


The adequate measurement of height in subjects assessed for osteoporosis is of interest for the correct calculation of the body mass index (BMI), a recognized risk factor for osteoporotic fracture. The BMI is related to squared height, which means that small changes in height may have a significant effect on the BMI. Height loss over time results in a fictitious increase in the BMI.1
The effect of height as measured by a stadiometer, ulnar length, and arm span on the assessment of the risk of fragility fractures was assessed in a sample of patients with suspected osteoporosis referred from different care settings for a bone densitometry test by axial DXA at the Complejo Asistencial Universitario de León.2 The study sample consisted of subjects aged 40–90 years with no prior treatment with antiosteoporotic drugs. To estimate the 10-year risk of hip fracture and principal fracture, the application available at the FRAX® website for the British population (http://www.shef.ac.uk/FRAX/) was used in order that the intervention thresholds of the NOGG guidelines could be applied.3,4
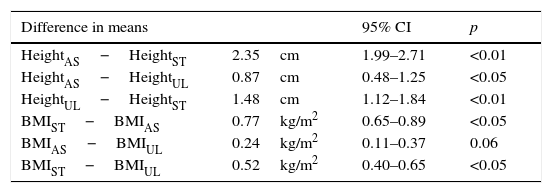
A total of 640 patients (95% females) with a median age of 59.4 years (IQR=14) and a mean BMI of 26.3kg/m2 (SD=4.2) were enrolled in the study. Height estimated from arm span was 2.35cm longer than height measured by a stadiometer (p<0.001). The BMI was greater when height measured by a stadiometer was used in calculation (p<0.001) (Table 1). Median risks of principal and hip fractures with the different height measurements showed no statistically significant differences, so that the use of different height measurement procedures resulted in no significant differences in the number of patients who required bone densitometry or who needed to be treated.
Comparison of heights estimated by stadiometer, arm span, and ulnar length and the BMI.
| Difference in means | 95% CI | p | |
|---|---|---|---|
| HeightAS−HeightST | 2.35cm | 1.99–2.71 | <0.01 |
| HeightAS−HeightUL | 0.87cm | 0.48–1.25 | <0.05 |
| HeightUL−HeightST | 1.48cm | 1.12–1.84 | <0.01 |
| BMIST−BMIAS | 0.77kg/m2 | 0.65–0.89 | <0.05 |
| BMIAS−BMIUL | 0.24kg/m2 | 0.11–0.37 | 0.06 |
| BMIST−BMIUL | 0.52kg/m2 | 0.40–0.65 | <0.05 |
CI: confidence interval; BMIUL: body mass index using HeightUL; BMIAS: body mass index using HeightAS; BMIST: body mass index using HeightST; HeightUL: height estimated by ulnar length; HeightAS: arm span as height; HeightST: height measured by stadiometer.
It is important when assessing a patient with osteoporosis to ascertain his/her maximum height achieved, because height loss results in a fictitious increase in the BMI and is considered to be an indirect sign of vertebral compression fractures.5 This data is often unavailable, but may be estimated from the arm span. Arm span does not change with age, and has therefore been suggested as an accurate indicator of the maximum height achieved.6 Unlike maximum height self-reported by the patient, arm span is obtained by objective measurement, provided the patient can stand and has no difficulty in extending both arms.
One of the limitations of arm span is that it should be measured in a precise, exact position. This is impossible when significant neuromuscular weakness, joint deformity, or abnormal muscle tone exists. Arm span measurement is inaccurate in these conditions. In addition, spinal deformities, such as kyphosis, make achieving an adequate position difficult, leading to wrong measurements. Ulnar length could be an alternative to arm span.2 The ulna is accessible, and its measurement points are easily identified even in people with severe disability and joint deformities. Ulnar measurement is reproducible and accurate, and provides a precise predictor of height.7 No significant differences were seen in our study between arm span and ulnar length, and both estimated a BMI lower than that calculated based on height.
In conclusion, the use of different methods to measure height in the FRAX® tool does not affect diagnostic and therapeutic decisions. Height measurement using ulnar length could be an alternative in cases where measurement might otherwise be impracticable, although additional studies are needed to verify this.
Conflicts of interestThe authors state that they have no conflicts of interest.
Please cite this article as: Kyriakos G, Vidal-Casariego A, Quiles-Sánchez LV, Calleja-Fernández A, Cano-Rodríguez I. La distancia cubital como una alternativa a la talla en el abordaje de la osteoporosis. Endocrinol Nutr. 2016;63:187–188.
