


Databases of birth certificates and fetal death certificates were used to carry out this study. These are freely available on the website of the Information Health General Direction.1
Birth certificates have been registered nationwide for all live births since 2007. According to category 25 related to the causes of disease of the live newborn, “Birth defects, Illness or Injury of live births” are recorded. Fetal death certificates were initiated in 1956 and record the three leading causes of death in a newborn including the underlying cause of death. Both documents have national coverage, and all institutions of the National Health System in Mexico participate with a single and standardized methodology.
Previously, prevalence rates of congenital malformations (CM) and Down syndrome were revealed based on estimates using the same information sources.2,3 The present paper reports on the prevalence of multifactorial inheritance congenital malformations (MICM) that occur due to complex interactions between genetic susceptibility and environment.4 This group of MICM has a significant impact on child morbidity and mortality. When this group of children is exposed to treatment, their care can be extended even into adulthood. The prevalence of these characteristics varies greatly in different populations.5
Both databases for the period 2008–2012 were combined. The study group was formed based on live births and fetal deaths of 22–45 weeks of gestation with weights ≥500 g; likewise, the usual residence of the mother was Mexico. For the first two variables, cases with incomplete data and mothers living abroad were excluded.
A general database of 10,585,032 births was constructed and comprised of 98.9% live births and 1.1% fetal deaths. Applying the inclusion criteria, the overall resulting study was 10,334,635 births; 2.4% of cases (250.397 births) were excluded, 99.2% were live births, and 0.8% were fetal deaths.
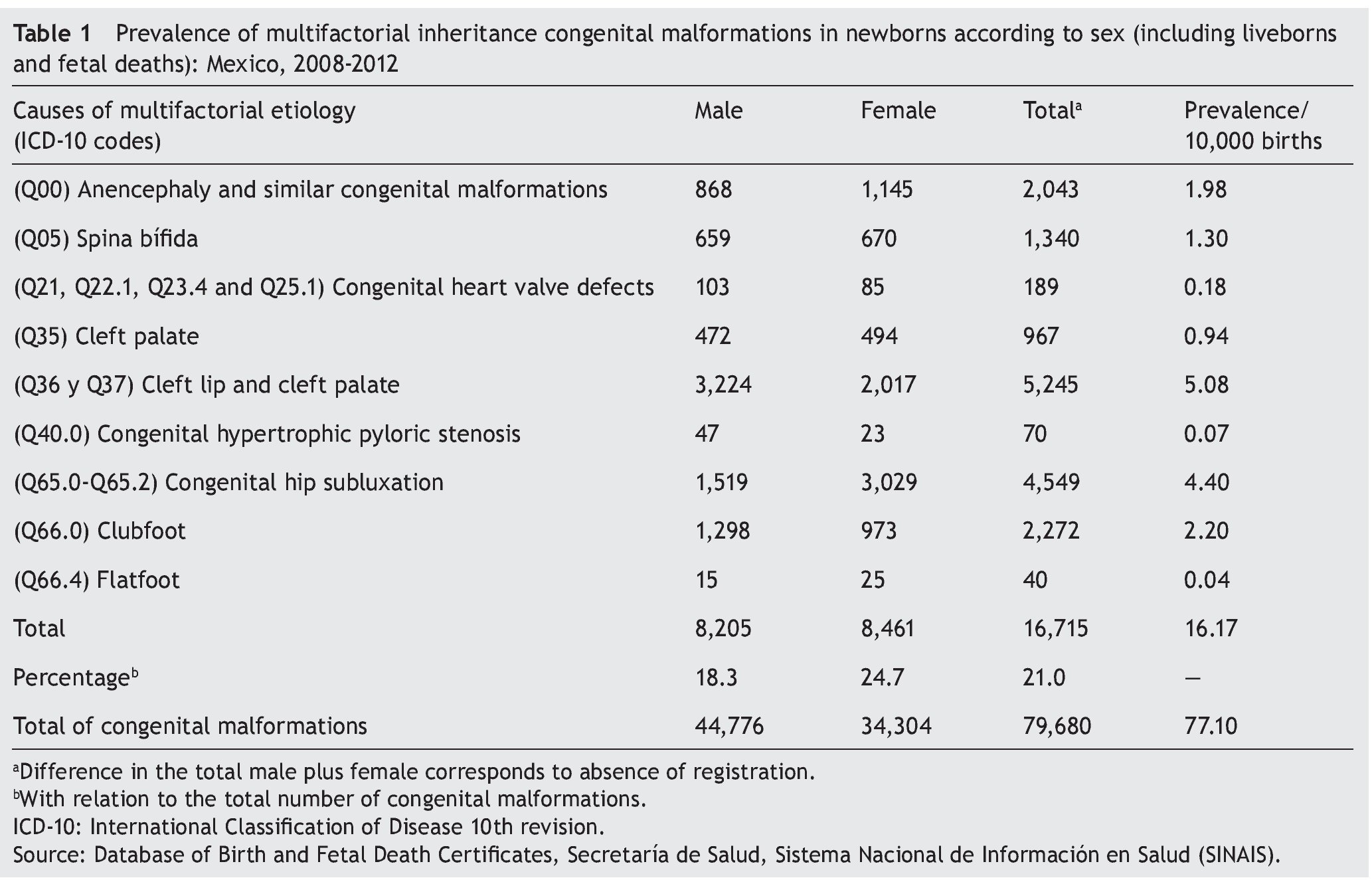
The resulting number of MICM was 79.680 with an overall prevalence of 77.1/10,000 births. Of this total, 91.6% belonged to live births and 8.4% to fetal deaths. MICM distribution by sex was 51.1% for males, 48.8% for females; 0.1% of the data was not registered (Table 1). The MICM ratio was 0.7% for live births and 8.3% for stillbirths.
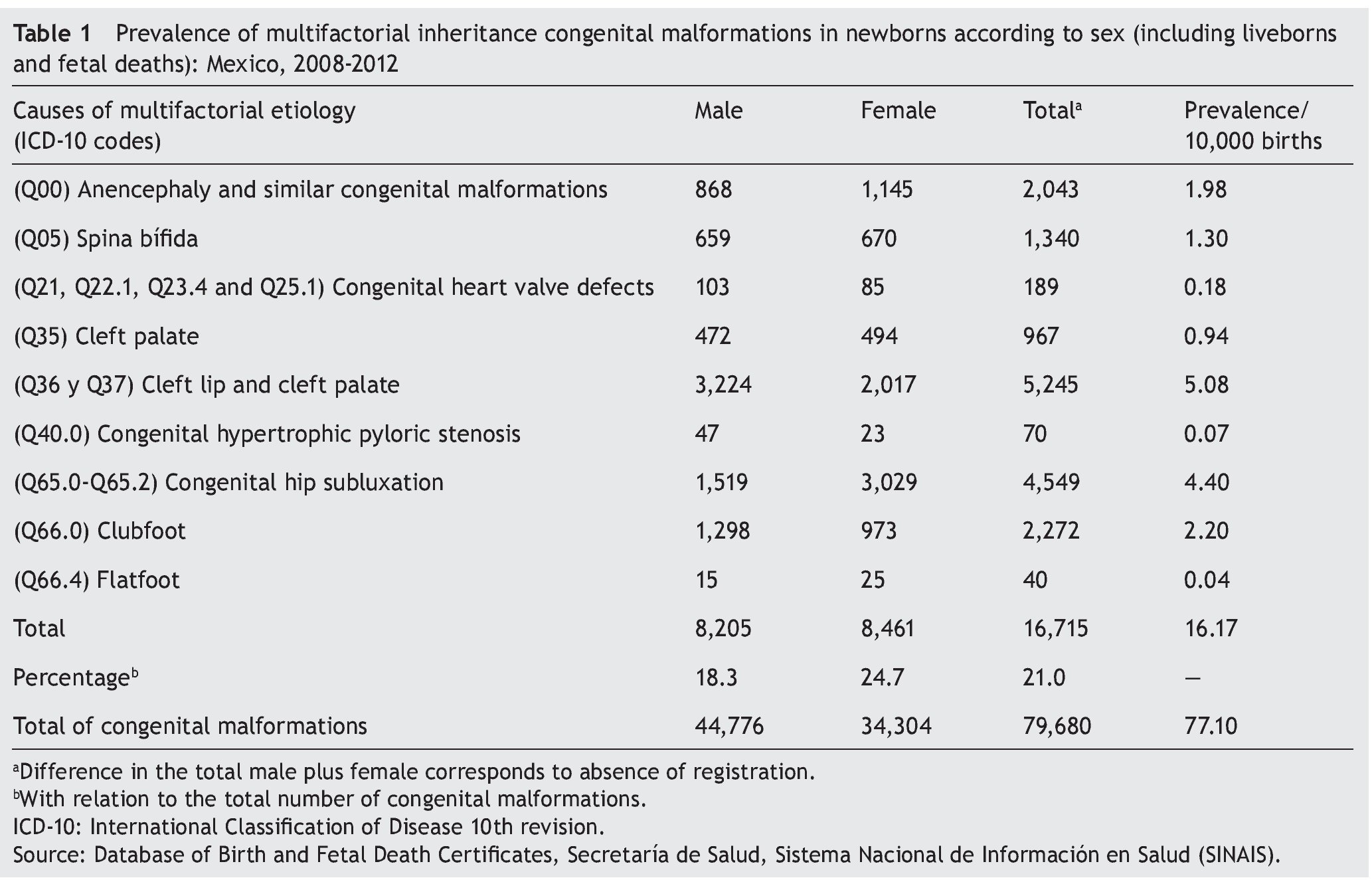
Regarding the causes of the selected multifactorial inheritance (MI), 16,715 cases accounted for 21% of the total congenital malformations recorded during the period under review (Table 1). This corresponded to a prevalence of 1 case/618 births, which shows the importance of this group of malformations.
Distribution of the absolute frequency of MI cases by sex was 18.3% for males and 24.7% for females, considering the respective CM totals (Table 1). Four specific causes stand out. In descending order of prevalence per 10,000 births are the following: cleft lip and cleft palate with cleft lip (5.08); congenital hip subluxation (4.4); clubfoot (2.2); anencephaly and similar congenital malformations (1.98) (Table 1).
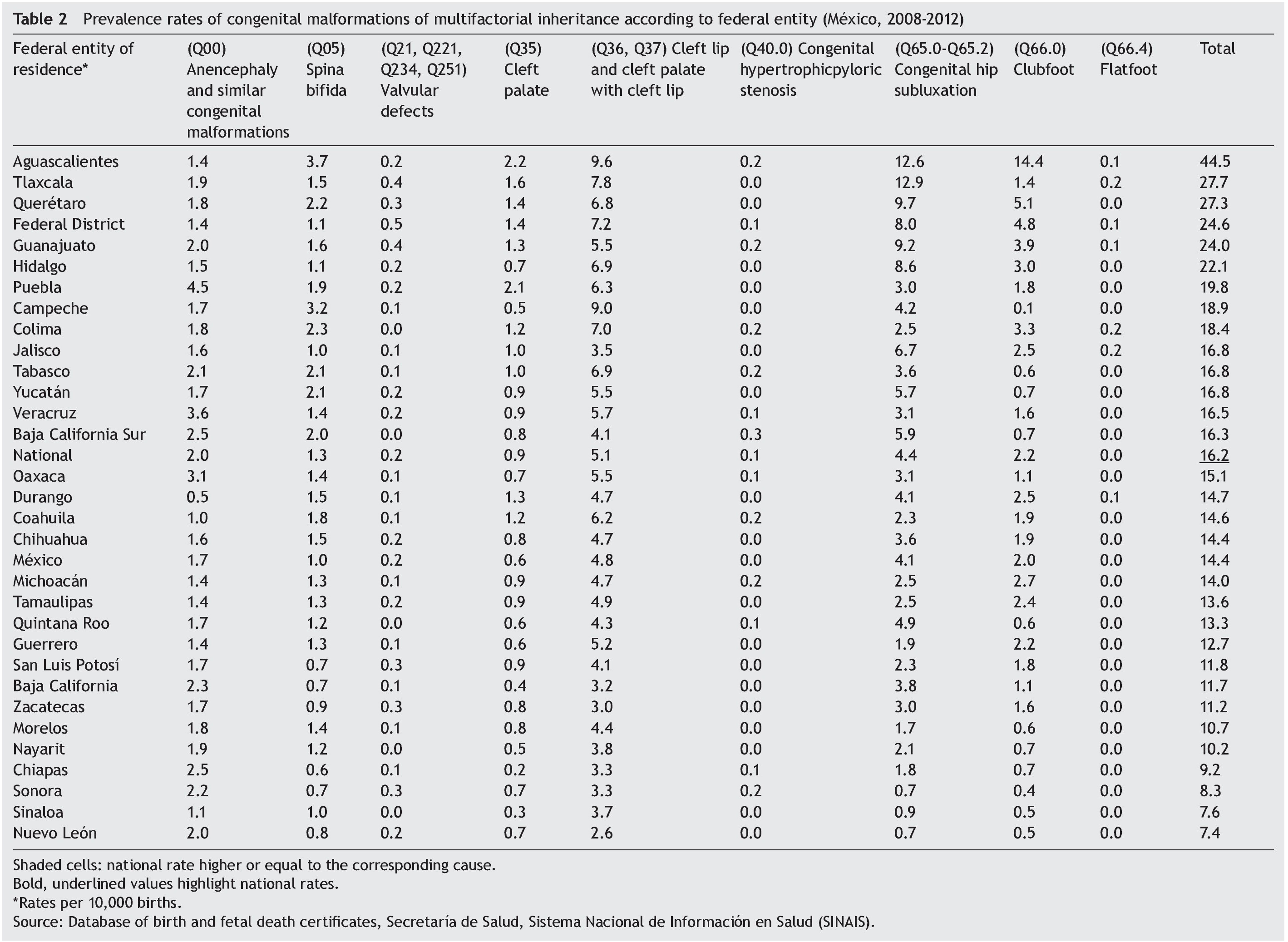
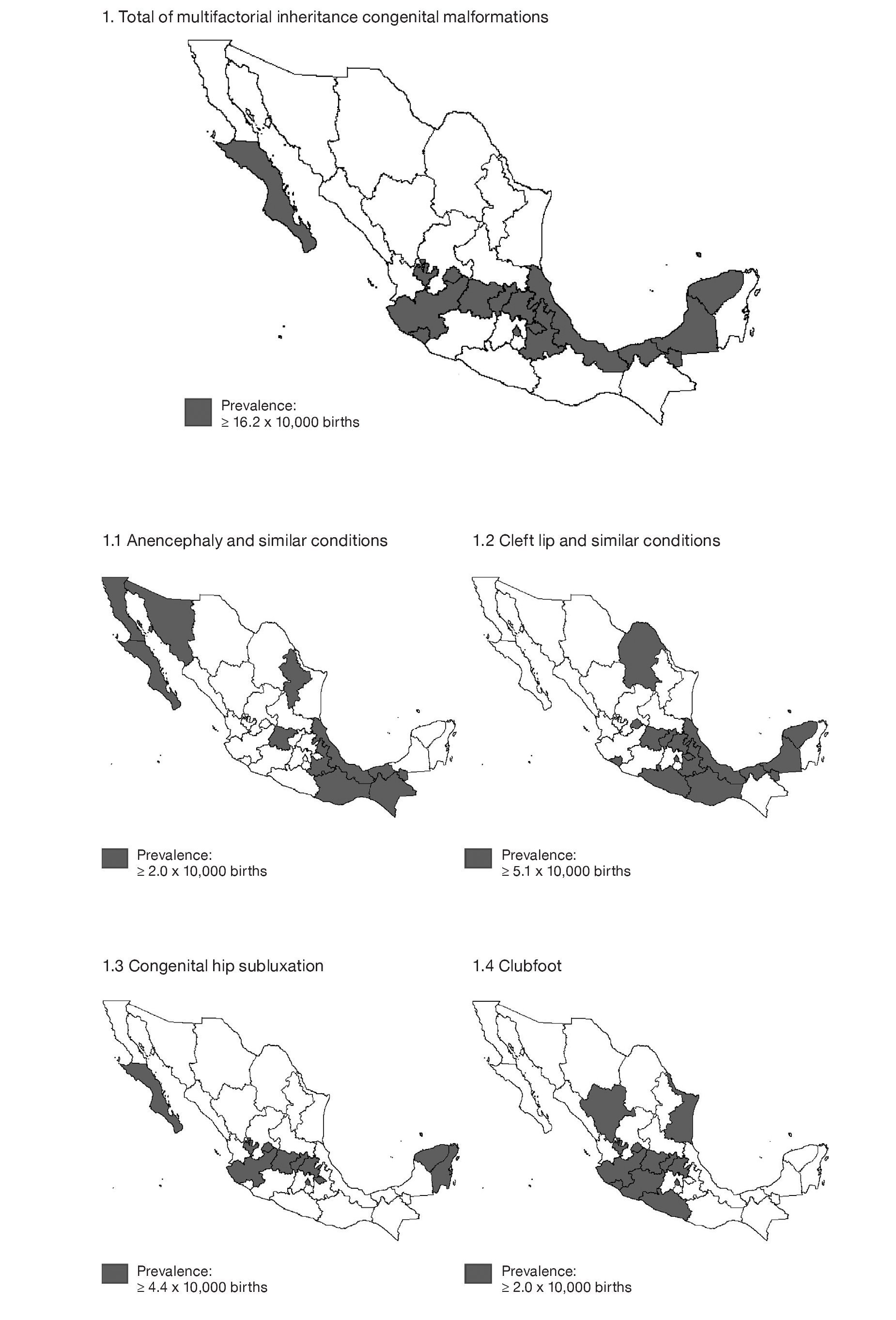
Overall prevalence rates of the MI causes selected by state allow identifying the states that are above the national average (Table 2), which more regularly tend to be located in central Mexico (Aguascalientes, Querétaro, Tlaxcala, Guanajuato, Mexico City, Hidalgo, Puebla, Colima and Jalisco) and in the southeast area bordering the Gulf of Mexico (Campeche, Yucatán and Tabasco) (Figure 1).
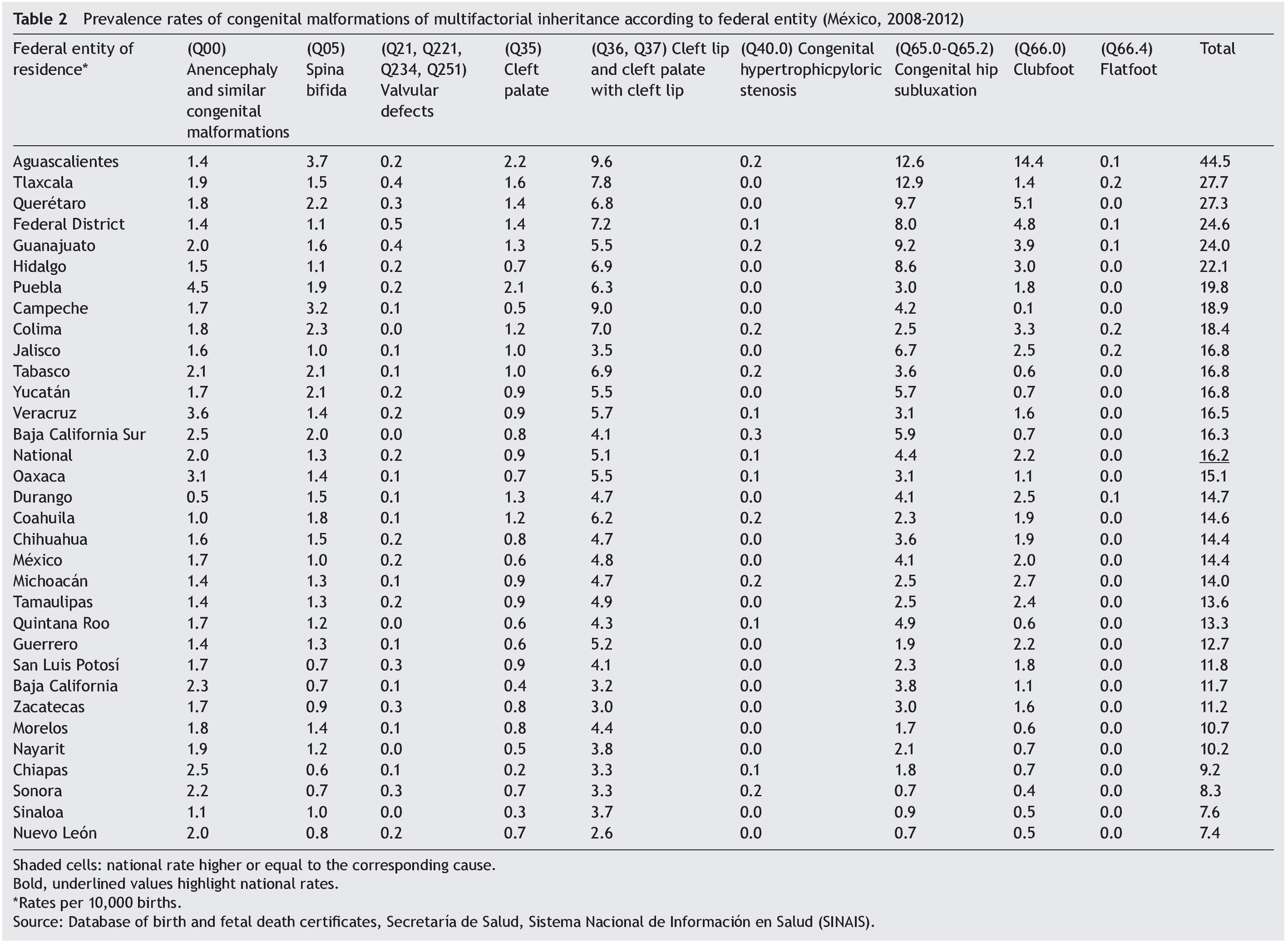
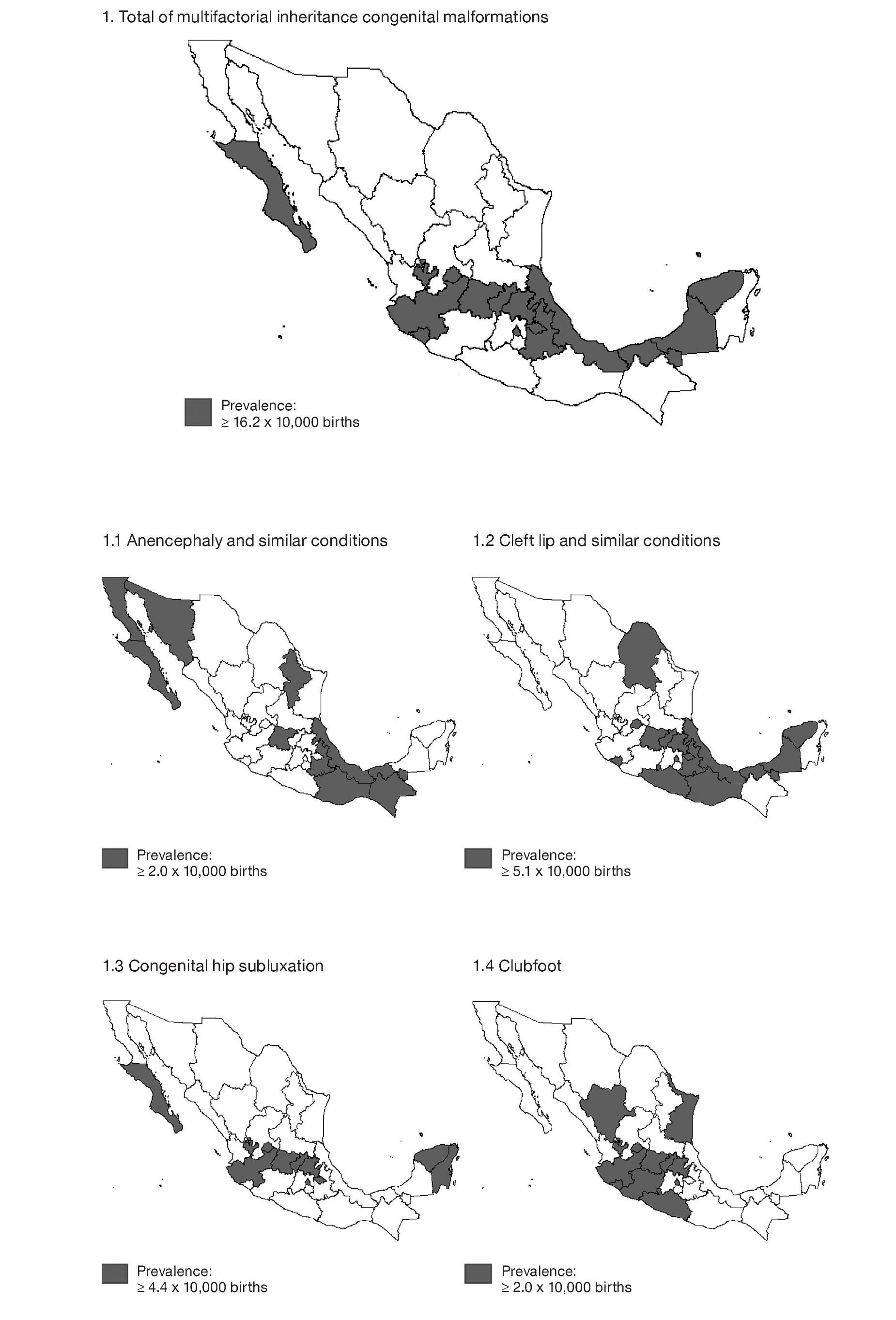
Figure 1. Prevalence rates of causes of multifactorial inheritance congenital malformations according to federal entity (México, 2008-2012).
The strength of this study is that the sources of information are official and issued by the Ministry of Health and this is a nationwide population-based study.
Information obtained through the registration system of birth and fetal death certificates is of great importance to determine the prevalence of MICM, not only nationally but also by state, city and municipality and can be used as part of a continued epidemiological surveil-lance system.
Ethical considerations
The study did not represent a risk to humans because official databases were used and are available to the interested public.
Funding
None.
Conflict of interest
The authors declare that there are no conflicts of interest.
Received 25 February 2015;
accepted 30 June 2015
* Corresponding author.
E-mail:scanuns@hotmail.com (S. Canún Serrano).