



This study sought to analyze the effects of resistance training on functional performance, lower-limb loading distribution and balance in older women with total knee arthroplasty (TKA) and osteoarthritis (OA) in the contralateral knee. In addition, this older knee OA and TKA group (OKG) was compared to older (OG) and young women (YG) without musculoskeletal diseases who underwent the same resistance training program.
METHODS:Twenty-three women divided into OKG (N = 7), OG (N = 8) and YG (N = 8) had their functional performance, lower-limb loading distribution and balance compared before and after 13 weeks of a twice-weekly progressive resistance training program.
RESULTS:At baseline, the OKG showed lower functional performance and unilateral balance, and impaired lower-limb loading distribution compared to the OG and the YG (p<0.05). After resistance training, the OKG showed improvements in functional performance (∼13% in sit-to-stand and rising from the floor, ∼16% in stair-climbing and ∼23% in 6-minute walking (6 MW)), unilateral balance (∼72% and ∼78% in TKA and OA leg, respectively) and lower-limb loading distribution, which were greater than those observed in the OG and the YG. The OKG showed post-training 6 MW performance similar to that of the OG at baseline. Sit-to-stand performance and unilateral stand balance were further restored to post-training levels of the OG and to baseline levels of the YG.
CONCLUSIONS:Resistance training partially restored functional, balance and lower-limb loading deficits in older women with TKA and OA in the contralateral knee. These results suggest that resistance training may be an important tool to counteract mobility impairments commonly found in this population.
Knee osteoarthritis (OA) is a common age-related clinical condition that has a major impact on function and independence 1, including limitations in walking, stair climbing, rising from a seated or prone position and household chores 2-5. Total knee arthroplasty (TKA) is a highly and increasingly prevalent surgery 6 recommended to those with knee OA showing radiographic evidence of joint damage, moderate to severe persistent pain and clinically significant functional limitations that diminish quality of life 7. Although TKA results in reduced pain and improved perceived function 8, patients continue to exhibit reduced voluntary muscle activation, muscle strength and functional performance even years after surgery 8. Quadriceps muscle strength deficits following TKA have considerable long-term consequences associated with impairments in functional activities (i.e., walking and stair climbing) and lower-limb loading distribution 8,9, as well as the progression of OA in the uninvolved leg 9,10.
Resistance training is the most effective exercise for improving muscle strength 11. The ability to improve muscle strength through resistance training is not affected by the aging process, with both older men and women without physical limitations showing muscle strength improvement and training intensity progression similar to young subjects 12,13. When applied to older subjects with TKA without OA in the contralateral lower extremity, resistance training reduces muscle strength deficits and improves function 4,14,15. However, little is known about the effects of resistance training in older subjects with TKA and symptomatic OA in the contralateral knee.
Previously reported data from this study showed that 13 weeks of a twice-weekly resistance training program partially restored muscle strength in older women with TKA and symptomatic OA in the contralateral knee 16. In this study, the women with TKA and symptomatic OA in the contralateral knee displayed a relative muscle strength increase and resistance exercise intensity progression greater than those of young and older healthy women following the same exercise training program 16. To the best of our knowledge, there is no study analyzing the effects of resistance training on several muscle strength-related impairments commonly found in this population, including functional performance, lower-limb loading distribution and balance.
Increased understanding of the effects of resistance training on the above-mentioned muscle strength-related impairments in subjects with TKA and symptomatic OA in the contralateral knee may help design future therapeutic programs to reduce functional limitations and improve quality of life in this population. Thus, the purpose of the present study was to analyze the effects of a resistance training program on functional capacity, lower-limb loading distribution and balance in older women with TKA and symptomatic OA in the contralateral knee and to compare this group with older and young women without musculoskeletal diseases who performed the same resistance exercise program.
METHODSPopulation and study designA detailed description of the study design, subjects' characteristics and inclusion/exclusion criteria has been previously published 16. In brief, 7 older women with unilateral TKA for at least 14 months (38.5±18.5 months; range, 14-66 months) due to severe OA and an established diagnosis of knee OA 17 in the contralateral limb (Kellgren/Lawrence scale grades 18 of 2-4) (older knee OA and TKA group; OKG), 8 older women without symptomatic musculoskeletal disorders (older control group; OG) and 8 healthy young women (young control group; YG) were recruited from the waiting list of the Cardiovascular and Muscular Fitness Program of the Laboratory of Kinesiology at the Institute of Orthopedics and Traumatology, School of Medicine, University of São Paulo. All volunteers were physically inactive and did not practice resistance training for at least the 12 months preceding the study. The absence of symptomatic musculoskeletal disorders in the OG and YG was assessed during a pre-participation structured interview, according to medical records and after performing clinical evaluations. In these groups, there was no pain during palpation or active movement, no limitation of more than 10% on range of motion during the active movement of large joints (knee, hip, shoulders, trunk, elbow, ankle and wrist), preserved ability to walk fast (30 m) without pain, absence of musculoskeletal disease according to medical records and no pain and/or limitations during the past 10 weeks. All OKG and OG volunteers had controlled hypertension; three OKG volunteers and two OG volunteers had osteopenia; and one OKG volunteer and two OG volunteers had dyslipidemia (simvastatin, n = 3). None of the YG women had any chronic conditions or were taking any medications. The demographic characteristics of the women included in the study are summarized in Table1.
Subjects' characteristics at baseline.
| Variable | OKG | OG | YG |
|---|---|---|---|
| N | 7 | 8 | 8 |
| Age (years) | 75.3±3.1 | 70.4±5.3 | 23.7±3.5 a, b |
| BMI (kg/m2) | 32.4±4.8 | 28.1±5.2 | 23.0±3.4 a, c |
OKG: Older knee OA and TKA group. OG: Older control group. YG: Young control group. N: number of subjects; BMI: body mass index. Significantly different from OKG: a = p<0.001. Significantly different from OG: b = p<0.001; c = p<0.05.
All volunteers had their balance, lower-limb loading distribution and functional capacity (sit-to-stand, rising from the floor, stair-climbing tests and 6-minute walking (6 MW)) assessed and compared before and after participation in the 13-week resistance training program. All measurements were performed in the sequence reported above, both before and after the exercise intervention, by the same technician who was blinded to the research protocol and subject grouping. Muscle strength and exercise intensity progression were also measured and compared between groups and these data were previously published 16. The resistance training program consisted of lower-limb resistance exercises performed twice-weekly. The present study was approved by the Ethics Committee for Analysis of Research Projects of Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (# CAPPesq 447/06). All volunteers read a detailed description of the protocol and provided their written informed consent.
Balance and lower-limb loading distributionBalance function and lower-limb loading distribution were assessed before and after the exercise program (4 days after last exercise session) using a Balance Master® System version 8.1 (NeuroCom International Inc, Clackamas, OR). This system consists of two force plates resting on force transducers that record vertical ground reaction forces and subsequently calculate the center of pressure, sway angles and movement directions. The balance assessment consisted of four tests, including three static and one dynamic test. In the static tests, the center of gravity sway (degrees per second) was measured during three balance tasks on the force plate system, which were performed with the subjects looking straight ahead while barefoot and standing still. The tasks included bilateral stance for 10 s on a firm surface with the eyes open (test 1), bilateral stance for 10 s on a high-density foam block (15-cm closed-cell) with the eyes open (test 2) and unilateral stance (firm surface) on the right and left leg for 10 s with the eyes open (test 3). If loss of balance resulting in a fall (non-tested foot touching the ground) occurred before ending test 3, the test was validated and the center of gravidity sway was recorded as 12 deg/sec, according to the Balance Master® System manual recommendation. Because the 12 deg/sec assumption in case of fall is a recommendation of the manufacturer that may not represent the actual center of gravity sway, the average unilateral stance time was compared before and after training when the fall occurred. During tests 1 and 2, subjects were asked to keep their feet at shoulder width, with their knees extended and arms relaxed along the body. During test 3, subjects were asked to keep the non-tested leg in a position of 0° of hip flexion and 90° of knee flexion and their arms along the body.
Dynamic balance and lower-limb loading distribution were measured during the sit-to-stand test (test 4) with the subjects barefoot. In this test, subjects were asked to rise quickly from a seated to a standing position, during which data were analyzed on weight transfer (time of center of gravity moving from sitting to standing position), rising index (percentage of body weight exerted to rise), end sway (center of gravity movement immediately after standing) and the right/left lower-limb loading symmetry (in percentage) from the sitting to standing position. All subjects performed 3 repetitions of each test and the average was used for data analysis.
Functional performanceMeasures of functional performance included the sit-to-stand, rising from the floor, stair climbing and 6 MW tests. All tests were performed the same day (between 2 and 5 p.m.), before and after the exercise program (4 days after last exercise session), following the sequence described below and with a 3-min rest interval between tests. The sit-to-stand test measured the time taken by subjects to perform 5 repetitions of rising from a standard chair without armrests (seat height of 46 cm) to a full upright position as quickly as possible and without assistance 5. The rising from the floor test measured the time taken by subjects to rise from the supine position (arms along the body) to a full upright position 40 cm ahead of its original position as quickly as possible. The test was performed 3 times (1 min of rest between tries) and the average was used for analysis. The stair climbing test measured as the time taken by subjects to ascend a flight of 15 steps (15 cm high and 30 cm depth) as quickly as possible. The 6 MW test measured the distance covered in 6 min while walking on a programmable treadmill without inclination and with self-controlled velocity, where the subjects were instructed to walk according to Borg's scale, in exertion levels ranging from light to somewhat hard (from 11 to 13) 19, as previously described 20.
Resistance training programThe resistance training program was performed twice weekly for 13 weeks and was designed to develop muscle mass and strength. Each exercise session was monitored by an exercise specialist and consisted of 5 min of warm-up, approximately 15 min of resistance exercise and 5 min of cool down. The resistance exercises were performed unilaterally (both legs were trained) and consisted of two sets of 8-12 repetitions each performed on the leg press, knee curl and calf raise using weight lifting machines (Biodelta Inc., São Paulo, Brazil). The initial workload was set at 60% of the 1-repetition maximum of the weaker leg, as previously reported 16. The volunteers were encouraged to perform at their maximum capacity during the sets of 8-12 repetitions prescribed, using proper form and avoiding the Valsalva maneuver. All subjects were instructed to take a 30- to 60-s rest between sets, which were performed on alternating legs. The exercise specialist also instructed all participants to perform the correct exercise movement during each session. To promote sufficient workload and produce improvements throughout the 13 weeks of training, exercise intensity was increased by 5-10% whenever the subjects had adapted to the exercise workload 16.
Statistical analysesAll data were reported as the mean ± standard deviation. The statistical program Sigma Stat 3.5 for Windows (Systat Software Inc., Chicago, IL, USA) was used for statistical analysis. The Kolmogorov-Smirnov test was applied to ensure a Gaussian distribution of the data. Differences in the volunteers' characteristics and post-exercise muscle strength improvements were analyzed by one-way analysis of variance (ANOVA). Inter- and intragroup comparisons of the data with a Gaussian distribution (functional performance data) were made using two-way ANOVA (group vs. time) with repeated measurements. Bonferroni post-hoc analysis was used to determine significant data indicated by ANOVA. Inter- and intragroup comparisons of the data with a nonparametric distribution (balance and lower-limb loading data) were made using the Kruskal-Wallis and Wilcoxon signed-rank tests, respectively. Dunn's post-hoc test was used to determine significant data indicated by the Kruskal-Wallis test. Because loss of balance resulting in falling occurred only in the OKG, the paired t test was used to compare average unilateral stance time before and after training in this group. The significance level was set at p<0.05.
Based on exercise training studies similar to ours 12,13, the sample size calculation estimated an overall sample of 7 subjects for each age group to provide a power of 80% to detect a muscle strength change of 20% with a two-sided alpha of <0.05, as previously indicated 16.
RESULTSAll subjects completed the 13-week resistance training program. No significant difference between groups was observed in resistance training session compliance (OKG = 89.5±8.4%; OG = 90.2±10.1%; YG = 82.5±12.6%). No injuries, muscle damage or major muscle or joint pain associated with the resistance training program were observed in the three groups during the study period.
Functional performanceFunctional performance data are displayed in Table2. The OKG displayed impaired performance (p<0.05) in the 6 MW, sit-to-stand, rising from the floor and stair climbing tests compared to both the OG and YG at baseline. Baseline performance in the 6 MW, sit-to-stand and rising from the floor tests (but not stair climbing) was also impaired (p<0.05) in the OG when compared to the YG. Resistance training was effective at improving (p<0.01) OKG performance in all functional tests and in improving (p<0.05) OG performance in 6 MW, sit-to-stand and rising from the floor tests. The YG did not show any significant improvement in functional performance during follow-up. Improvements in 6 MW and rising from the floor after resistance training were greater (p<0.01) in the OKG (6 MW = 22.6±11.8%; rising from the floor = 15.5±5.3%) than the YG (6 MW = −1.7±4.8%; rising from the floor = 6.7±4.3%). Post-exercise 6 MW improvement was also greater in the OKG than the OG (13.7±5.8%), but this difference failed to reach statistical significance. With these improvements, the OKG showed post-training 6 MW and sit-to-stand performance similar to the baseline performance of the OG.
Functional capacity before and after 13 weeks of resistance training.
| Test | OKG (N = 7) | OG (N = 8) | YG (N = 8) | |||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |
| 6-min walking (m) | 270±62 | 327±58 c | 485±57a | 550±45 a, c | 626±37 a, b | 614±29 a, b |
| Sit-to-stand (s) | 9.58±1.01 | 7.41±0.80 c | 7.55±0.69 a | 6.51±0.63 c | 6.48±0.53 a, b | 6.44±0.51 a |
| Rising from the floor (s) | 10.04±1.11 | 8.45±0.81 c | 6.11±2.12 a | 5.40±2.20 a, c | 2.89±0.25 a, b | 2.70±0.27 a, b |
| Stair climbing (s) | 10.85±1.62 | 9.36±1.52 c | 5.53±1.28 a | 5.07±1.48 a | 2.79±0.58 a, b | 2.60±0.61 a, b |
OKG: Older knee OA and TKA group. OG: Older control group. YG: Young control group. a: different from OKG during the same period (p<0.05). b: different from OG during the same period (p<0.05). c: different from pre-exercise in same group (p<0.05).
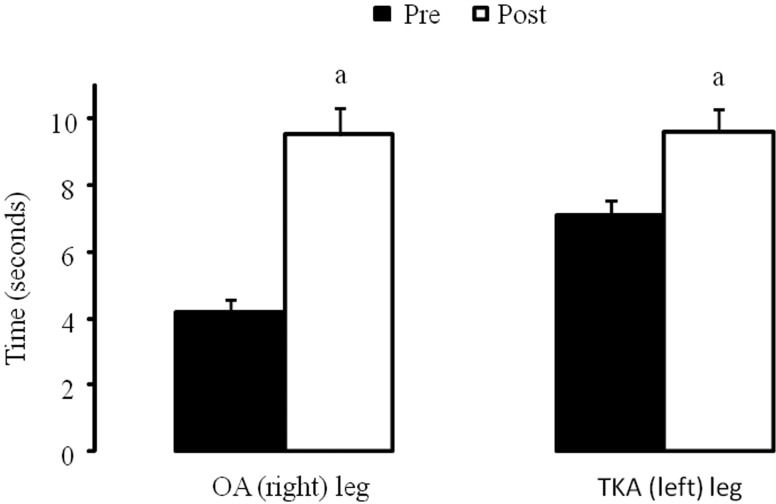
Balance and lower-limb loading distribution data are displayed in Table3. The OKG displayed impairments (p<0.05) in bilateral standing balance on foam surfaces (but not on firm surfaces), unilateral standing balance and rising index in comparison to the OG and YG at baseline. The OKG also showed greater baseline loading distribution deficits than the OG and YG (p<0.05), with greater loading in the TKA than OA leg during the sit-to-stand test. Differences in baseline balance performance were also found between the OG and YG, with the OG showing reduced bilateral standing balance on foam surfaces and unilateral standing balance. The OKG showed improvements in unilateral standing balance (72.2±27.7% and 78.2±30.3% in the TKA and OA leg, respectively), sit-to-stand rising index (12.3±6.1%) and loading distribution (57.6±17.2%) during follow-up (p<0.05). However, bilateral stand balance and sway during sit-to-stand did not change. The OG and YG showed no significant change in balance and loading distribution variables after resistance training. With these results, the OKG restored their unilateral stance balance to levels similar to those observed in the OG, while loading distribution was partially restored. It is imperative to note that the 12 ± 0 deg/sec sway velocity of the OA (right) and TKA (left) leg observed during the pre-training unilateral standing of the OKG occurred because all subjects failed to complete the 3 repetitions of the test without loss of balance, resulting in falling (see methods). However, only 2 OKG subjects failed to complete 1 repetition (but were able to complete the other 2 repetitions) of the unilateral stance test during post-training, which resulted in a significant improvement (p<0.001) in the average unilateral stance time after resistance training (Figure1). None of the individuals in the OG and YG failed to complete any repetition of the unilateral stance test during both pre- and post-training.
Balance and lower-limb loading distribution before and after 13 weeks of resistance training.
| Test | OKG (N = 7) | OG (N = 8) | YG (N = 8) | |||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |
| Bilateral standing | ||||||
| Firm surface (deg/s) | 0.18±0.06 | 0.19±0.06 | 0.26±0.17 | 0.23±0.12 | 0.26±0.21 | 0.18±0.09 |
| Foam surface (deg/s) | 0.85±0.09 | 0.79±0.11 | 1.07±0.26 | 1.01±0.22 | 0.55±0.06 a, b | 0.59±0.13 a, b |
| Unilateral standing | ||||||
| OA/Right leg (deg/s) | 12.0±0.0 | 2.95±4.45 c | 4.8±5.6 a | 4.76±5.6 | 0.68±0.06 a, b | 0.73±0.05 a, b |
| TKA/Left leg (deg/s) | 12.0±0.0 | 3.67±4.13 c | 6.0±5.4 a | 4.73±5.63 | 0.71±0.15 a, b | 0.68±0.10 a, b |
| Sit-to-stand | ||||||
| Weight transfer (s) | 0.27±0.02 | 0.25±0.02 | 0.41±0.35 | 0.34±0.25 | 0.23±0.03 | 0.23±0.03 |
| Rising index (%) | 11.1±0.8 | 12.8±0.7 c | 25.4±9.0 a | 23.8±8.4 a | 29.1±5.4 a | 34.0±6.4 a |
| Loading distribution* (%) | −21.2±4.9 | −9.3±5.2 c | −2.5±3.9 a | 0.6±4.1 a | 4.3±9.4 a | 2.0±5.2 a |
| Sway (deg/s) | 5.4±1.1 | 5.5±0.8 | 4.4±1.4 | 4.1±1.5 | 3.1±1.4 | 3.2±1.1 |
OKG: Older knee OA and TKA group. OG: Older control group. YG: Young control group. OA: Lower-limb with knee OA. TKA: Lower-limb with TKA. a: different from OKG during the same period (p<0.05). b: different from OG during the same period (p<0.05). c: different from pre-exercise in the same group (p<0.05). * Positive values in loading distribution during sit-to-stand indicate grater loading on dominant (OG) or non-operated (OKG) leg, while negative values indicate greater loading on non-dominant (OG) or operated (OKG) leg.
.")
To our knowledge, this is the first study focused on analyzing the effects of a resistance training program on functional performance, lower-limb loading distribution and balance in older women with TKA and OA in the contralateral knee. These results were also compared to those of older and younger women without musculoskeletal diseases who performed the same resistance exercise program. The Baseline baseline characteristics of the OKG were typical to the population of individuals with knee OA or TKA, exhibiting impairments in functional performance and lower-limb loading distribution 2,8,9. The primary finding of the present study was that the resistance training program was a safe and effective intervention to improve functional performance, lower-limb loading distribution and balance among OKG women. Moreover, several resistance training-induced improvements, including those in the 6 MW, rising from the floor, unilateral stand balance, sit-to-stand rising and loading distribution tests, were greater in the OKG compared to both the OG and YG. These improvements in the OKG following resistance training were sufficient to restore the performance in the 6 MW, sit-to-stand and unilateral stand balance tests to levels similar to those observed in the OG at baseline. In addition, sit-to-stand performance and unilateral stand balance were also restored to post-training OG and baseline YG levels.
Although there is a paucity of studies analyzing the effects of resistance training in subjects with both TKA and OA in the contralateral knee, the beneficial effects of resistance training on functional performance has been shown in the early 14 and late 4 rehabilitation phases after TKA, as well as in subjects with only knee OA 21,22. In subjects with unilateral TKA without OA in the contralateral knee, a lower-limb resistance exercise program beginning 3−4 weeks after surgery resulted in improvements in stair climbing and 6 MW performance during a 12-month follow-up period that were greater than the improvements observed in subjects who received a standard rehabilitation program 7. A thrice-weekly resistance exercise program performed for 12 weeks by subjects that had unilateral (without symptomatic OA in the contralateral knee) or bilateral TKA for 1−4 years resulted in ∼8.6% and ∼16.7% improvement on 6 MW and stair climbing performance, respectively 4. Although 6 MW distance did not change in middle-aged subjects with knee OA after 12 weeks of a thrice-weekly resistance exercise program 22, greater improvements in stair-climbing and sit-to-stand performance in older women with knee OA were observed after 4 months of a resistance exercise program when compared to a control group receiving an educational program 21. In this context, the resistance training-induced improvements on 6 MW, sit-to-stand and stair climbing performance observed in this study are in accordance with previous studies that evaluated subjects with only TKA or knee OA.
Several studies have shown that a decline in balance performance is a hallmark of the aging process 23-26. For example, decline in unilateral standing stability, a clinical measure for higher-level balance ability 23,27, has been demonstrated for women in their 40 s, with significant decline during each subsequent decade 24. However, little is known about the balance performance in subjects with TKA or knee OA. The present study shows that older women with TKA and OA in the contralateral knee have impaired balance performance than both young and older healthy women. Although no significant difference between the OKG and OG was observed in the bilateral standing balance on both firm and foam surfaces, the OKG displayed greater instability during unilateral standing than both the YG and OG at baseline. Resistance training was effective at improving unilateral standing balance in the OKG, resulting in significant ∼72% and ∼78% reductions in sway when standing on the TKA and OA leg, respectively. It is important to emphasize that resistance training-induced improvement was sufficient to restore unilateral standing balance of both the TKA and OA legs to levels similar to those observed in the OG. As falls are a growing problem with significant economic, personal and social costs among elderly people 28-30 and the inability to stand on one leg has been shown to be an important predictor of serious falls in older individuals 31, the resistance training-induced improvement in unilateral standing balance observed in the OKG may have important implications in fall prevention and its consequences in this specific population. Additional longitudinal studies investigating the impact of these balance improvements on fall risk are needed.
Another important finding of the present study was that women in the OKG displayed increased TKA leg loading during the bilateral sit-to-stand task. This finding is in contrast to the reduced TKA leg loading observed during the sit-to-stand task at 3 months after surgery in older subjects without symptomatic OA in the contralateral limb 9. Differences in time from surgery (3 vs. ∼38.5 months) and characteristics of the contralateral leg (asymptomatic vs. symptomatic OA) in the populations studied are possible explanations for these discrepant findings 9. The resistance training program was also effective in reducing the deficits on lower-limb loading during the sit-to-stand task. The deficits between the legs improved from −21.2±4.9% to −9.3±5.2% loading on the OA leg after the 13-week resistance training. Because the altered loading distribution during bilateral tasks observed in the early phase after TKA may have important long-term consequences for OA progression in the uninvolved leg 9,10, it appears reasonable to suggest that the opposite loading pattern observed in the OKG, which would overload joints of the TKA leg during daily living bilateral support tasks, may also have important long-term consequences, including reduced implant lifespan and early need for revision surgery 32. In this context, the resistance training-induced improvement in lower-limb loading may have important clinical implications.
One probable mechanism that may explain the resistance exercise-induced improvements in functional performance, balance and lower-limb loading distribution is the enhancement of muscle strength and endurance. Lower muscle strength, in particular quadriceps strength, has been advocated as the main contributor to the reduced functional performance and altered lower-limb loading distribution commonly observed in older subjects with TKA or knee OA 4,8,9,14,22,23,33. Although muscle strength data are not reported in the present manuscript, previously reported data from this study showed lower baseline muscle strength among OKG women, especially in the OA leg 16. This previous report also showed that the OKG demonstrated a greater muscle strength increase after the 13-week resistance training program. Greater improvements were even observed in the OA leg, which were enough to restore the OA leg muscle strength levels of the OKG to those of the OG at baseline, as well as to reduce the muscle strength deficits between legs 16. One must argue that knee pain is another factor common to individuals with knee OA that can influence functional performance and lower-limb loading 34,35. For example, non-operated knee pain was the primary contributor to performance on the stair climbing and 6 MW tests in patients 3 years after TKA 34. In contrast, resistance training has led to reduced pain in individuals with knee osteoarthritis 21. Therefore, it is possible that the greater improvement in functional performance and balance, as well as the reduction in lower-limb loading distribution deficits may have been mediated, at least in part, by pain reduction in the OA knee of the OKG. However, no pain measures were performed in the present study to confirm this hypothesis.
Poor functional performance levels have been associated with increasing rates of disability and daily living dependence 36,37, as well as a higher risk for mortality and nursing home admission 38. For example, older subjects aged 70 to 79 years with the 5-repetition sit-to-stand time above 12.6 s can be considered to have a lower-than-average performance 39. Older subjects aged 65 to 99 years performing the 5-repetition sit-to-stand test above 13.5 seconds displayed a greater risk (20% to 420%) of having mobility-related disability after 2 years of follow-up 37. Although both the OKG and OG showed baseline sit-to-stand performance below the above-mentioned cut-off points, the resistance training-induced improvements in functional performance of both the OKG and OG observed in the present study may have important clinical implications by helping to reduce the risk of future disability and to increase the number of years with daily living independence.
It is important to note that the YG failed to demonstrate functional improvements after the resistance training program, which could be due to insufficient exercise intensity in this population. The resistance training intensity was sufficient to promote YG muscle strength increases similar to those observed in the OG 16 and to those observed in previous studies 12,13, suggesting that the failure of the YG to demonstrate functional improvements was likely due to a ceiling effect of muscle strength on these variables.
The results of the present and previous studies suggest that the ceiling effect of muscle strength on balance performance seems to be even more pronounced. Although the association between lower-limb muscle strength and balance in older people has been shown in cross-sectional studies 40-42, it appears to be weaker in older individuals without limitations 40 compared to older individuals with limitations 11. Previous studies have failed to show any resistance training-induced improvement in balance performance in older subjects without limitation 43,44, while older adults identified at the highest risk for fall were shown to benefit from exercise programs including resistance training 11. In this context, it has been proposed that the beneficial effects of resistance training on balance performance likely occur in the older population with greater limitations 11. Thus, the present resistance training-induced improvement in balance performance observed in the OKG, but not in the OG and YG, supports this hypothesis.
The present study has several limitations that must be addressed. First, although the statistical power of the present sample is adequate, caution must be taken in generalizing the present results. The small number of women studied may not represent the greater population of patients with knee OA and TKA. Second, the present data cannot be generalized to men because our population was composed strictly of women. Third, the lack of a no-exercise control group must be noted. One could argue that operated patients (OKG), fearing a new surgery if the exercise fails, may give more attention to the exercise program and could improve in a second evaluation even without the proposed exercises. However, previous studies with only TKA subjects showed no improvement in functional performance in no exercise or standard physical therapy control groups, suggesting that the fear of a new operation would not improve these variables 4,7,14. Moreover, the total or partial restoration of OKG functional performance, lower-limb loading distribution and balance levels to those of healthy older women performing the same exercise program reinforces the benefits of resistance training among older women with TKA and OA in the contralateral knee. Fourth, the 12 deg/sec assumption in case of falling does not represent the real value of center of gravity sway during the unilateral stance test; rather, this value is a recommendation from the manufacturer for research and clinical purposes. Moreover, the fact that all OKG women failed to complete the 3 repetitions of the unilateral stance test without loss of balance resulting in falls before training and that only 2 women failed to complete 1 repetition (but were able to complete the other 2 repetitions) after training, which resulted in a significant improvement in average unilateral stance time after training, shows that unilateral stance balance was improved during follow-up in OKG women. Finally, the follow-up period was rather short, warranting additional studies with a no-exercise control group; in particular, long-term follow-up focused on analyzing end points such as radiographic evaluation of disease progression or second TKA may offer additional compelling evidence for the validity of the present resistance training program.
In summary, resistance training was an effective and safe intervention to improve functional performance, lower-limb loading distribution and balance in older women with TKA and OA in the contralateral knee. These improvements were greater than those observed in older and younger healthy women performing the same resistance training program, resulting in total or partial restoration of several variables, including 6 MW and sit-to-stand performance, unilateral stand balance and lower-limb loading distribution. Although future studies with a no-exercise control group, larger sample size and longer follow-up period are required to confirm the present findings, this study suggests that resistance training may be an effective method to counteract the impairments in functional performance, balance and lower-limb loading distribution in older women with TKA and OA in the contralateral knee.
AUTHOR CONTRIBUTIONSCiolac EG participated in the study design, data collection, analysis and manuscript preparation. Rodrigues da Silva JM participated in the data collection, analysis and manuscript preparation. Greve JM participated in the study design and manuscript preparation.
No potential conflict of interest was reported.