded. To establish the epidemiological profile, records were reviewed, and the information corresponding to the variables of interest was recorded. For the clinical study, we assessed the surgeries to which the patients were subjected. In both cases, the information was recorded in the respective data collection sheet.
The review of the records was made from the first to the last note. The information was captured on the record sheets as it was found, and was transcribed to the database once the file review was completed. To do this, we used the program Excel 2011 for Mac version 14.4.1 (140326). Subsequently, the information was analyzed using the following statistical procedures:
- •
Univariate analysis, with frequencies for qualitative variables and distribution of frequency, measures of central tendency and dispersion for quantitative variables.
- •
Because only scarce data was found in the clinical records, the total number of cases in which information was found was considered as a base. We calculated the percentage of the absence of data, except where three variables were analyzed; in these cases, the total population was considered.
- •
For the psychomotor development variable, we calculated the average of each skill according to the clinical history due to the absence of data about psychological and motor development in the reviewed files.
The results obtained from the analysis of the data that were collected to define the epidemiological and clinical profile of the 85 cases considered in the study are presented.
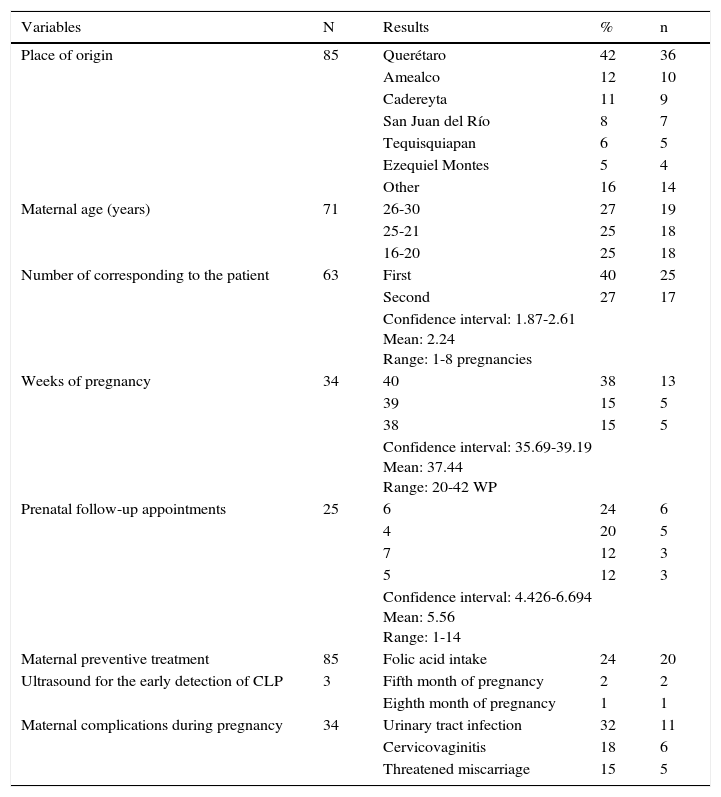
3.1Epidemiological profileTable 1 shows the data of the mothers of patients with CLP seen at the HENM during 2011-2014. The place where the majority of them came from (42%) was tehcity of Queretaro; the dominant age group was between 16 and 30 years (77%), and the majority of the patients were the product of the first pregnancy of their mother (40%). Pregnancy lasted 40 weeks (38%) in the majority of the cases. The highest percentage of prenatal follow-up had a variation of three to six consultations, and in only three cases (3.5%) an early detection of the disease was achieved. Folic acid intake as a preventive treatment during pregnancy was observed in only 24% of the studied cases.
Variables related to the patient's mother with cleft lip and palate.
| Variables | N | Results | % | n |
|---|---|---|---|---|
| Place of origin | 85 | Querétaro | 42 | 36 |
| Amealco | 12 | 10 | ||
| Cadereyta | 11 | 9 | ||
| San Juan del Río | 8 | 7 | ||
| Tequisquiapan | 6 | 5 | ||
| Ezequiel Montes | 5 | 4 | ||
| Other | 16 | 14 | ||
| Maternal age (years) | 71 | 26-30 | 27 | 19 |
| 25-21 | 25 | 18 | ||
| 16-20 | 25 | 18 | ||
| Number of corresponding to the patient | 63 | First | 40 | 25 |
| Second | 27 | 17 | ||
| Confidence interval: 1.87-2.61 Mean: 2.24 Range: 1-8 pregnancies | ||||
| Weeks of pregnancy | 34 | 40 | 38 | 13 |
| 39 | 15 | 5 | ||
| 38 | 15 | 5 | ||
| Confidence interval: 35.69-39.19 Mean: 37.44 Range: 20-42 WP | ||||
| Prenatal follow-up appointments | 25 | 6 | 24 | 6 |
| 4 | 20 | 5 | ||
| 7 | 12 | 3 | ||
| 5 | 12 | 3 | ||
| Confidence interval: 4.426-6.694 Mean: 5.56 Range: 1-14 | ||||
| Maternal preventive treatment | 85 | Folic acid intake | 24 | 20 |
| Ultrasound for the early detection of CLP | 3 | Fifth month of pregnancy | 2 | 2 |
| Eighth month of pregnancy | 1 | 1 | ||
| Maternal complications during pregnancy | 34 | Urinary tract infection | 32 | 11 |
| Cervicovaginitis | 18 | 6 | ||
| Threatened miscarriage | 15 | 5 | ||
WP, weeks pregnant.
Source: Clinical files of patients with CLP treated at HENM at the city of Querétaro 2011-2014.
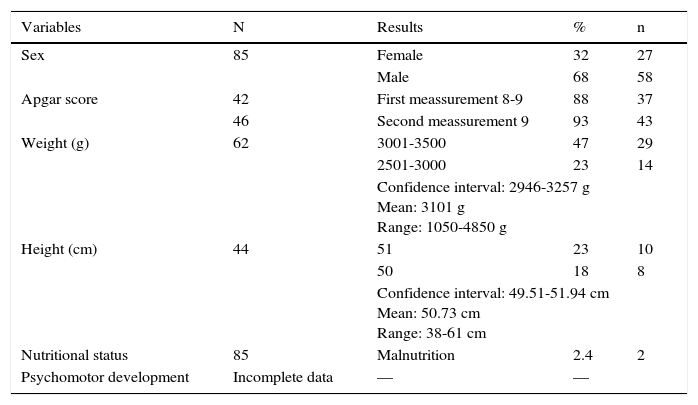
Table 2 shows the variables related to patients with CLP, such as sex and Apgar score, which was between 8 and 9 for 88% of cases (first measure), and five minutes later of 9 for 93% of the cases. Regarding weight, a mean of 3101g was observed, and for height, 50.73cm at birth.
Variables related to the patient with cleft lip and palate.
| Variables | N | Results | % | n |
|---|---|---|---|---|
| Sex | 85 | Female | 32 | 27 |
| Male | 68 | 58 | ||
| Apgar score | 42 | First meassurement 8-9 | 88 | 37 |
| 46 | Second meassurement 9 | 93 | 43 | |
| Weight (g) | 62 | 3001-3500 | 47 | 29 |
| 2501-3000 | 23 | 14 | ||
| Confidence interval: 2946-3257 g Mean: 3101 g Range: 1050-4850 g | ||||
| Height (cm) | 44 | 51 | 23 | 10 |
| 50 | 18 | 8 | ||
| Confidence interval: 49.51-51.94 cm Mean: 50.73 cm Range: 38-61 cm | ||||
| Nutritional status | 85 | Malnutrition | 2.4 | 2 |
| Psychomotor development | Incomplete data | — | — | |
Source: Clinical files of patients with CLP treated at HENM at the city of Querétaro 2011-2014.
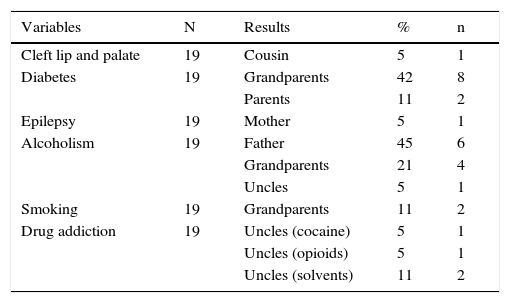
Table 3 includes the risk factors in 19 files; among them, we remark the presence of family history of diabetes in 42% (grandparents) of the cases, CLP in one case (cousin) and epilepsy in another case (mother). Substance abuse reported in the clinical files is also shown. No addictions were found in the mothers in contrast to other relatives. It is worth highlighting the alcoholism in parents (45%), smoking in grandparents (11%) and drug addiction in uncles, with cocaine, opioid substances and solvents (21%).
Risk factors: family history and addictions.
| Variables | N | Results | % | n |
|---|---|---|---|---|
| Cleft lip and palate | 19 | Cousin | 5 | 1 |
| Diabetes | 19 | Grandparents | 42 | 8 |
| Parents | 11 | 2 | ||
| Epilepsy | 19 | Mother | 5 | 1 |
| Alcoholism | 19 | Father | 45 | 6 |
| Grandparents | 21 | 4 | ||
| Uncles | 5 | 1 | ||
| Smoking | 19 | Grandparents | 11 | 2 |
| Drug addiction | 19 | Uncles (cocaine) | 5 | 1 |
| Uncles (opioids) | 5 | 1 | ||
| Uncles (solvents) | 11 | 2 |
Source: Clinical files of patients with CLP treated at HENM at the city of Querétaro 2011-2014.
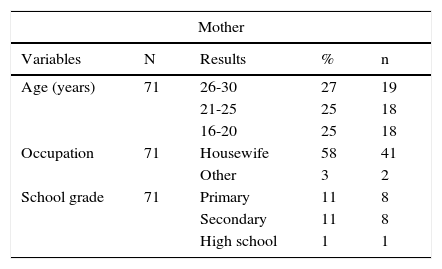
Table 4 shows the results of the socioeconomic study of all patients enrolling at the HENM. It is observed that the majority of mothers are between 26 and 30 years old (27%), predominantly housewives (58%) with primary and secondary grade of studies (11% each group). Most fathers are between 21 and 25 years old (26%), 31% work as construction workers, with a maximum grade of primary education in 13%. The highest percentage of the families of the patients have three to five members (62%), own the house they live in (29%) and produce a monthly income between $ 2,903 to $ 4,354 Mexican pesos (44%).
Socioeconomic study.
| Mother | ||||
|---|---|---|---|---|
| Variables | N | Results | % | n |
| Age (years) | 71 | 26-30 | 27 | 19 |
| 21-25 | 25 | 18 | ||
| 16-20 | 25 | 18 | ||
| Occupation | 71 | Housewife | 58 | 41 |
| Other | 3 | 2 | ||
| School grade | 71 | Primary | 11 | 8 |
| Secondary | 11 | 8 | ||
| High school | 1 | 1 | ||
| Father | ||||
|---|---|---|---|---|
| Variables | N | Results | % | n |
| Age (years) | 39 | 21-25 | 26 | 10 |
| 26-30 | 23 | 9 | ||
| 31-35 | 18 | 7 | ||
| Ocupation | 39 | Construction worker | 31 | 12 |
| Employee | 8 | 3 | ||
| School grade | 39 | Primary | 13 | 5 |
| Secondary | 3 | 1 | ||
| High school | 3 | 1 | ||
| Family | ||||
|---|---|---|---|---|
| Variables | N | Results | % | n |
| Economical dependents | 85 | 3 y 5 | 62 | 53 |
| 1 y 2 | 13 | 11 | ||
| House property | 85 | Owned | 29 | 25 |
| Borrowed | 22 | 19 | ||
| Shared | 15 | 13 | ||
| Monthly income (Mexican pesos) | 85 | $2,903-$4,354 | 44 | 37 |
| $1,451-$2,902 | 25 | 21 | ||
| $4,355-$7,258 | 12 | 10 | ||
Source: Clinical files of patients with CLP treated at HENM at the city of Querétaro 2011-2014.
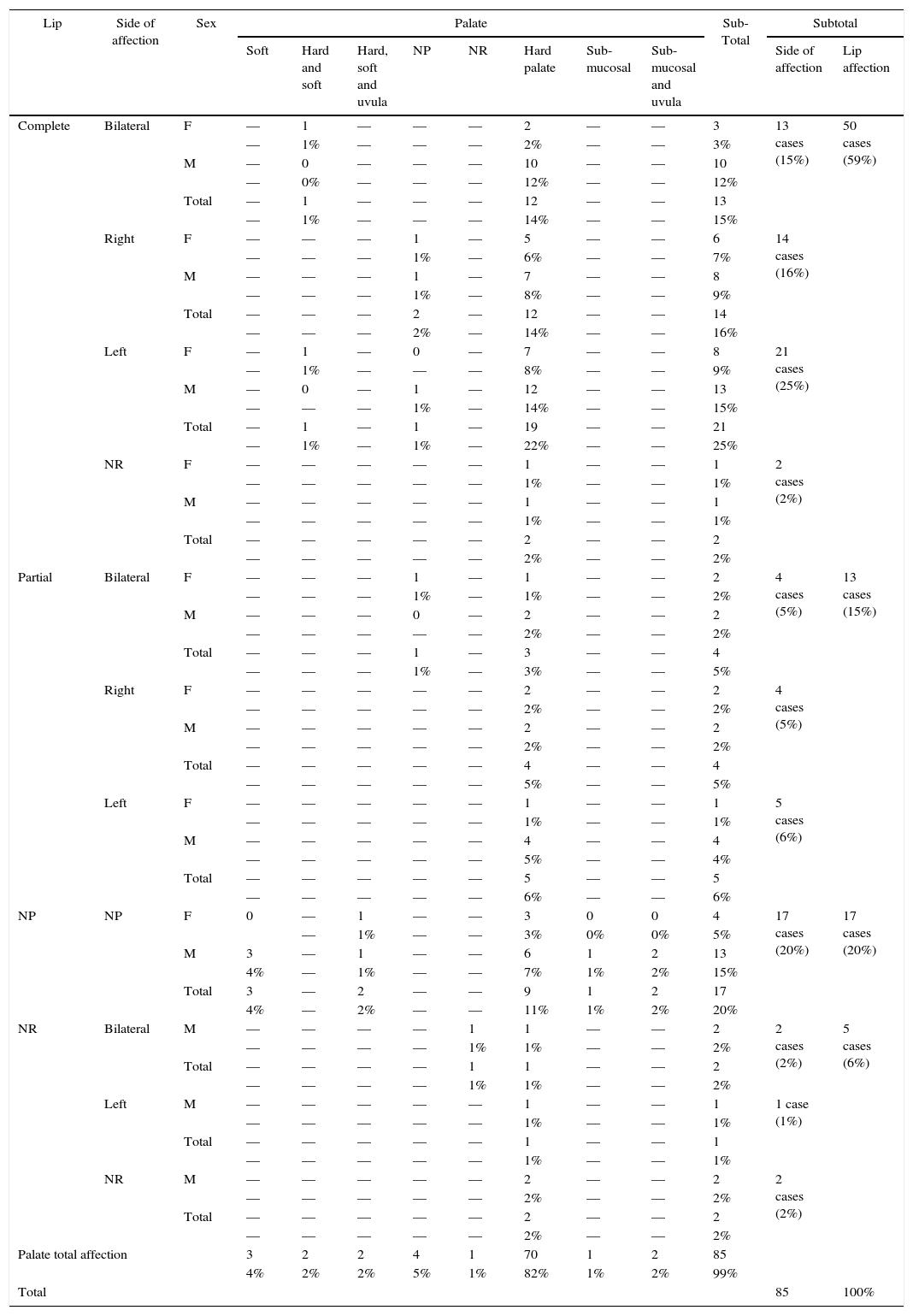
The clinical profile is presented in Table 5. Classification of the disease by sex, structure, and side of affection are shown. The most frequent type of affection was found in males (46% vs 21%), involved the entire lip (59%), the left side being the most affected (25%).
Clinical profile. Classification by sex, affected structure and side.
| Lip | Side of affection | Sex | Palate | Sub-Total | Subtotal | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Soft | Hard and soft | Hard, soft and uvula | NP | NR | Hard palate | Sub-mucosal | Sub-mucosal and uvula | Side of affection | Lip affection | ||||
| Complete | Bilateral | F | — | 1 | — | — | — | 2 | — | — | 3 | 13 cases (15%) | 50 cases (59%) |
| — | 1% | — | — | — | 2% | — | — | 3% | |||||
| M | — | 0 | — | — | — | 10 | — | — | 10 | ||||
| — | 0% | — | — | — | 12% | — | — | 12% | |||||
| Total | — | 1 | — | — | — | 12 | — | — | 13 | ||||
| — | 1% | — | — | — | 14% | — | — | 15% | |||||
| Right | F | — | — | — | 1 | — | 5 | — | — | 6 | 14 cases (16%) | ||
| — | — | — | 1% | — | 6% | — | — | 7% | |||||
| M | — | — | — | 1 | — | 7 | — | — | 8 | ||||
| — | — | — | 1% | — | 8% | — | — | 9% | |||||
| Total | — | — | — | 2 | — | 12 | — | — | 14 | ||||
| — | — | — | 2% | — | 14% | — | — | 16% | |||||
| Left | F | — | 1 | — | 0 | — | 7 | — | — | 8 | 21 cases (25%) | ||
| — | 1% | — | — | — | 8% | — | — | 9% | |||||
| M | — | 0 | — | 1 | — | 12 | — | — | 13 | ||||
| — | — | — | 1% | — | 14% | — | — | 15% | |||||
| Total | — | 1 | — | 1 | — | 19 | — | — | 21 | ||||
| — | 1% | — | 1% | — | 22% | — | — | 25% | |||||
| NR | F | — | — | — | — | — | 1 | — | — | 1 | 2 cases (2%) | ||
| — | — | — | — | — | 1% | — | — | 1% | |||||
| M | — | — | — | — | — | 1 | — | — | 1 | ||||
| — | — | — | — | — | 1% | — | — | 1% | |||||
| Total | — | — | — | — | — | 2 | — | — | 2 | ||||
| — | — | — | — | — | 2% | — | — | 2% | |||||
| Partial | Bilateral | F | — | — | — | 1 | — | 1 | — | — | 2 | 4 cases (5%) | 13 cases (15%) |
| — | — | — | 1% | — | 1% | — | — | 2% | |||||
| M | — | — | — | 0 | — | 2 | — | — | 2 | ||||
| — | — | — | — | — | 2% | — | — | 2% | |||||
| Total | — | — | — | 1 | — | 3 | — | — | 4 | ||||
| — | — | — | 1% | — | 3% | — | — | 5% | |||||
| Right | F | — | — | — | — | — | 2 | — | — | 2 | 4 cases (5%) | ||
| — | — | — | — | — | 2% | — | — | 2% | |||||
| M | — | — | — | — | — | 2 | — | — | 2 | ||||
| — | — | — | — | — | 2% | — | — | 2% | |||||
| Total | — | — | — | — | — | 4 | — | — | 4 | ||||
| — | — | — | — | — | 5% | — | — | 5% | |||||
| Left | F | — | — | — | — | — | 1 | — | — | 1 | 5 cases (6%) | ||
| — | — | — | — | — | 1% | — | — | 1% | |||||
| M | — | — | — | — | — | 4 | — | — | 4 | ||||
| — | — | — | — | — | 5% | — | — | 4% | |||||
| Total | — | — | — | — | — | 5 | — | — | 5 | ||||
| — | — | — | — | — | 6% | — | — | 6% | |||||
| NP | NP | F | 0 | — | 1 | — | — | 3 | 0 | 0 | 4 | 17 cases (20%) | 17 cases (20%) |
| — | 1% | — | — | 3% | 0% | 0% | 5% | ||||||
| M | 3 | — | 1 | — | — | 6 | 1 | 2 | 13 | ||||
| 4% | — | 1% | — | — | 7% | 1% | 2% | 15% | |||||
| Total | 3 | — | 2 | — | — | 9 | 1 | 2 | 17 | ||||
| 4% | — | 2% | — | — | 11% | 1% | 2% | 20% | |||||
| NR | Bilateral | M | — | — | — | — | 1 | 1 | — | — | 2 | 2 cases (2%) | 5 cases (6%) |
| — | — | — | — | 1% | 1% | — | — | 2% | |||||
| Total | — | — | — | — | 1 | 1 | — | — | 2 | ||||
| — | — | — | — | 1% | 1% | — | — | 2% | |||||
| Left | M | — | — | — | — | — | 1 | — | — | 1 | 1 case (1%) | ||
| — | — | — | — | — | 1% | — | — | 1% | |||||
| Total | — | — | — | — | — | 1 | — | — | 1 | ||||
| — | — | — | — | — | 1% | — | — | 1% | |||||
| NR | M | — | — | — | — | — | 2 | — | — | 2 | 2 cases (2%) | ||
| — | — | — | — | — | 2% | — | — | 2% | |||||
| Total | — | — | — | — | — | 2 | — | — | 2 | ||||
| — | — | — | — | — | 2% | — | — | 2% | |||||
| Palate total affection | 3 | 2 | 2 | 4 | 1 | 70 | 1 | 2 | 85 | ||||
| 4% | 2% | 2% | 5% | 1% | 82% | 1% | 2% | 99% | |||||
| Total | 85 | 100% | |||||||||||
F, female; M, male; NP, Not present, NR, not reported.
Source: Clinical files of patients with CLP treated at HENM at the city of Querétaro 2011-2014.
Hard palate injuries were present in 82% of the cases, of which 11% did not involve the lip, and males were more frequently affected (39%).
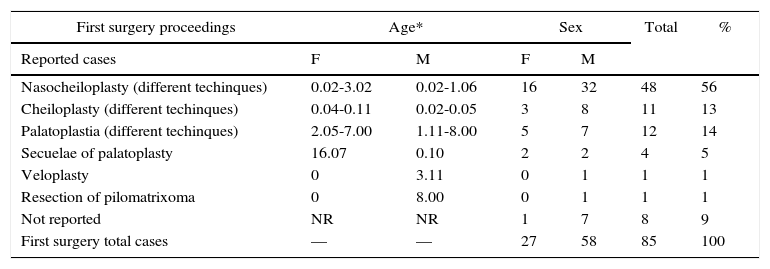
Table 6 shows the classification of surgeries according to the order in which the procedure were performed, the types and the relationship that they keep on age and sex. Results are shown by both procedure and sex.
Practiced surgeries.
| First surgery proceedings | Age* | Sex | Total | % | ||
|---|---|---|---|---|---|---|
| F | M | F | M | |||
| Reported cases | ||||||
| Nasocheiloplasty (different techinques) | 0.02-3.02 | 0.02-1.06 | 16 | 32 | 48 | 56 |
| Cheiloplasty (different techinques) | 0.04-0.11 | 0.02-0.05 | 3 | 8 | 11 | 13 |
| Palatoplastia (different techinques) | 2.05-7.00 | 1.11-8.00 | 5 | 7 | 12 | 14 |
| Secuelae of palatoplasty | 16.07 | 0.10 | 2 | 2 | 4 | 5 |
| Veloplasty | 0 | 3.11 | 0 | 1 | 1 | 1 |
| Resection of pilomatrixoma | 0 | 8.00 | 0 | 1 | 1 | 1 |
| Not reported | NR | NR | 1 | 7 | 8 | 9 |
| First surgery total cases | — | — | 27 | 58 | 85 | 100 |
| Second surgery proceedings | Age* | Sex | Total | % | ||
|---|---|---|---|---|---|---|
| F | M | F | M | |||
| Reported cases | ||||||
| Palatoplasty (different techinques) | 1.01-3.06 | 1.01-4.03 | 9 | 20 | 29 | 58 |
| Cheiloplasty (different techinques) | 1.01-3.00 | 3.00 | 2 | 1 | 3 | 6 |
| Soft palate and uvula reconstruction /faringoplasty | 0 | 2.05-3.11 | 0 | 4 | 4 | 8 |
| Secuelae of palatoplasty (different techinques) | 1.01-8.00 | 1.11-9.00 | 2 | 8 | 10 | 20 |
| Plastic surgery | 0 | NR | 0 | 1 | 1 | 2 |
| Not reported | NR | NR | 0 | 3 | 3 | 6 |
| Second surgery total cases | — | — | 13 | 37 | 50 | 100 |
| Third surgery proceedings | Age* | Sex | Total sex | % | ||
|---|---|---|---|---|---|---|
| F | M | F | M | |||
| Reported cases | ||||||
| Palatoplasty (different techinques) | 2.11 | 2.00-5.06 | 1 | 7 | 8 | 57 |
| Cheiloplasty (different techinques) | 2.00 | 0 | 1 | 0 | 1 | 7 |
| Retrofaringeal flap | 0 | 3.00 | 0 | 1 | 1 | 7 |
| Other | 0 | 16.00-20.06 | 0 | 2 | 2 | 14 |
| Not reported | NR | NR | 1 | 1 | 2 | 14 |
| Third surgery total cases | — | — | 3 | 11 | 14 | 100 |
| Fourth surgery proceedings | Age* | Sex | Total sex | % | ||
|---|---|---|---|---|---|---|
| Reported cases | F | M | F | M | ||
| Retrofaringeal flap | 4.07 | 0 | 0 | 1 | 1 | 50 |
| Palate reconstruction and faringoplasty | 0 | 4.00 | 0 | 1 | 1 | 50 |
| Fourth surgery total cases | — | — | 0 | 2 | 2 | 100 |
F, female; M, male.
The recorded data for the first surgery corresponds to 100% of the sample; the number of cases progressively decreased for the second (58%), third (58%) and fourth (2%) surgeries.
Procedures involving any labial structure were found in a higher percentage in the first surgery (70%), while those involving the palate had the highest percentage in the second and third surgery (58% and 57%, respectively).
4Discussion4.1Epidemiological profileAccording to our review of the literature, isolated CLP occurs in 70% of cases, and the remaining 30% is associated to syndromes.19,20 From the patients who had treatment at HENM during 2011-2014, 15% were syndromic cases and 85% non-syndromic cases.
Worldwide, the highest prevalence occurs in Asian and Native Americans (one case in 500), the Caucasian population has an average prevalence (one case in 1000), and the lowest is in the African population (one case in 2500).2,23
Nationally, a prevalence of 0.59, 0.56 and 0.60 is reported (per 1,000 cases) in 2011, 2012 and 2013, respectively.24,25,28 In 2011, Gonzalez-Osorio et al. reported a prevalence of CLP of one case in 700 people. Meanwhile, during 2013, the HM and the Mexican Social Security Institute reported 17 new cases of CLP in the state of Queretaro.24–28
Dixon et al. reported a prevalence of 70% in cases with CLP and 50% with only palate affection.23 The reported figures correspond to 85% of non-syndromic cases involving one or more structures (70% of these affecting only the hard palate). In this study, it was observed that 59% involved the whole lip, mostly affecting males (46%) on their left side (25%). Interestingly, 82% of the sample only had the hard palate affected, and most of them were males (39%) also (Table 5).
In the studied population, only three cases with complete unilateral lip involvement, one case of the incomplete bilateral lip and nine with hard palate were observed. In 63 cases (74%), the affection of both structures was detected, in 17 cases (20%), there was no form of lip affection, and five cases did not have data about it (6%).
Importantly, perhaps due to the low incidence of CLP reported in Querétaro (14, 16 and 17 cases during 2011, 2012 and 2013, respectively25,28) prevention has not been considered a priority. However, there is an increase in the number of cases. Given the lack of prevention, the number of cases of this disease may rise in the future bringing negative effects. Hence, the importance of the work carried out at the HENM: timely detection, treatment, and follow-up until the resolution of the disease through a multidisciplinary team.
The city with the highest number of patients with CLP in our analysis was Querétaro, which ranked first with 42% (36). This is expected, because according to data by INEGI (by its acronym in Spanish: National Institute of Statistics and Geography), 70% of the inhabitants of this region are concentrated in the urban area (1,382,105 inhabitants), and it is also where there are more hospitals that provide specialized medical care. No information was found pointing that the patients belonged to a particular ethnic group with a genetic disorder (Table 1).
According to the reviewed literature, recognition of the condition in the intrauterine stage is very helpful to minimize complications at birth. The information from the HENM files was not sufficient to know if there was an intrauterine detection of CLP in all women during their pregnancy. However, of the 85 files reviewed, three cases (3.5% of the sample) were early detected by gynecological ultrasound (Table 1). A case was found in which four ultrasound studies were performed during pregnancy, and in the latter, CLP was detected; the other two cases were diagnosed at the eighth month of pregnancy (Table 1).
It should be remembered that the fusion of the processes that will form the primary lip and palate takes place around the seventh week of pregnancy, and is in the twelfth week when the secondary palate forms. Consequently, after thirteenth or fourteenth weeks of pregnancy, an early diagnosis could be obtained, which would allow an early assessment and the establishment of early treatment for CLP. Thus, both parents and health personnel would be prepared to achieve the survival of the newborn (which is compromised due to the nutritional status because problems for weight gain that arise from insufficient sucking of breast milk, the presence of milk in the nasal cavity, aspiration, and the small amount of intake) and schedule early needed surgical treatments.12,19
In the studied population, only two cases of malnutrition (2.4%) were found, without mentioning the degree, but were referred to the nutritionist (Table 2). According to the reviewed literature, one of the problems that parents face is the difficulty in feeding the newborn with CLP,1,2,9–12 which is solved with the first two surgeries as well as with other actions.3,15–17
Predisposing factors that cause orofacial fissures are congenital and environmental. Recent epidemiological studies22,23 have shown that the presence of isolated cleft lip is due to etiological factors including strong genetic associations.29 Some cases of cleft palate with subclinical cleft lip signs have been found because the embryonic origin is different in the involved tissues, and it has even been proposed to study their etiology separately in future studies.
According to the literature, a high recurrence in family transmission of CLP exists, when compared with other congenital disabilities. In studied populations, 32% for cleft lip and 56% for CP in first-degree relatives is observed.2,30
Our review of the clinical files did not show data on genetic inheritance, but two cases of patients with complete left CLP were observed: one having a paternal cousin and history of smoking and alcoholism in the family as predisposing environmental factors, and another reported having unspecified relatives with the disease, and no environmental factors (Table 3).
In Mexico, the HM issued technical guidelines on prevention, treatment, management and rehabilitation of children with CLP,4 providing genetic counseling to patients, parents, and relatives of patients with this condition so they can understand and act according to the situation that they face. In contrast to other reports, a higher proportion of young mothers (younger than 30 years old) with children presenting with the disease was found in this study (Table 4).
In contrast to what was established by the HM1,4 in terms that a greater parental age (>45 years for men) represents increases risk, the results of this research showed a higher proportion of young parents (between 21 and 35 years) (Table 4).
Regarding other points offered by the HM, advising to give genetic counseling, in this study no family history data was found for the previous birth or congenital defects or family history with chromosomal abnormalities.
Also, among genetic advises by the HM,4 there are histories of abortions or fetal loss, data not reflected in the clinical records; however, within the complications observed in our analysis of the information, urinary tract infection, cervicovaginitis and threats of abortion were found. It is important to mention that the highest percentage of the observed cases of CLP corresponded to the first pregnancy (15.3%) and had a gestation age of 40 weeks (38%) (Table 1).
According to literature, among the environmental factors that contribute to the formation of CLP, low socioeconomic level stood out. As mentioned above, the prevalence in some populations is of one in 700 patients, with social, economic and belonging to some ethnic groups as factors associated with the condition1,20,26,27,31 (Table 4).
Associations that are predisposing factors for CLP are alcohol intake, smoking, maternal age, diabetes, previous abortions, genetic and nutritional aspects, pesticides use in agriculture, exposure to ionizing radiation, infectious agents, stress, family history and any other craniofacial malformation.1,2,9–12
When investigating other predisposing environmental factors in the relatives of the patients with CLP in the sample, data on alcoholism, smoking, and drug abuse were found. The most reported addiction in the studied population was alcoholism in fathers, grandparents, and uncles; other reported addictions were smoking in grandparents and drug abuse in uncles (addiction to cocaine, opioids, and solvents) (Table 3).
No data was found specifying the line of inheritance; however, grandparents were the group that reported more illnesses (asthma, cirrhosis, hypotension, language delay).
In the studied sample, one maternal epilepsy was present. In this regard, some authors report CLP association with risk factors such as maternal epilepsy with anticonvulsants intake during the first trimester of pregnancy,1,32,33 and acute illnesses such as influenza. However, for this particular case data on the treatment of the mother for the control of her condition was not known, so that the ingestion of anticonvulsants cannot be associated with the condition of CLP (Table 3).
4.2Clinical profileIn the study conducted in Mexico City between 2003-2008 on CLP and socio-demographic, socioeconomic factors and associated pollution, an average of 1,000 births per year was reported nationwide.1 According to the births in the state of Queretaro during 2013 (41 817), 17 cases of CLP were reported by the HM; this represents an incidence of 0.87 per 100,000 inhabitants. This data could be due to lack of epidemiological surveillance during those years.25,28
In Mexico, the HM4 reports a frequency of 21% of patients with an isolated cleft lip, 33% with only the palate affected, and 46% with both structures involved. According to data obtained from patients with isolated lip involvement at HENM, the cases with an affectation of the palate and those compromising both structures do not match with the nationally reported percentages.
This study reports a higher percentage of isolated palate affection in males (58%) compared with females (27%); that is, a ratio of 2.1: 1. In contrast, females have a higher ratio of 2: 1 in two studies2,23 and 1: 1 in another study;20 the latter matches with what was reported in 2006 by the HM (Table 5).4
Regarding the involvement of the lip with or without affection of the palate, the percentage found was 69% for males and 32% females, with a ratio of 2.1: 1. Studies by Marazita,20 Dixon et al.,23 and Parada and Chai2 mentioned a higher incidence in lip affection in males (2:1) consistent with that reported by the HM in 20064 but not with the present results (Table 5).
Regarding location of the cleft lip, the results of this research are consistent with the revised literature,2,20,23 where the left side is the most frequently affected, with a 2: 1 ratio. The proportion obtained in this study was 1.6: 1 (Table 5).
Patients with CLP need interdisciplinary treatments performed by specialists: plastic surgeons, orthodontists, dentists, otolaryngologists, speech therapists, psychologists, ophthalmologists, pediatricians,6 among others, during the different stages of life for both patients and their relatives, who are socially and psychologically affected.14,22
The CLP clinic at the HENM provides interdisciplinary care to patients. Those in charge of this clinic seek the best care for outpatients to the town of Queretaro: scheduling the following consultations on the same day, facilitating the process of care for the patient and helping the economy of families, taking into account the expenses it would represent the transport to consult with several doctors on different days.
The HENM offers CLP patients the possibility of carrying out a multidisciplinary treatment, accompanies the development and growth of the patient, and tries to make it accessible to the family economy performing a socioeconomic study, so that all patients are covered with the necessary treatment.
The interdisciplinary team includes dentists since dental arches are affected in these patients, depending on whether the cleft is unilateral or bilateral. Generally, they have unilateral or bilateral crossbites and lack of development of premaxilla, causing an occlusion class III,34 absence of dental germs, and deforming shape. Maxillary orthopedic treatments are very useful in getting the arch shape and directing the lingual position, which helps the development of the maxillary arches.
Our data shows the placement of palatal obturators according to the needs of the patients. The absence of several patients to the prophylaxis dental appointments for fluoride application or restorations was observed.
The early prescription of dental treatment allows carrying out a treatment plan for teeth that are in ectopic positions and, therefore, difficult access for cleaning, which compromises their integrity. In some cases, the referral to the orthodontist was reported without further details.
Maxillary orthopedic treatment helps the development, mainly of the maxilla compromised by the fissure, allowing the recovery of the necessary space for dental eruption, and contribute to a better success at the time of surgery. Orthodontics is helpful to achieve a proper occlusion and relieve dental positions.
Another team that provides services to these patients is the Psychology service since a guilt factor appears in parents when they learn that their child has this condition, according to the literature reviewed. As a result, psychological problems arise due to the lack of knowledge about the disease and the different treatments that should be provided during the development of the patient.35 In this sample, the mother was referred to psychological treatment in only one case.
Facing CLP, patients have problems integrating into society since they look different and speak differently from other people in the stages of their development. There are reports of foreign questionnaires that have been used to measure the impact on parent-child relationships (The Alarm Détresse BéBé score) and on parental stress to a congenital condition (Parenting Stress Index).36 At the time of this study, no specific questionnaire for CLP had been found.
At the consultation of Pediatrics, tests are performed to evaluate psychological and motor development of the patient; although each child develops differently, the order in which they start controlling their body begins with the head, hands, and then feet. If necessary, there is a clinic for early stimulation to help the family and the patient.
Observed data on the psychomotor development of patients show that patients with non-syndromic CLP have the same development as any other child without this condition. In the reviewed files, two cases were undernourished and referred to the Department of Nutrition. With proper counseling for parents, there should not be problems to feed the patient correctly.
In its technical guideline for prevention, treatment, and rehabilitation of children with CLP,4 the HM proposes four surgeries to repair this condition. The first one should be performed at three months of age for lip and hard palate closure and the reconstruction of the nasal tip. A second surgery, for palate closure and pharyngoplasty should be performed between 12 and 18 months of age. The third surgery, to perform a bone graft, should be carried out between six and eight years. Finally, a fourth surgery after 14 years of age, to improve facial aesthetics (as rhinoseptumplasty or mentoplasty) (Table 6).
The first surgery is performed in patients with CL when they meet the requirements of having a hemoglobin count of at least 10g, being older than ten weeks, and weighing at least 10 pounds (4600g).3
In most cases, the first surgical procedures were nasocheiloplasty, cheiloplasty, and palatoplasty. This is consistent with that established by international agencies and the HM for the care of patients with CLP, where the first surgery is performed to the seal the lip (Table 6).
There are different opinions on when to perform the first surgery. The Muenster protocol proposes to close the lip between four to six months old. To Anastassov and Joos, the best age is three months old, and Hamburg suggests the procedure at eight months old.37 In this study, only two cases exceeded the age suggested by these authors (a girl of 3 years two months of age with malnutrition, and a one-year-six-month-old child).
During a year, parents and their children have two important contacts with the interdisciplinary team that will provide the assistance to lip (at eight weeks) and hard and soft palate closure (at 24 months). Data obtained from the records of patients treated at the HENM CLP agreed with this information.
Unfortunately, no data to corroborate the advantages offered by the first surgery (lip and palate closure) in patients with CLP was found. However, among these, the following have been reported:
- -
Promote better feeding
- -
Reduce health complications
- -
Allow better adaptation of the involved structures
- -
Aid dentition, to later dental and orthopedic treatment
- -
Improve the appearance of the child
- -
Reduce the psychological impact of parents and society
The resolution of cases by some palatoplasty is performed during the second surgery, which meets the specifications of the HM in the number of surgeries and type of procedures that should be performed in these patients (Table 6).
The parameters established by the HM are fulfilled in the different surgical procedures performed at the HENM; data analysis show the behavior of the resolution of the disease in the decreasing number of surgical procedures and the different surgeries performed according to the patient's needs and development.
According to the analysis of the different surgeries performed at the HENM regarding the involved structures, the use of procedures such as the Miller technique, the Bardach flaps technique, Vómer flap and Veau technique coincided with the recommendations by Huber et al.3
When analyzing the reported data in the clinical files, unintended consequences after surgery in the treated structures were found, which would have to be considered for the following surgical procedure planned.38
The percentage of cases decreased after the second surgery and drastically dropped for the fourth, in which only two cases were reported. Surgical notes did not show if the treatment presented a complete solution or if the patients and their families decided to abandon the treatment at some point (Table 6).
The CLP clinic at HENM provides the opportunity to monitor since patient admission if birth happened at the same hospital or by referral from other health care centers or hospitals; unfortunately, there are contextual factors that limit their healthcare. According to data analysis, it is common for families not to continue with a long-term treatment due to several reasons: the lack of economic resources, low schooling, the lack of understanding correct drug administration, as well as factors associated with a culture that does not value health care. All this hinders the proper implementation of treatments that will benefit CLP patients.
Although the HENM provides the option of taking a comprehensive approach, an additional factor is that not all records contain the information needed to keep track of it in the different areas of healthcare involved.
Some findings showed that in this particular studied context not only mothers over 35 years and fathers over 45 years of age are predisposed to have a child with CLP (as stated in the literature). On the contrary, these results showed a higher frequency in young parents.
Regarding degrees of affection, a higher percentage of lip involvement in males, and a decrease in the proportion of the left unilateral condition were observed, in contrast to what has been reported in the literature.
The highest percentages of procedures correspond to the first and second surgery, where the lip and palate are treated. It seems that it is very important to perform these surgical procedures since many of the clinical records reported the absence of clinical remission, which could be helpful for feeding psychological development, early stimulation, dentistry.
The finding of fewer syndromic cases and differences between the affected structures than those reported in the literature supports the development of local epidemiological studies to acknowledge the needs and characteristics of the Mexican population. The findings of this research offer some advantages to continue the analysis of the problems associated with CLP in Queretaro.
Although maternal disease after the third month of pregnancy does not affect the incidence of the disease, it may alter the development of the child. Further research is necessary to investigate about addictions and inherited diseases in these patients. The data of this study are not enough to make a conclusion but a precedent for future studies.
A very important aspect is patient education to promote awareness of the prevention, management, and rehabilitation of the disease. Adherence to their appointments and following medical indications is an arduous task influenced by the lack of studies, the desire to learn and improve their conditions. Most of the studied population has a low income for daily living, although the reported data on household income could be altered by the same parents, so their revenues would not influence the cost of medical services.
With the development of biomedicine, an area of opportunity to reach the bottom of CLP has been opened. Genetic studies on CLP would allow us to learn more about its origin.
Genetic counseling established by the HM should not be overlooked; extensive promotion among the population is required to allow people to take precautions, and plan their pregnancies.
A wide variety of genes that can affect the development of this condition has been reported in the literature. However, a higher percentage of the population should have access to these studies, in order to prevent the onset of CLP.
Data showed that most patients came from communities lacking medical services. The construction of new health care centers would help to solve some problems. It should not be forgotten that the practice of prevention is and will remain as the cheapest medical treatment given to people.
A large influx of patients younger than one-year-old was observed, perhaps due to the aesthetic appearance of the patients, and the parents need to provide a better quality of life. Since the average waiting time for lip surgery is between 4 to 6 months, performing a perinatal diagnosis would provide promotion, prevention, and institution of a treatment plan for the future.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
FundingThe principal investigator did all the economical expenses in this research.
Conflict of interestThe authors declare no conflict of interest.
We want to thank the Hospital de Especialidades Del Niño y la Mujer Dr. Felipe Núñez Lara. We also want to thank Dr. Enimia Vargas, Head of the Education Department, the Ethics Committee of the hospital, Dr. López, Dr. Menchaca, all the personnel who works in the clinical archive and to all the people who contributed to making this study.
Please cite this article as: Pons-Bonals A, Pons-Bonals L, Hidalgo-Martínez SM, Sosa-Ferreyra CF. Estudio clínico-epidemiológico en niños con labio paladar hendido en un hospital de segundo nivel. Bol Med Hosp Infant Mex. 2017;74:107–121.