





A 45-year-old woman suffering from primary hypothyroidism, previously well substituted with levothyroxine, was urgently referred from Primary Care to Endocrinology due to very elevated thyrotropin, free thyroxine at low limit of normality, very high cholesterol and generalised oedema. Hypothyroidism was suspected as the main aetiology of this clinical condition. A detailed examination showed nephrotic range proteinuria and the patient was finally diagnosed with lupus nephritis. Urinary loss of thyroid hormones, fundamentally linked to their transport proteins, in patients affected by nephrotic syndrome is sometimes a forgotten phenomenon and one which should be considered in patients with increased levothyroxine requirements. In this report, we present the details of this case and a brief review of the literature on this topic.
Mujer de 45 años con hipotiroidismo primario, previamente bien sustituido con levotiroxina, remitida de urgencia desde Atención Primaria a Endocrinología por tirotropina muy elevada, tiroxina libre en límite bajo de la normalidad, colesterol muy elevado y edema generalizado. Se sospechó hipotiroidismo como principal etiología de este cuadro clínico. Un examen detallado mostró proteinuria de rango nefrótico y la paciente fue finalmente diagnosticada de nefritis lúpica. La pérdida urinaria de hormonas tiroideas, ligada fundamentalmente a sus proteínas transportadoras, en pacientes afectos de síndrome nefrótico es a veces un fenómeno olvidado y que debe tenerse en cuenta en pacientes con requerimientos elevados de levotiroxina. En este artículo presentamos los detalles de este caso y una breve revisión de la literatura sobre este tema.
A 42-year-old woman consulted for symptoms of asthenia, poorly quantified weight loss, diarrhoea and palpitations, with a five-month history. She also complained of itchy eyes and swollen eyelids. As a previous medical history, she presented penicillin allergy, she was a smoker of 10cigarettes/day and she had suffered from epilepsy since childhood, which remained stable and without crisis in recent years. She was not taking any pharmacological treatment. Physical examination showed a diffuse goitre, erythematous and retracted eyelids, and conjunctival redness. Heart auscultation revealed rhythmic tones, without murmurs, with a frequency of 96 beats per minute. A blood test displayed primary hyperthyroidism [thyrotropin (TSH)<0.01μU/ml (reference range – RR: 0.4–4.0), free thyroxine (FT4) 5.33ng/dl (RR: 0.8–1.9)] and positive anti TSH receptor antibodies [22.96mU/ml (RR: <1.75)]. She was diagnosed with Graves–Basedow disease, accompanied by mild thyroid ophthalmopathy and treatment with methimazole 25mg/day, propranolol 10mg every 8h, and selenium 200μ/day was started. The patient showed good response to methimazole and FT4 levels decreased, so the antithyroid drug dose could be reduced. In contrast, the ophthalmopathy worsened and inflammatory signs became more evident reaching a Clinical Activity Score (CAS) of 3/7. An orbital magnetic resonance imaging (MRI) was performed, which showed eye muscle thickening, with signs of acute inflammation, in the inferior, lateral, and superior rectus muscles of both eyes. Based on those findings, treatment with intravenous pulses of methylprednisolone was started. Response to corticosteroids was good and ocular inflammatory signs improved very significantly. FT4 levels remained controlled with doses of 5–10mg/day of methimazole but increased if an attempt to reduce the dose or stop the treatment was made. Thus, approximately sixteen months after the onset of disease, the need for definitive treatment of hyperthyroidism was raised. The use of radioiodine was ruled out due to a history of severe thyroid ophthalmopathy. Therefore, a total thyroidectomy was performed without any complications. Anatomopathological analysis of the surgical specimen reported diffuse hyperplasia of thyroid gland. Levothyroxine replacement therapy was started. Levothyroxine requirement was high but good substitution was achieved (TSH 0.53μU/ml) with 200μg/day (2.04μg/kg/day).
Eight months later, the patient was urgently referred from her General Practitioner to the Endocrinology Department due to symptoms of generalised oedema and laboratory findings of TSH 86.1μU/ml, FT4 0.9ng/dl and total cholesterol 399mg/dl (RR: 150–200). She was taking levothyroxine 225μg/day (2.25μg/kg/day) and she assured good compliance (no tablet omissions, taken on an empty stomach).
ManagementOn physical examination, there was certainly a generalised tension oedema in both lower extremities. The patient was moderately hypertensive (blood pressure 153/82mmHg). Cardiorespiratory status was good, without significant abnormalities in auscultation and with an oxygen saturation of 99%. Based on the significant oedema and severe hypercholesterolaemia, not justifiable due to the degree of hypothyroidism she showed, the possibility of nephrotic-range proteinuria was suspected. A semi-quantitative measurement of proteinuria with a dipstick was performed in a single urine sample and it showed proteinuria (+++). The patient was admitted to the Nephrology Department where a 24-h urine collection was performed, which showed a proteinuria of 6.58g/24h (RR: <0.15). The patient's glomerular filtration rate (GFR) was normal (creatinine 0.80mg/dl; creatinine clearance 97.1ml/min). Treatment with furosemide, ramipril, atorvastatin and aspirin was started. Levothyroxine was increased to 275μg/day (2.75μg/kg/day).
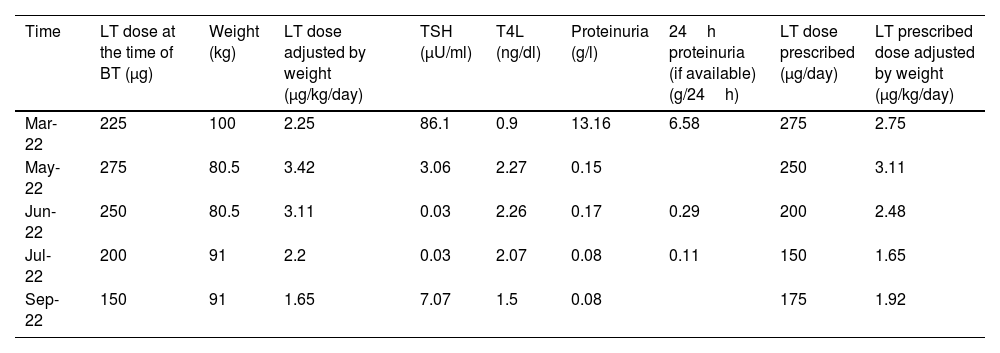
A kidney biopsy was carried out and it showed lupus nephritis (mesangial proliferative pattern). Treatment with prednisone, hydroxychloroquine, and mycophenolate mofetil was started. Under the described treatments, the patient showed a very significant improvement in the oedema and reduction of proteinuria which turned negative in a few weeks. Along with the reduction in oedema and proteinuria, a progressive reduction in levothyroxine requirement was observed. Changes in thyroid hormones, proteinuria, weight, and levothyroxine requirement are summarised in Table 1. Changes in proteinuria, TSH and FT4 are represented in Fig. 1.
Changes in thyroid hormones, proteinuria, weight, and levothyroxine requirement in a patient with post-surgical hypothyroidism and nephrotic syndrome due to lupus nephritis.
| Time | LT dose at the time of BT (μg) | Weight (kg) | LT dose adjusted by weight (μg/kg/day) | TSH (μU/ml) | T4L (ng/dl) | Proteinuria (g/l) | 24h proteinuria (if available) (g/24h) | LT dose prescribed (μg/day) | LT prescribed dose adjusted by weight (μg/kg/day) |
|---|---|---|---|---|---|---|---|---|---|
| Mar-22 | 225 | 100 | 2.25 | 86.1 | 0.9 | 13.16 | 6.58 | 275 | 2.75 |
| May-22 | 275 | 80.5 | 3.42 | 3.06 | 2.27 | 0.15 | 250 | 3.11 | |
| Jun-22 | 250 | 80.5 | 3.11 | 0.03 | 2.26 | 0.17 | 0.29 | 200 | 2.48 |
| Jul-22 | 200 | 91 | 2.2 | 0.03 | 2.07 | 0.08 | 0.11 | 150 | 1.65 |
| Sep-22 | 150 | 91 | 1.65 | 7.07 | 1.5 | 0.08 | 175 | 1.92 |
LT: levothyroxine; BT: blood test.

This case is a good illustration of the relationship that may exist between the presence of proteinuria and changes in thyroid hormones. Although an increase in levothyroxine requirement may have a multifactorial origin (increased body weight due to oedema, reduced absorption due to intestinal wall oedema) we think that a fundamental element was urinary loss of thyroid hormone binding proteins and, regarding this phenomenon, we decided to do a brief review of the scientific literature on this topic.
DiscussionRelationship between thyroid and kidney physiology is very important and increasingly well known. Normality of thyroid hormones is necessary for embryonic development of kidney and thyroid hormones influence the activity of many co-transporters of kidney tubules and regulate glomerular haemodynamics. Thus, it is well established that hypothyroidism leads to a decrease in GFR and an impaired ability to excrete free water. In contrast, hyperthyroidism implies an increase in GFR with decreased serum creatinine and a difficulty in concentrating urine.1
When glomerular damage occurs, involving a non-selective loss of serum proteins, it can include a significant loss of thyroid hormone binding proteins. Along with the loss of protein, huge amounts of thyroxine (T4) and triiodothyronine (T3) also leak from the body being able to generate de novo hypothyroidism or increase the requirement of levothyroxine in subjects with pre-existing hypothyroidism that is already being treated.1–5
The thyroid gland produces daily a mixture of T4 and T3, with a significant major proportion of the former. Mainly in the liver and kidney, type 1 iodothyronine deiodinase activates T4 via outer ring deiodination to obtain T3, which is the only one that can bind to the intranuclear thyroid hormone receptor. In many other tissues, such as the pituitary gland or brown adipose tissue, local transformation of T4 to T3 is also produced, catalysed by type 2 iodothyronine deiodinase. While circulating in the plasma, thyroid hormones are mainly transported bound to different proteins. The protein that transports the largest amounts of thyroid hormones is thyroxine-binding globulin (TBG), a protein of 54kDa mainly produced in the liver. The two other proteins with an important role in the transport of thyroid hormones are transthyretin (TTR or TBPA) and albumin. TTR, formerly known as prealbumin, is also mainly produced in the liver and has a molecular weight of 55kDa. Albumin is the most abundant protein in human plasma, has a molecular weight of 66.5kDa and, apart from very important transport functions, it is the major protein responsible for maintaining the oncotic pressure in body fluids.6–8
Nephrotic syndrome classically can occur when there is proteinuria greater than 3.5g/day, although minor losses (over 3g/day) can already initiate the process. Many diseases can cause the syndrome (diabetes mellitus, systemic lupus erythematosus, Sjögren syndrome, cryoglobulinemia, amyloidosis, solid or haematological malignancies, infections – syphilis, human immunodeficiency virus, hepatitis B and C). Damage or dysfunctions occur in the glomerulus components (basement membrane, endothelial surface, or epithelial cells – podocytes) that allow a massive leakage of proteins (mainly albumin) from plasma into urine. As a consequence of proteinuria, hypoalbuminemia develops, and it significantly reduces plasmatic oncotic pressure, generating oedema, which can lead to an anasarca condition. Other clinical manifestations of nephrotic syndrome are hypercoagulability and dyslipidaemia. The pathophysiology of these two phenomena is not yet well known. Urinary loss of antithrombotic proteins (protein S, antithrombin) and activators of lipoprotein lipase has been implicated.9
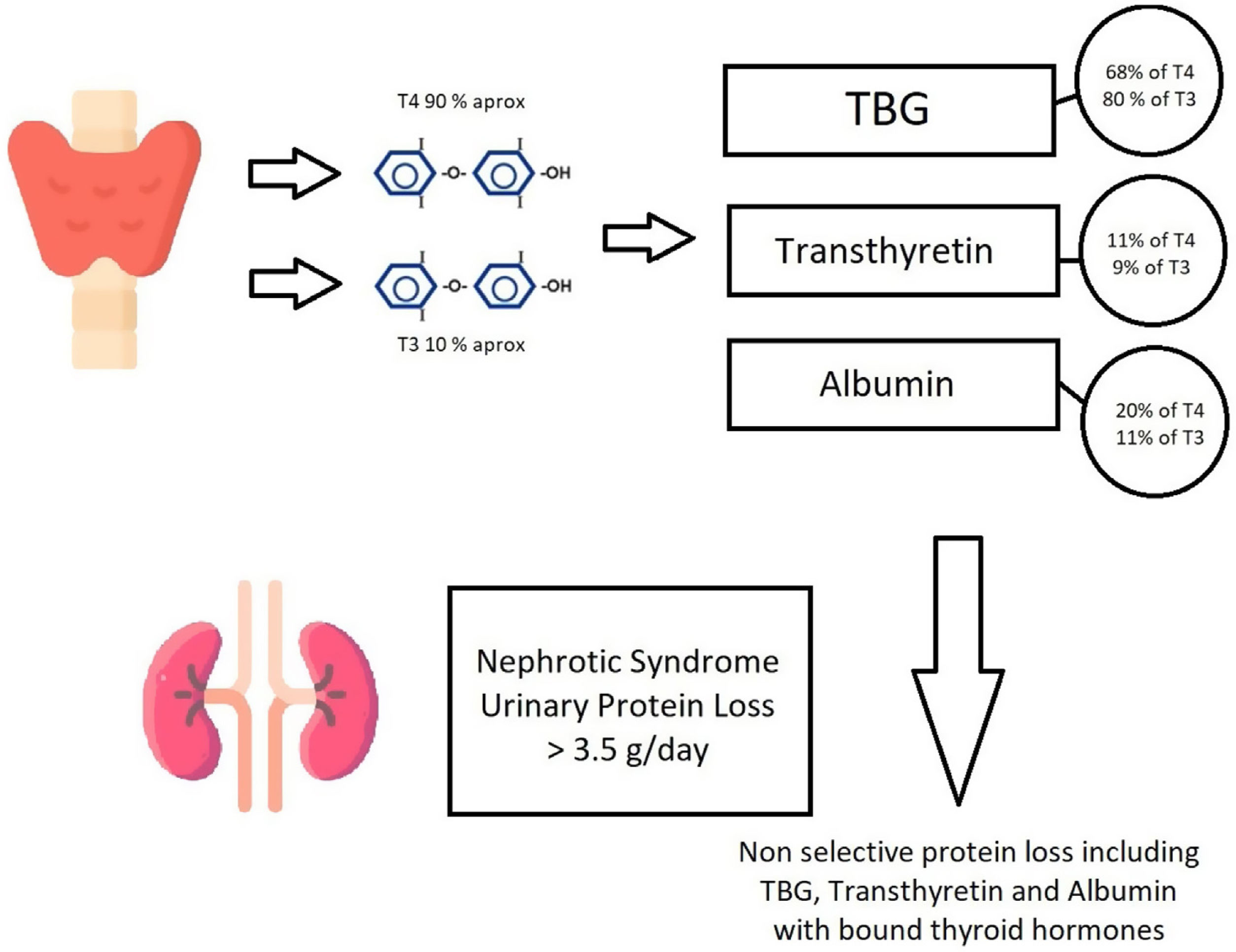
Urinary loss of thyroid hormone-binding proteins and thyroid hormones themselves, in patients with nephrotic-range proteinuria, has been well documented at least since the 1970s. Afrasiabi et al.10 demonstrated that in subjects with proteinuria>3g/day, the levels of total T4 in urine were 24.3μg/day compared with 1.5μg/day in healthy subjects. In parallel, urinary TBG levels in patients with nephrotic syndrome were 2.1mg/day while they were undetectable in subjects without disease. Gavin et al.11 found a positive correlation between the degree of proteinuria and daily urinary T4 loss (+0.53; p<0.001). Fig. 2 represents thyroid hormone production, linkage to binding proteins and loss of proteins when a nephrotic proteinuria occurs.

Thyroid hormones production, linkage to binding proteins and loss of proteins when a nephrotic proteinuria occurs. The binding percentages of hormones to carrier proteins are taken from Ref. 8. TBG: thyroxine-binding globulin.
In subjects with nephrotic syndrome and an intact thyroid gland, in most cases, thyroid hormone production will be increased to maintain proper function of the hormonal axis. However, in some patients, this adjustment will be insufficient and subclinical or primary hypothyroidism may be triggered. In children with idiopathic steroid-resistant nephrotic syndrome, Marimuthu et al.5 reported non autoimmune subclinical hypothyroidism in 8/30 patients and overt hypothyroidism in 2/30 patients. In adult patients, the de novo appearance of hypothyroidism in the context of nephrotic syndrome seems to be not so frequent, but there are also some case series reports.12,13
In patients with pre-existing hypothyroidism and treated with levothyroxine, the occurrence of nephrotic-range proteinuria causes, in most cases, an increase in hormone requirement and there are numerous reports of this phenomenon.2,14 In some of them, the diagnosis of proteinuria was delayed because symptoms such as oedema or dyslipidaemia are attributed to poorly substituted hypothyroidism, and levothyroxine malabsorption or non-compliance is suspected. The increase in the requirement of levothyroxine associated with proteinuria has been estimated at around 17%4 but higher increases in doses could be needed when severe proteinuria exists.
It should be taken into account that autoimmunity is a frequent cause of thyroid and kidney diseases and that both phenomena could coexist on many occasions (as in the case that we present). The relationship between lupus and thyroid autoimmunity is especially significant15 and antithyroid drug treatments have been associated with a greater risk of developing antibodies that cause vasculitis.16
It should also be noted that adjusting the treatment with levothyroxine, or starting it, when necessary, is of great importance, since thyroid hormones in their target tissues can positively contribute to the prognosis of kidney disease.17,18
Conclusions and recommendationsUrinary loss of thyroid hormones, fundamentally linked to their transport proteins, is a phenomenon that must be considered in patients with nephrotic-range proteinuria. In patients with prior hypothyroidism, it will increase levothyroxine requirement and in subjects without prior hypothyroidism it may trigger its occurrence.
Measurement of thyroid hormones should be recommended in patients with nephrotic syndrome, as well as assessing the presence of proteinuria in subjects affected by hypothyroidism who show increased levothyroxine requirement.
FundingThis article is a clinical case with a review of the literature. It has not had any specific funding.
Conflict of interestsThe authors declare that they have no conflict of interest.
