




The aim of the study was to assess the influence of a physical exercise programme on VO2max in sedentary subjects with cardiovascular risk factors.
Materials and methodsThe sample was composed of 214 patients (80 males, 134 females) with an average age of 52 years, who were referred to a physical exercise programme from 2 primary care centres of Spanish southeast. It was implemented a 10 week programme (3 training×1h/week) combining strength with cardiorespiratory fitness. TheVO2max was analysed through the Rockport Walk Test (RWT) comparing the pre and post programme measurements.
ResultsThe results show significant improvements on VO2max for both genders (p<0.05). The most pronounced increase in VO2max was among males in the highest age band (56–73 years).
ConclusionsPrescribing and referral exercise programmes from primary care centres must be considered as a resource for improving cardiorespiratory fitness in the population studied.
El objetivo de la presente investigación fue valorar la influencia de un programa de ejercicio físico terapéutico en el VO2máx en sujetos sedentarios que presentan factores de riesgo cardiovascular.
Materiales y métodosLa muestra estuvo formada por 214 pacientes (80 varones y 134 mujeres) con una media de edad de 52 años, derivados de 2 centros de atención primaria del sureste español. Se llevó a cabo un programa de 10 semanas (3 sesiones×1h/sem) que combinaba fuerza muscular con resistencia cardiorrespiratoria. El nivel de VO2máx se analizó mediante el test de campo Rockport Walk Test (RWT), comparando las 2 mediciones efectuadas al inicio y final del programa.
ResultadosLos resultados indican que se producen mejoras significativas sobre el VO2máx en ambos sexos (p<0,05). El aumento más pronunciado en el VO2máx se produce en varones en la franja de edad analizada superior (56-73 años).
ConclusionesLa prescripción y derivación a programas de ejercicio físico desde los centros de atención primaria se debe de valorar como recurso para la mejora del fitness cardiorrespiratorio en la población estudiada.
Cardiovascular risk diseases are the world's leading cause of death, accounting for around 31% of all deaths. These diseases can, however, be prevented by acting on risk factors of a behavioural nature, such as smoking, alcohol consumption, diet and physical activity.1
A number of different studies found that physical activity and cardiovascular fitness, assessed quantitatively through maximum oxygen consumption (VO2max),2 were associated with improvements in health, quality of life and cardiovascular risk factors.3–5
In a study conducted with adults, it was observed that physical activity and cardiovascular fitness were independently associated, with a lower risk of developing cardiovascular disease.6 Other research suggests that cardiovascular fitness induces improvements greater than those of physical activity in different cardiovascular risk parameters.7,8
For the improvement of cardiovascular fitness (VO2max), an increase in the level of physical activity9 has generally been recommended, and continuous physical exercise for cardiorespiratory endurance has been shown to be an effective resource for increasing VO2max in some studies.10 However, a recent study indicates that in adults who are overweight and obese, the modalities of high-intensity interval training (HIIT) lead to better improvements in VO2max than those of continuous endurance training at moderate intensity.11 HIIT has also shown superior benefits in patients with coronary artery disease12 and heart failure,13 in subjects who have just recovered from a myocardial infarction14 and when simply prescribed to improve vascular function.15
However, physical exercise for muscle strength has also been related to slight improvements in VO2max,16,17 although recent studies indicate that muscle strength exercise has a greater influence on cardiovascular fitness when performed in combination with cardiovascular endurance exercise.18–20
In a study with healthy adults, improvements in VO2max were evaluated after two training protocols; one where HIIT was combined with strength training and the other with strength training only. The results showed improvements in the concurrent training group (strength and HIIT), while no significant improvements were found in the strength-only group.21
In addition to the mentioned benefits, power or muscle strength training has also been used in physical exercise protocols with adults and older people to improve functional capacity22 and achieve neuromuscular adaptations.23
There are very few studies available in the international literature on physical exercise intervention programmes in adults or older people. In general, regardless of the type of training used (endurance, strength or concurrent) all the studies we were able to find showed benefits in terms of the cardiovascular fitness of subjects who had diligently followed the programmes.24–29
In a study with older adults with obesity, it was observed that the monitored physical exercise programmes in sports centres led to better improvements over VO2max than those centred around the recommendation of the general practitioner or the prescription of exercise to be performed autonomously at home.30 Significant improvements were also observed with American adults in VO2max as well as in various cardiovascular risk factors after a 6-month programme of directed physical exercise.31
Although the use of physical exercise as a therapeutic strategy for certain diseases is becoming more widespread, there is a lack of studies that include prescribing physical exercise from the primary healthcare perspective with the aim of helping to improve cardiovascular risk factors.32,33
For that reason, this study focused on the prescribing of physical exercise for therapeutic purposes from health centres and aimed to evaluate the influence of a physical exercise programme on the VO2max of sedentary subjects with at least one cardiovascular risk factor. These objectives were pursued within the framework of a larger study of the results of the application of a physical exercise programme on improvement in cardiovascular risk factors and cardiorespiratory fitness in adults: ACTIVA programme.
MethodsParticipantsAn experimental, descriptive, cross-sectional study was carried out with 214 subjects (80 males and 134 females) aged from 26 to 73 (mean±standard deviation: 52.02±8.50). The participants voluntarily agreed to participate in the study, signing an informed written consent form. The sample for this study was extracted from the Therapeutic Exercise Programme that was part of the Murcia Region's 2010–15 Health Plan.
To select the participants, a purposive sampling method was used, as the subjects had to meet the following criteria for inclusion in the programme: have a sedentary lifestyle; have more than one cardiovascular risk factor (hypertension, dyslipidaemia, type 2 diabetes, obesity or smoking); and be a patient of the primary healthcare centres of the town of Molina de Segura (Murcia).
The therapeutic exercise programme groups were formed by patients prescribed therapeutic physical exercise by the general practitioner, who selected the subjects according to the aforementioned inclusion criteria. To be included in this study, they had to have participated in 75% of the programme (a minimum of 22 sessions).
The entire project was carried out in accordance with the ethical standards recognised by the Declaration of Helsinki (revision of 2008) and following the EEC recommendations for Good Clinical Practice (document 111/3976/88 of July 1990).
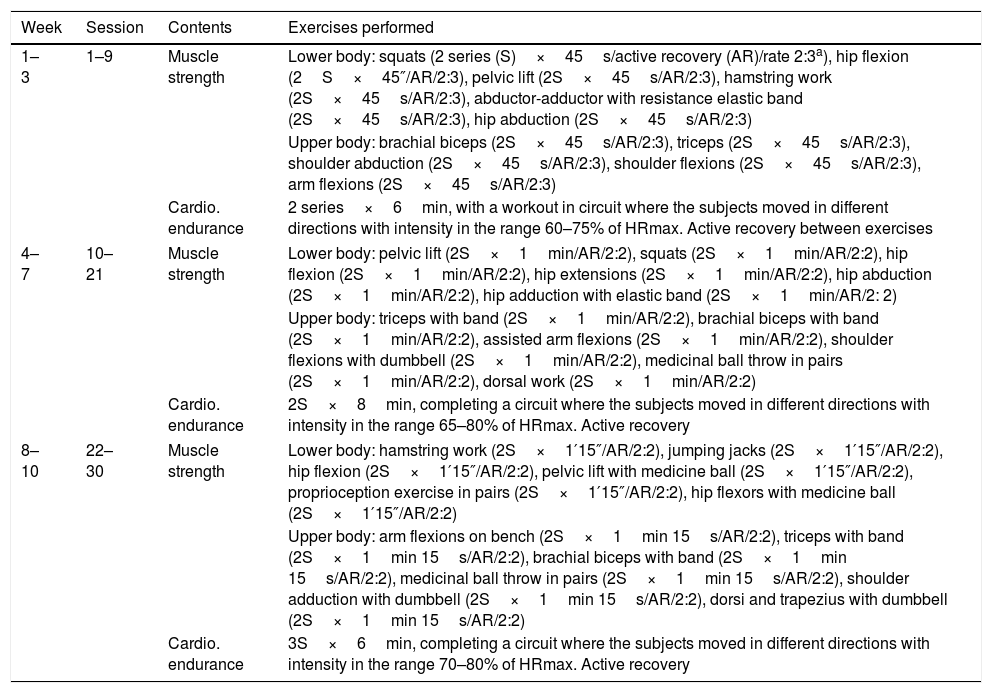
Design of the programmeThe physical exercise programme was designed by physical activity professionals in collaboration with family doctors. It consisted of 30 sessions spread over ten weeks, with three 1h sessions each week. Before starting the programme and after the end of the last session, the appropriate measurements were made.
The sessions were directed by licensed physical activity and sports professionals who had been previously trained to carry out the programme. They began with a warm up of approximately 15min before starting the main part of the session. The sessions alternated between the main content being muscle strength and the main content being cardiovascular endurance, with the intensity and complexity of the exercises gradually increasing as the weeks progressed. The exercises were designed specifically to adapt to the particular characteristics of the sample, while respecting the abilities they wished to develop. The sessions were set out in the form of a circuit, to maximise the motor commitment time and so that subjects could adapt to the requirements of the exercises individually. Additionally, as the aim was to provide individualised attention to the participants, the maximum number of people per group was limited to 15.
In the muscle conditioning sessions, posture, the series, the number of seconds in the series and recovery between each series were all monitored. In the cardiovascular endurance sessions, subjects wore a heart rate monitor to monitor the intensity at which they were exercising, with the upper and lower thresholds marked according to their personal characteristics (Table 1).
ACTIVA-physical exercise programme.
| Week | Session | Contents | Exercises performed |
|---|---|---|---|
| 1–3 | 1–9 | Muscle strength | Lower body: squats (2 series (S)×45s/active recovery (AR)/rate 2:3a), hip flexion (2S×45″/AR/2:3), pelvic lift (2S×45s/AR/2:3), hamstring work (2S×45s/AR/2:3), abductor-adductor with resistance elastic band (2S×45s/AR/2:3), hip abduction (2S×45s/AR/2:3) |
| Upper body: brachial biceps (2S×45s/AR/2:3), triceps (2S×45s/AR/2:3), shoulder abduction (2S×45s/AR/2:3), shoulder flexions (2S×45s/AR/2:3), arm flexions (2S×45s/AR/2:3) | |||
| Cardio. endurance | 2 series×6min, with a workout in circuit where the subjects moved in different directions with intensity in the range 60–75% of HRmax. Active recovery between exercises | ||
| 4–7 | 10–21 | Muscle strength | Lower body: pelvic lift (2S×1min/AR/2:2), squats (2S×1min/AR/2:2), hip flexion (2S×1min/AR/2:2), hip extensions (2S×1min/AR/2:2), hip abduction (2S×1min/AR/2:2), hip adduction with elastic band (2S×1min/AR/2: 2) |
| Upper body: triceps with band (2S×1min/AR/2:2), brachial biceps with band (2S×1min/AR/2:2), assisted arm flexions (2S×1min/AR/2:2), shoulder flexions with dumbbell (2S×1min/AR/2:2), medicinal ball throw in pairs (2S×1min/AR/2:2), dorsal work (2S×1min/AR/2:2) | |||
| Cardio. endurance | 2S×8min, completing a circuit where the subjects moved in different directions with intensity in the range 65–80% of HRmax. Active recovery | ||
| 8–10 | 22–30 | Muscle strength | Lower body: hamstring work (2S×1′15″/AR/2:2), jumping jacks (2S×1′15″/AR/2:2), hip flexion (2S×1′15″/AR/2:2), pelvic lift with medicine ball (2S×1′15″/AR/2:2), proprioception exercise in pairs (2S×1′15″/AR/2:2), hip flexors with medicine ball (2S×1′15″/AR/2:2) |
| Upper body: arm flexions on bench (2S×1min 15s/AR/2:2), triceps with band (2S×1min 15s/AR/2:2), brachial biceps with band (2S×1min 15s/AR/2:2), medicinal ball throw in pairs (2S×1min 15s/AR/2:2), shoulder adduction with dumbbell (2S×1min 15s/AR/2:2), dorsi and trapezius with dumbbell (2S×1min 15s/AR/2:2) | |||
| Cardio. endurance | 3S×6min, completing a circuit where the subjects moved in different directions with intensity in the range 70–80% of HRmax. Active recovery | ||
For the measurement of VO2max, the Rockport Walk Test (RWT),34 also known as the 1-mile (1609m) test, was used. The RWT is a test adaptable to all types of population, as it simply involves walking, and is particularly helpful for use in large samples in ordinary sports facilities. The RWT is an indirect measurement test that uses an equation to obtain an estimate of a subject's VO2max expressed in mlkg−1min−1. To estimate the VO2max, different parameters are required: body weight (kg), age (years), gender, time spent on the route (min) and heart rate (bpm at the end). The following formula is used:

SECA 861 electronic scales (range 0.05–130kg, accuracy of 0.05kg) were used to measure body weight, with the subjects being informed that they should wear light clothes and take off their shoes. A telemetric heart rate monitor (Polar S610) was used to record HR, placed from the beginning of the test until the end. To record the time, the investigator used a digital stopwatch.
Prior to the implementation of the study, a confirmatory analysis of the test was carried out, showing an intra-class R coefficient with high intra-investigator reliability (0.82) and inter-investigator reliability (0.79).
The therapeutic physical exercise programme and the RWT (initial and final) were carried out in an air-conditioned sports hall with a flat horizontal track, where a complete lap, starting at one corner and returning to the starting point, was equivalent to 120m.
The programme had a total duration of three months, and at the beginning and the end of the programme VO2max was estimated through the RWT. Both measurements were carried out on the same day of the week and at the same time (from 6.00p.m. to 8.00p.m.). The investigators, who had a training and familiarisation process with the test, explained to the participants prior to the RWT that they had to complete the course walking and at a speed, “as fast as they could, but keeping a constant rate”. The subjects had to complete 13 and a half laps, with the start and finish point marked out. When they reached the finish point, the investigator recorded the time. All the participants wore a heart rate monitor and immediately after finishing the test, another investigator was responsible for recording the HR reading.
Statistical analysisFrequency tables were created with basic descriptive statistics, calculating the mean, the dispersion and the distribution of the data. Similarly, a t test was carried out to observe the differences between the initial and the final tests. The statistical analyses were carried out with the statistical programme SPSS (v.19.0 of SPSS Inc., Chicago, IL, USA), setting the level of significance in p<0.05. Basic descriptions are presented: mean, standard deviation and standard error of the mean. The distribution of the variables was normal through a Kolmogorov–Smirnov test, so differences in the study parameters at the beginning and end of the exercise programme were established by means of a t test for related samples.
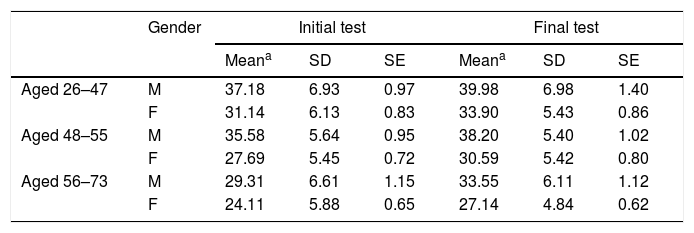
ResultsIn Table 2, comparing the results of the initial and final tests, we see that the means are increased in all age ranges for both genders. The biggest difference was found in males in the 56–73 age range (initial test: 27.45±6.62 vs final test: 32.54±4.88). Similarly, males had higher means than females in both the initial and the final tests in all age groups.
Mean scores obtained in the initial and final VO2max tests by gender and age range.
| Gender | Initial test | Final test | |||||
|---|---|---|---|---|---|---|---|
| Meana | SD | SE | Meana | SD | SE | ||
| Aged 26–47 | M | 37.18 | 6.93 | 0.97 | 39.98 | 6.98 | 1.40 |
| F | 31.14 | 6.13 | 0.83 | 33.90 | 5.43 | 0.86 | |
| Aged 48–55 | M | 35.58 | 5.64 | 0.95 | 38.20 | 5.40 | 1.02 |
| F | 27.69 | 5.45 | 0.72 | 30.59 | 5.42 | 0.80 | |
| Aged 56–73 | M | 29.31 | 6.61 | 1.15 | 33.55 | 6.11 | 1.12 |
| F | 24.11 | 5.88 | 0.65 | 27.14 | 4.84 | 0.62 | |
SD: standard deviation; SE: standard error.
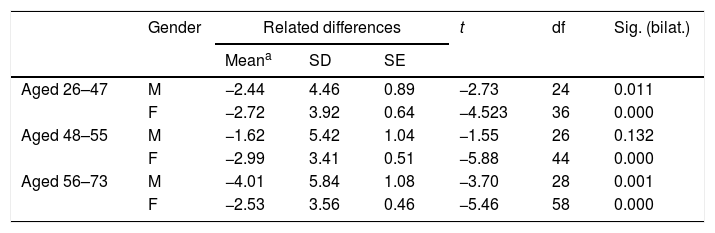
The t test detected significant differences for all age groups and both genders with respect to the initial and final tests. In the 26–47 age group, males had greater differences than females (−2.71 vs 2.28; p<0.01 for both). Meanwhile, in the 48–55 age group, females (−2.52; p<0.05) showed greater differences than males (−3.22; p<0.01). In the oldest age group (56–73) males were found to a significant degree (p<0.01) to have more pronounced differences between the initial and final tests with respect to the whole sample set (Table 3).
T test for related samples associating the initial and final VO2max tests by gender and age.
| Gender | Related differences | t | df | Sig. (bilat.) | |||
|---|---|---|---|---|---|---|---|
| Meana | SD | SE | |||||
| Aged 26–47 | M | −2.44 | 4.46 | 0.89 | −2.73 | 24 | 0.011 |
| F | −2.72 | 3.92 | 0.64 | −4.523 | 36 | 0.000 | |
| Aged 48–55 | M | −1.62 | 5.42 | 1.04 | −1.55 | 26 | 0.132 |
| F | −2.99 | 3.41 | 0.51 | −5.88 | 44 | 0.000 | |
| Aged 56–73 | M | −4.01 | 5.84 | 1.08 | −3.70 | 28 | 0.001 |
| F | −2.53 | 3.56 | 0.46 | −5.46 | 58 | 0.000 | |
SD: standard deviation; SE: standard error.
This study analysed changes in VO2max at the end of a physical exercise programme with subjects with cardiovascular risk factors. The results indicate that there were improvements in VO2max in both males and females after the 10 weeks of the programme.
Results similar to those found in this study have been reported by other authors. In a study with 36 American subjects aged from 60 to 84, improvements in different exercise modalities (endurance, strength and both concurrently) were assessed in terms of maximum strength, functionality and cardiorespiratory fitness, measured by way of a submaximal treadmill test. The findings indicate that the three groups had significant improvements in cardiorespiratory fitness, concluding that concurrent training is more effective than strength or endurance alone for improving cardiovascular fitness.25 In another similar study, Australian adults aged from 40 to 66 who were obese or overweight were subjected for 12 weeks to three types of exercise programme: aerobic endurance (n=15); strength endurance (n=16); and a combination of the two (n=16). The results showed improvements in VO2max in all three groups, with the greatest benefits being found with the combined training, followed by strength training and then aerobic. Similar conclusions were reached in another study, where the benefits on VO2max of concurrent training (strength and aerobic endurance) were assessed in healthy Brazilian adults with an average age of 45.18 In that study, three 40-min sessions per week were held for 24 weeks, where aerobic endurance training (maintaining intensity in the fat-burning zone) was combined within the same session with strength training (squat and bench press); the authors concluded that the training led to significant improvements in VO2max.19 In our study, cardiovascular endurance and muscle strength were kept in separate sessions, with more emphasis given to the strength sessions in the overall number of weeks, and with improvements in VO2max reported for the sample as a whole.
In another study conducted with 24 subjects in the USA with an average age of 70, taking part in a three-month strength-endurance programme was associated with significant improvements of 38% in submaximal cardiorespiratory endurance when walking, on comparing the initial and final tests.27 Similarly, another study with 30 adults aged over 60 in South America who took part in a physical exercise programme for 10 weeks (3sessions/week) reported improvements in VO2max, highlighting the improvement in the respiratory system and vital capacity.29
In our study, males achieved more pronounced improvements than females in 2 of the 3 age ranges studied, with the 48–55 age group being where most improvement was found in the average values among females. We were only able to find one study which examined the difference between males and females with respect to VO2max. In that study, 47 subjects from the southeast of Spain aged over 65 were the subject of an 8-week aerobic training programme; mean VO2max values were found to have improved among females at the end of the programme, but not among the males.26
In our study, the most pronounced improvements in VO2max occurred in the older age groups, specifically in males aged 56–73. In a study with similar age ranges, 76 adults aged 65–70 from the north of Spain were evaluated. A monitored aerobic exercise programme was carried out at a sports centre for 24 weeks with three 1-h sessions/week. Aerobic capacity was assessed by a 6 min field test before and after the intervention. The results showed improvements in aerobic capacity in the group that took part in the programme compared to the control. There were also significant improvements compared to those who only received a medical prescription without monitoring.30
The study with the largest population we were able to find analysed different health parameters with 78 older people aged 65–95 in Portugal. Subjects were divided into three groups: control, aerobic training and strength training. A 16-week programme was carried out with three 45-min sessions/week. The subjects in both groups (strength and aerobic) achieved similar increases in the results for the endurance test, showing that both types of training were effective for improving cardiovascular fitness.28
This study is not without limitations. First of all, despite the fact that the participants were asked not to perform any other physical or sports activities in their free time, it was not possible to objectively control all the physical activity outside the programme. Consequently, there are other factors that may have influenced the subjects’ results. Secondly, the VO2max was obtained by means of an indirect equation extracting the data from a field test; this would have been more accurate performing a laboratory test on a treadmill. However, the large sample to be evaluated led us to choose a standardised field test for the estimation of cardiorespiratory fitness, and thus be able to conduct the measurements within the sports facility where the programme was carried out. There was also a lack of studies on which to base our rationale for some of the analyses we carried out, this being the first study to compare VO2max by age group and gender in subjects with cardiovascular risk factors.
Although it has been demonstrated that medical prescription of physical exercise can by itself improve cardiorespiratory fitness in older people,35 there is evidence of greater benefits from physical exercise monitored and guided by professionals than from simply prescribing it.32,33 This study provides more evidence of the adaptive improvements in VO2max stemming from the physical exercise programmes monitored by professionals in sports centres which patients are referred to from primary care. One solution therefore for improving the VO2max of patients with cardiovascular risk factors and thereby improving their health parameters is for primary care to prescribe these patients monitored physical exercise programmes.
Conflict of interestsThe authors declare that they are independent and do not receive any financial support, with no interests or values affecting the execution of the work and the writing of the manuscript other than those routinely existing in research.
Please cite this article as: Meseguer Zafra M, García-Cantó E, Rodríguez García PL, Pérez-Soto JJ, Tárraga López PJ, Rosa Guillamón A, et al. Influencia de un programa de ejercicio físico terapéutico sobre el consumo máximo de oxígeno en adultos con factores de riesgo cardiovascular. Clin Invest Arterioscler. 2018;30:95–101.