





Type 1 diabetes mellitus (T1DM) is one of the most common chronic diseases in childhood. An increased incidence of T1DM has recently been noted in children under 15 years of age, and especially in the younger group. The purpose of this study was to know the incidence of T1DM in Asturias and its characteristics.
Material and methodsChildren and young adults under 40 years of age living in Asturias and diagnosed with T1DM in public and private centers from January 1, 2002 to December 31, 2011, were included in the study. Information collected included age, sex, date of diagnosis, initial symptoms, and biochemical parameters of the disease.
ResultsA total of 436 patients were diagnosed, of whom 59.63% were males; 169 were younger than 15 years, 56.8% of them males. The age-adjusted overall incidence rate (IR) in Asturias of people diagnosed with diabetes before 40 years of age during this period was 9.45/100.000 population/year (95% CI: 8.58–10.38), 11.07 in males (95% CI: 9.77–12.50) and 7.77 in females (95% CI: 6.66–9.00). In subjects under 30 years of age, IR rate was 10.82 (95% CI: 9.67–12.07), 11.91 in males (95% CI: 10.23–13.78) and 7.61 in females (95% CI: 6.25–9.17). The IR in subjects younger than 15 years of age was 15.60 (95% CI: 13.33–18.13), 17.24/100,000 population/year (95% CI: 13.97–21.06) in males and 13, 86 (95% CI: 10.86–17.42) in females.
Estimated IR adjusted by age group in children under 15 years of age was 9.58 (95% CI: 6.64–13.39) in those aged 0–4 years, 18.25 in those aged 5–9 years (95% CI: 14.06–23.31), and 18.78 (95% CI: 14.67–23.69) between 10 and 14 years of age.
IR remained stable in virtually all age groups and in both sexes, except in girls under 4 years of age, who showed a significant upward trend.
There were significant differences in incidence between the central area of Asturias, predominantly urban, and the peripheral areas, mainly devoted to farming and livestock breeding. Thus, while IR in Mieres was 8/100,000/year, in Jarrio reached 25.6/100,000/year.
ConclusionIn Asturias, incidence of T1DM in children and young adults is similar to that of the surrounding communities, but lower than the average in Spain. It has remained stable in recent years, except in the younger girls (in whom it has increased), and shows a great geographical variability between the center of the region and the periphery.
La diabetes mellitus tipo 1 (DM1) es una de las enfermedades crónicas más frecuentes en la infancia. En los últimos años se observa un aumento de la incidencia de esta enfermedad en los menores de 15 años y sobre todo en el grupo de edad más joven. EL objetivo de este estudio es conocer la incidencia de la DM1 en Asturias y sus características.
Material y métodosSe incluyeron en el estudio los niños y jóvenes adultos de menos de 40 años, residentes en Asturias y diagnosticados de DM1 en los centros públicos y privados entre el 1 de enero de 2002 hasta el 31 de diciembre de 2011. Se recogió información sobre edad, sexo, fecha al diagnóstico, síntomas iniciales y parámetros bioquímicos de la enfermedad.
ResultadosSe diagnosticaron 436 pacientes; de ellos, el 59,63% eran hombres; 169 eran menores de 15 años, de los cuales el 56,8% eran hombres. La tasa de incidencia global ajustada por edad (TI) en Asturias para los diabéticos diagnosticados antes de los 40 años durante este periodo fue de 9,45/100.000 habitantes/año (IC95%: 8,58-10,38); para los hombres fue de 11,07 (IC95%: 9,77-12,50) y para las mujeres, de 7,77 (IC95%: 6,66-9,00). En los menores de 30 años la TI fue de 10,82 (IC95%: 9,67-12,07), 11,91 (IC95%: 10,23-13,78) en los hombres y 7,61 (IC95%: 6,25-9,17) en las mujeres. Para los menores de 15 años la TI fue de 15,60 (IC95%: 13,33-18,13), 17,24/100.000 habitantes/año (IC95%: 13,97-21,06) en hombres y 13,86 (IC95%: 10,86-17,42) en mujeres.
Si estimamos la TI ajustada por grupos de edad, en los menores de 15 años observamos que entre 0 y 4 años de edad la TI es de 9,58 (IC95%: 6,64-13,39), entre 5 y 9 años es de 18,25 (IC95%: 14,06-23,31), y entre 10 y 14 años es de 18,78 (IC95%: 14,67-23,69).
La incidencia ha permanecido estable en este decenio en prácticamente todos los grupos de edad y sexo, excepto en las niñas menores de 4 años, en las cuales muestra una tendencia significativa al alza.
Se observan importantes diferencias en la incidencia entre el área central de Asturias, predominantemente urbana, y las zonas periféricas, predominantemente agrícolas y ganaderas; así la incidencia en Mieres es del 8/100.000/año, mientras en Jarrio llega al 25,6/100.000/año.
ConclusiónEn Asturias la incidencia de DM1 en niños y jóvenes es comparable a la de las comunidades de nuestro entorno, aunque por debajo de la media de España; permanece estable en los últimos años excepto en las niñas más pequeñas, en quienes aumenta, y presenta una gran variabilidad geográfica entre el centro de la región y la periferia.
Type 1 diabetes mellitus (DM1) is one of the most common chronic diseases in childhood. Projects such as EURODIAB in Europe,1 DIAMOND worldwide,2,3 and other more recent initiatives such as the SEARCH for Diabetes in Youth Study in the United States,4 compile information on the incidence, risk factors and mortality associated with DM1; evaluate the efficacy and efficiency of the medical care of these patients; and allow planning of the resources needed to cope with this health problem.
An increase in the incidence of DM1 has been observed in recent years among individuals under 15 years of age, and particularly in the 0–4 years age group. It is estimated that the worldwide incidence of the disease grows 3% annually, with 86,000 new cases each year.1
According to the International Diabetes Federation (IDF), Spain is a country with a high incidence of DM1 (between 10 and 25/100,000 inhabitants under 15 years of age).5 Based on the studies made in different Spanish Autonomous Communities, the estimated interval in this country ranges between 7.9 in Mallorca5 and 30–35 in some parts of the Canary Islands.6,7
The most recent data available in Asturias on diabetes in children between 0 and 14 years of age date back to 1998.8 This study included all children diagnosed in Asturias between 1 January 1991 and 31 December 1995, with data from the hospitals and primary care centers of the 8 public healthcare areas (SESPA) in the Community, and from private clinics. A total of 126 cases of DM1 were diagnosed, representing an incidence of 11.5/100,000 inhabitants/year.
The incidence of DM1 shows important variations worldwide, between countries – including those in Europe1,9 – and between regions within the same country.10–12
Carrying out epidemiological studies constitutes a priority recommendation in diabetes research. Due to the prevalence and increase in the incidence of DM1 worldwide, it is one of the chronic diseases in which studies in a concrete population are required in order to know the factors underlying its pathogenesis and to establish the necessary social and health resources.
The aim of the present study was to ascertain the epidemiology of DM1 in the Autonomous Community of Asturias and to describe the characteristics of the presentation of the disease. Once the population of our Community has been characterized and the most important etiopathogenic risk factors have been defined, prevention programs can be developed. According to EURODIAB, a 70% increase in the prevalence of DM1 can be expected in subjects under 15 years of age by the year 2020.1
Material and methodsThe study compiled the identifying and clinical data corresponding to all children and adults under 40 years of age living in our Community and diagnosed with DM1 at the start of the disease in the public and private healthcare centers of Asturias during the period between 1 January 2002 and 31 December 2011. Use was made of the capture–recapture method, employing as primary source the codes of the International Classification of Diseases – Ninth Edition (ICD9) of the Services of Endocrinology, Internal Medicine and Pediatrics of all the public and private hospitals in Asturias. As a secondary source we used the Primary Care electronic case history records of the entire Community; the case registries of the private clinics of specialists in Endocrinology; and the records of the Diabetics Association of Asturias (Asociación de Diabéticos del Principado de Asturias [ASDIPAS]). The exhaustiveness of the primary source was 99.6%, with no yearly variations, whereas the secondary sources were of very limited use, since only three cases were detected.
The study involved a descriptive observational design, with the compilation of information referring to age at onset, gender, origin, date of diagnosis, starting symptoms and biochemical parameters of the disease in all the patients diagnosed with DM1 in Asturias and who had been living for at least 12 months in the Community.
The following diagnostic criteria for DM1 were used: compliance with the clinical characteristics for the diagnosis of diabetes as established by the American Diabetes Association (ADA), positivity for anti-GAD antibodies and/or anti-IA2 antibodies and/or islet cell antibodies (ICA), and the need for sustained insulin treatment within less than 6 months following diagnosis. In the event that no antibody determinations were made, or if the determinations proved negative, the clinical characteristics of the diagnosis were assessed, along with the need for sustained insulin treatment within less than 6 months following diagnosis, and the professional criterion of the physician attending the patient.
For the calculation of the incidence rates (IRs) we used the data of the Spanish National Institute of Statistics for the Community of Asturias and for each of its 8 healthcare areas in each year. We estimated the annual rates and the rates per 100,000 inhabitants in risk year, by age and gender groups, and per healthcare area. The 95% confidence intervals (95% CIs) were estimated following the Poisson distribution. A Poisson regression model was generated to explore possible trends/changes in the studied period. Microsoft Excel and the SPSS version 24 statistical package (IBM) were used for the statistical analysis. The study was approved by the Clinical Research Ethics Committee of Hospital Universitario Central de Asturias.
ResultsIn the decade 2002–2011, a total of 436 patients under 40 years of age were diagnosed with DM1; of these, 260 were males (59.63%). A total of 169 patients were under 15 years of age (56.8% males), while 320 patients were under 30 years of age (180 males; 56.25%). Data for anti-GAD antibodies and/or anti-IA2 antibodies were available in 358 cases, with positivity to some of them in 324 cases (90.5%).
The overall IR adjusted for age in Asturias for the patients diagnosed with diabetes before the age of 40 during this period was 9.45/100,000 inhabitants/year (95% CI: 8.58–10.38). In the case of males the ratio was 11.07 (95% CI: 9.77–12.50) and in females the ratio was 7.77 (95% CI: 6.66–9.00).
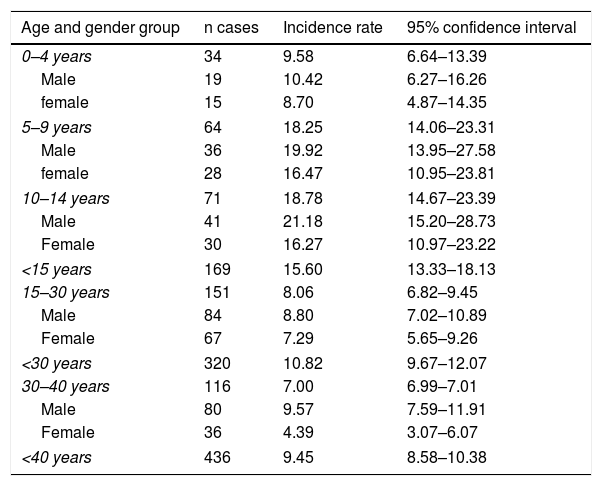
Among the subjects under 30 years of age the IR was 10.82 (95% CI: 9.67–12.07). In the case of males the ratio was 11.91 (95% CI: 10.23–13.78) and in females the ratio was 7.61 (95% CI: 6.25–9.17). In the subjects under 15 years of age the IR was 15.60 (95% CI: 13.33–18.13), with 17.24/100,000 inhabitants/year (95% CI: 13.97–21.06) in males and 13.86 (95% CI: 10.86–17.42) in females (Table 1).
Incidence rates per 100,000 inhabitants/year, and age and gender groups.
| Age and gender group | n cases | Incidence rate | 95% confidence interval |
|---|---|---|---|
| 0–4 years | 34 | 9.58 | 6.64–13.39 |
| Male | 19 | 10.42 | 6.27–16.26 |
| female | 15 | 8.70 | 4.87–14.35 |
| 5–9 years | 64 | 18.25 | 14.06–23.31 |
| Male | 36 | 19.92 | 13.95–27.58 |
| female | 28 | 16.47 | 10.95–23.81 |
| 10–14 years | 71 | 18.78 | 14.67–23.39 |
| Male | 41 | 21.18 | 15.20–28.73 |
| Female | 30 | 16.27 | 10.97–23.22 |
| <15 years | 169 | 15.60 | 13.33–18.13 |
| 15–30 years | 151 | 8.06 | 6.82–9.45 |
| Male | 84 | 8.80 | 7.02–10.89 |
| Female | 67 | 7.29 | 5.65–9.26 |
| <30 years | 320 | 10.82 | 9.67–12.07 |
| 30–40 years | 116 | 7.00 | 6.99–7.01 |
| Male | 80 | 9.57 | 7.59–11.91 |
| Female | 36 | 4.39 | 3.07–6.07 |
| <40 years | 436 | 9.45 | 8.58–10.38 |
On estimating the IR adjusted according to age groups, we found that in subjects under 15 years those between 0 and 4 years of age presented an IR of 9.58 (95% CI: 6.64–13.39), those between 5 and 9 years presented an IR of 18.25 (95% CI: 14.06–23.31), and those between 10 and 14 years presented an IR of 18.78 (95% CI: 14.67–23.69).
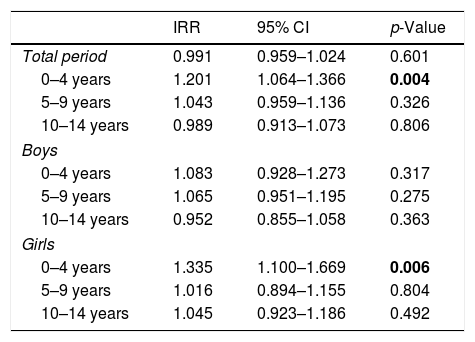
Looking at the year by year incidence (Table 2) adjusted for age during this period of time, the IR was seen to vary between 7.96 and 10.82/100,000 inhabitants/year in the 0–40 years age range. Among individuals under 15 years of age, the lowest incidence corresponded to the year 2003, with 7.60/100,000 inhabitants/year, and the highest to 2009, with 18.84/100,000 inhabitants/year. The Poisson regression model revealed no significant variation in incidence in this period (p=0.601) for the global study population, with a mean variation of −0.90% (95% CI: −4.1 to 2.4%). Likewise, no significant variation was observed among those under 15 years of age. On examining the sample according to age groups, a significant increase in incidence was observed among girls between 0 and 4 years of age (Table 3).
Annual incidence rates per 100,000 inhabitants/year, according to age groups.
| <40 years | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|---|---|---|
| n cases | 40 | 50 | 47 | 48 | 45 | 42 | 41 | 49 | 39 | 35 |
| IR | 8.25 | 10.43 | 9.96 | 10.27 | 9.74 | 9.22 | 9.04 | 10.82 | 8.72 | 7.96 |
| CI− | 5.89 | 7.74 | 7.32 | 7.57 | 7.11 | 6.65 | 6.49 | 8.00 | 6.2 | 5.54 |
| CI+ | 11.23 | 13.75 | 13.24 | 13.62 | 13.04 | 12.47 | 12.26 | 14.3 | 11.92 | 11.07 |
| <15 years | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|---|---|---|
| n cases | 20 | 8 | 15 | 15 | 19 | 15 | 15 | 21 | 21 | 20 |
| IR | 18.81 | 7.60 | 14.36 | 14.17 | 17.84 | 14.00 | 13.83 | 18.84 | 18.54 | 17.42 |
| CI− | 11.49 | 3.28 | 8.04 | 7.93 | 10.74 | 7.84 | 7.74 | 11.66 | 11.47 | 10.64 |
| CI+ | 29.05 | 14.97 | 23.69 | 23.37 | 27.86 | 23.1 | 22.81 | 28.79 | 28.34 | 26.91 |
Incidence rate ratios in individuals under 15 years of age.
| IRR | 95% CI | p-Value | |
|---|---|---|---|
| Total period | 0.991 | 0.959–1.024 | 0.601 |
| 0–4 years | 1.201 | 1.064–1.366 | 0.004 |
| 5–9 years | 1.043 | 0.959–1.136 | 0.326 |
| 10–14 years | 0.989 | 0.913–1.073 | 0.806 |
| Boys | |||
| 0–4 years | 1.083 | 0.928–1.273 | 0.317 |
| 5–9 years | 1.065 | 0.951–1.195 | 0.275 |
| 10–14 years | 0.952 | 0.855–1.058 | 0.363 |
| Girls | |||
| 0–4 years | 1.335 | 1.100–1.669 | 0.006 |
| 5–9 years | 1.016 | 0.894–1.155 | 0.804 |
| 10–14 years | 1.045 | 0.923–1.186 | 0.492 |
Age groups with a significantly higher incidence rate appear in boldface.
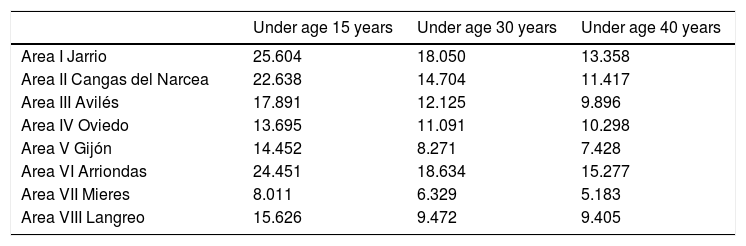
Examining the IR according to geographic zones, and taking as reference the 8 healthcare areas of Asturias, important differences were noted between the central areas and the peripheral areas (see Table 4), since the ratio among individuals under 15 years of age varied from 8/100,000 inhabitants/year in Mieres to 25.6/100,000 inhabitants/year in Jarrio. Less marked differences were also seen in other age groups.
Incidence rate according to geographic area.
| Under age 15 years | Under age 30 years | Under age 40 years | |
|---|---|---|---|
| Area I Jarrio | 25.604 | 18.050 | 13.358 |
| Area II Cangas del Narcea | 22.638 | 14.704 | 11.417 |
| Area III Avilés | 17.891 | 12.125 | 9.896 |
| Area IV Oviedo | 13.695 | 11.091 | 10.298 |
| Area V Gijón | 14.452 | 8.271 | 7.428 |
| Area VI Arriondas | 24.451 | 18.634 | 15.277 |
| Area VII Mieres | 8.011 | 6.329 | 5.183 |
| Area VIII Langreo | 15.626 | 9.472 | 9.405 |
During the study period 2002–2011, the global IR corresponding to DM1 in Asturias among individuals under 15 years of age was 15.59/100,000 inhabitants/year. This figure is below the average recorded for Spain as a whole,13 17.69/100,000 inhabitants/year, which is regarded by the World Health Organization (WHO) as a high figure, but is consistent with the data found in other Communities in the north of the country, such as Galicia14 with 17.2, Navarra15 with 16.48, Cantabria16 with 13.8, and the Basque Country11 with 11.6/100,000 inhabitants/year. Although the Spanish data are highly variable, and not all the studies are comparable,13 historically the incidence in the north of the country has been lower than in the south, and the north-south gradient reported in studies in other European countries1 cannot be applied to Spain. This is confirmed by the findings of the present study.
As in the majority of studies, the highest incidence was recorded in the 10–14 years age group,15 though the figure was practically the same as in the 5–9 years age group. By contrast, in Navarra the incidence was substantially greater in the 10–14 years age group.
The incidence in individuals between 15 and 30 years of age was slightly higher than half the figure recorded in subjects under 15 years of age (8.06/100,000 inhabitants/year), and this incidence in turn decreased slightly between 30 and 40 years of age (7.00/100,000 inhabitants/year). Few data are available in the literature in relation to these age groups in Spain, but this incidence is clearly lower than that found in Navarra,10 and also lower than the figures recorded in other European countries.17,18 Between 30 and 40 years of age the incidence remained at levels similar to those documented in the 15–30 years age group, as in Italy,19 while in other studies such as that made in Navarra,10 a significant decrease was observed.
With regard to the study carried out in Asturias in 1998 (IR: 11.5/100,000 inhabitants/year),8 a clear and very significant increase in incidence was noted (p<0.001), though the methodology used in the two studies is not fully comparable. According to the 1998 study, the number of new expectable cases per year was 13 in the population under 15 years of age. However, on establishing calculations according to the incidence found for the period 2002–2011, the number of new cases was 17, most of which correspond to the 10–14 years age group. It can, therefore, be concluded that there has been a significant increase in the number of patients developing DM1 in this period.
In our study, the IR of DM1 was significantly higher in males (11.07/100,000 inhabitants/year) than in females (6.44/100,000 inhabitants/year) and, as can be seen in Table 1, this difference was observed in all age groups. This same difference favorable to males can be found in other studies, both in our country20 and elsewhere in Europe.2,3
The evolution of the annual incidence during the analyzed period (2002–2011) has remained without significant changes during the entire decade, with the lowest IR corresponding to the year 2003 (7.60/100,000 inhabitants/year) and the highest to 2009 (18.84/100,000 inhabitants/year). These differences are nonsignificant. As can be seen in Table 2, although a slight increase was noted during the years 2005–2007 in males, together with a slight decrease in females, the global IRs experienced very little change. On analyzing the age groups, we only found a slight increase in girls under four years of age, which is consistent with the data recorded in other European studies.21
In recent years the incidence in other Communities of northern Spain such as Galicia,12 Cantabria,16 the Basque Country11 and Catalonia22 has also remained stable in a way similar to the situation seen in our own Community. In other parts of Spain such as Navarra, the incidence clearly increased, particularly in the youngest age group.23 A rise in incidence has also been observed in Málaga,24 Valencia and to a lesser degree in Aragón.25 Other countries such as the United Kingdom have noted a sustained increase in incidence in all age groups in recent years.18
The incidence of DM1 in children is rising in many countries, particularly among those under 15 years of age. There are clear geographic differences in the trends, though the total annual increment is estimated to be about 3%.3 Furthermore, several European studies have suggested that in relative terms, the increase is greater among the youngest children.1 However, based on the results of our study, as well as on the most recent findings corresponding to other Communities in the north of Spain, the incidence over the last two decades has remained stable, the highest incidence being found in the 10–14 years age group for both genders.10,12,26
Large differences were observed on examining the incidence of DM1 in the different areas of the Community of Asturias. In this regard, central Asturias, which is predominantly urban, showed a notably lower incidence than the peripheral areas, which are predominantly rural. Such geographic differences have also been documented elsewhere in our country (Navarra, Catalonia)10,22,27 and in other European countries such as Sweden.28 Although comparison with previous data is not possible, these differences could be explained by genetic parameters or environmental factors such as diet,29 metals,30 water pH31 or the presence of pesticides.32 This marked geographic variability in the incidence of DM1 in Asturias requires the generation of hypotheses and the conduction of new studies.
To summarize, it can be affirmed that the incidence of DM1 in children and young adults is comparable to that found in other Communities in our setting, but is lower than the average for Spain as a whole. The incidence has remained stable in recent years and exhibits great geographic variability between the center of the region and its periphery. We consider that a DM1 registry should be implemented in Asturias in order to facilitate the epidemiological study of the disease.
Conflict of interestNone.
Thanks are due to all the endocrinologists and pediatricians in Asturias, in both the public and private centers, for the work done in relation to the diagnosis and contribution of data; to the documentation and filing staff of all the hospitals in the region; and also to Tania Iglesias of the statistical department of the University of Oviedo.
Please cite this article as: Mayoral González B, Riaño Galán I, Rodriguez Dehli C, Labra Alvarez R, Díaz Naya L, Menéndez Torre E. Epidemiología de la diabetes tipo 1 en Asturias: 2002–2011. Endocrinol Diabetes Nutr. 2018;65:68–73.
