




Since it was first described in 1992 by Gagner,1 minimally invasive laparoscopic or retroperitoneoscopic surgery of the adrenal gland has proven to be safe and effective for all types of indications. There is still controversy regarding which surgical approach should be used, as retroperitoneal, transperitoneal (with or without “handports”) and even transdiaphragmatic thoracoscopic approaches have all been reported.2–8 Although the retroperitoneal approach has some advantages, especially in patients with previous abdominal surgery, it is an unusual surgical field with which abdominal surgeons are not familiar. Meanwhile, the transperitoneal approach has been described with 2 different patient positions: lateral decubitus (LD) and supine decubitus (SD).9–12 The LD position provides better vision for this intervention and is currently being used by most endocrine surgery groups. It does, however, have its disadvantages, such as in patients with a history of previous abdominal surgery. It also takes longer to position the patient; moreover, when access to both glands in the same intervention is required, the patient has to be repositioned.
We report the case of a patient who underwent laparoscopic bilateral adrenalectomy, which was performed in a supine decubitus position with 4 trocars. The patient is a 26-year-old woman from Romania with a history of migraines and polyarthritis, which had been diagnosed and treated in Romania when she was a child. She was not under any treatment or follow-up at present. She had undergone an appendectomy and caesarean section.
During gestation, she had been diagnosed with hypertension, which persisted in the postoperative period with the onset of proteinuria. Abdominal ultrasound showed a single left retroperitoneal lesion. CT revealed 2 masses, one in each adrenal gland, the left measuring 3.5cm×2.7cm and the right 2.7cm×2.1cm. A 24h hour urine work-up isolated highly elevated levels of noradrenaline, fractionated normetanephrine and total metanephrine, confirming the diagnosis of bilateral pheochromocytoma. During the study prior to surgery, the patient also presented amaurosis of the left eye associated with an image compatible with retinal capillary hemangioma, which made us suspect a diagnosis of Von Hippel Lindau syndrome.
In our group, the SD approach is always used, both for unilateral adrenalectomy as well as for bilateral cases. Thus, our patient was placed in the SD position, with lateral support at the axilla and the hip on the contralateral side of the gland to be operated on. This achieves sufficient surgical exposure with the range of movement of the operating table, without the need for subcostal support.
The advantage of our SD approach compared with complete LD is its greater simplicity when positioning the patient, which saves surgical time. What is most important is that there are no disadvantages as it provides an excellent surgical field.
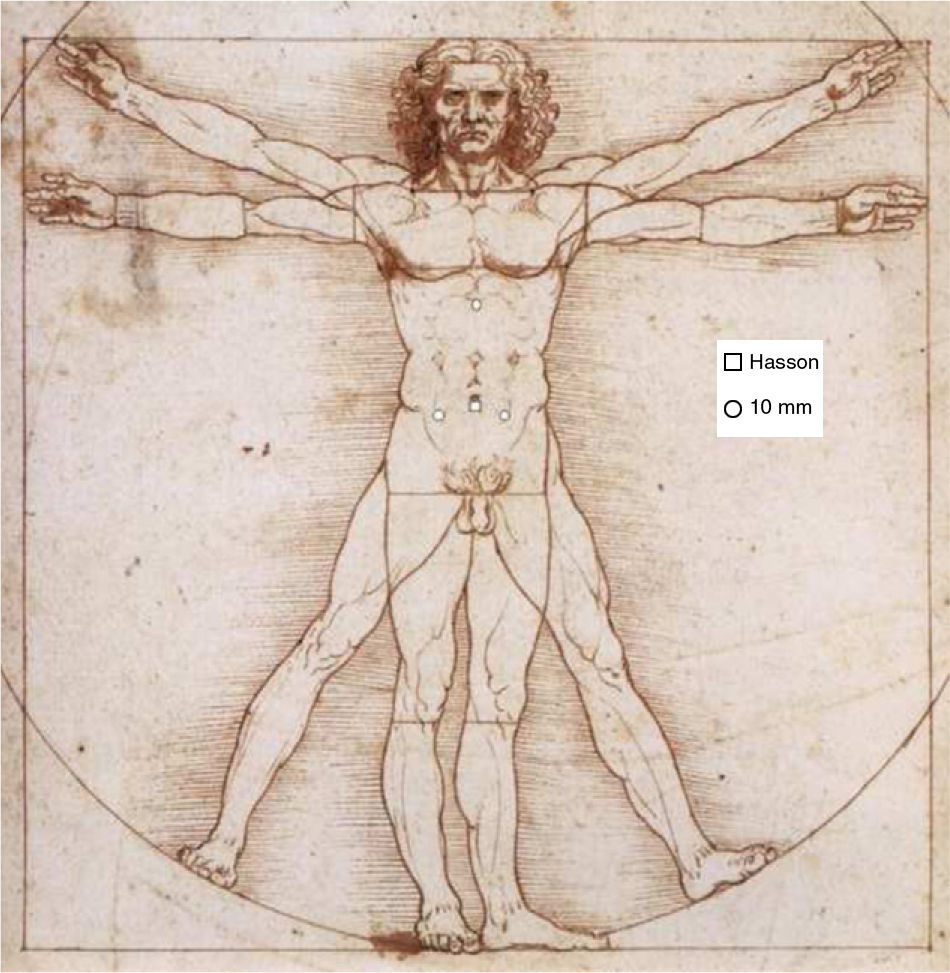
Four trocars were used: a Hasson trocar in the navel for the camera, another 10mm epigastric trocar for hepatic and gastric retraction, and one 10-mm trocar in each iliac fossa for the main surgeon (Fig. 1). The operating table was placed in forced SD towards the side opposite the gland to be treated. The surgeon stood between the patient's legs and the assistant surgeon stood on the side of the decubitus at all times.

Initially, we addressed the right gland, given the increased risk of vascular injury. Achieving a good surgical field is essential, and to do so we used a liver retractor. Afterwards, we cut the right triangular ligament of the liver in order to expose the retroperitoneum. We continued the dissection at this level, progressing through the lateral-inferior margin of the gland, clamping and dissecting the adrenal branches of the right inferior phrenic vein. At this point, we looked for the right adrenal vein, which we cut between clips. The surgical specimen was bagged and left over the liver until the end of the procedure.
We began the dissection of the left gland by releasing the splenorenal ligament and the splenic angle of the colon. We mobilized the spleen medially with the aid of the liver retractor. We then identified the left adrenal vein, which runs from the medial side of the gland obliquely towards the midline and caudal to drain into the left renal vein. The dissection was made as close as possible to the renal vein. We continued to dissect on the superomedial side, ligating the adrenal branches of the left inferior phrenic vein.
We extracted both surgical specimens in separate bags through the Hasson trocar port. The total surgical time was 135min, which was substantially shorter than reports of other papers (320,1 245,2 194,5 240,9 200,11 23512 and 412min, respectively). Total blood loss was less than 100ml. The patient recovered without problems and was discharged on the 5th day post-op.1–3,5,9–14
Bilateral laparoscopic adrenalectomy in the supine position is an alternative that should be integrated in endocrine surgery groups as it significantly reduces surgical time as well as the number of trocars used.
Conflict of InterestThe authors have no conflict of interests to declare.
Please cite this article as: Serralta de Colsa D, Argüello de Andrés MJ, Tallón Iglesias B, Ruiz de la Hermosa A, Seoane González JB. Adrenalectomía bilateral laparoscópica por feocromocitoma en el síndrome de Von Hippel Lindau: técnica con 4 trocares. Cir Esp. 2014;92:137–139.
