




We present the case of a 62-year-old Spanish man, with a history of high blood pressure, dyslipidaemia, obesity and prediabetes mellitus. He was a former smoker of 45 pack-years. A farmer by profession.
He presented with general malaise, fever and an erythematous reaction on the left side of the face, radiating to the upper left thoracic area. He was prescribed doxycycline 100 mg/12 h and streptomycin 1 g/24 h, but with no improvement.
Given his worsening condition, he went to his health service to be re-assessed. He had an erythematous rash covering his body with extension towards the scalp, and left perichondral involvement with purulent content coming out of his ear canal. In addition to these regions, enlargement of his laterocervical, preauricular and retroauricular lymph node chains was detected. Notably, there were multiple erosions in his ear canal. His vital signs were as follows: temperature (T) 37.2°C; blood pressure (BP) 168/94 mmHg; heart rate (HR) 84 bpm; oxygen saturation (SatO2) 92%.
Blood tests showed a high C-reactive protein (289.80 mg/l, reference range 0−15 mg/l) with leucocytosis (18.63 × 1,000/μl, reference range 4 × 1,000–10 × 1,000/μl) and neutrophilia (15.69 × 1,000/μl, reference range 2 × 1,000–7.5 × 1,000/μl). The rest of the tests performed were within normal limits, including a chest x-ray.
The patient was admitted to the Infectious Diseases Unit. After an initial assessment, the symptoms were confirmed and it was decided to obtain two samples of the purulent content of the left ear canal, and initial treatment was proposed based on intravenous (IV) piperacillin – tazobactam 4 g–0.5 g/8 h plus linezolid 600 mg/12 h, replacing the previous regimen. After this, an Ear, Nose and Throat (ENT) assessment was requested and investigations were completed with a computed tomography (CT) scan of the facio-cervical structures to detect possible abscesses, collections or erosions of the surrounding bone material which could cause local fistulisation.
The ENT assessment and CT images ruled out the presence of local complications. It was also decided to expand the treatment with ciprofloxacin ear drops at 3 mg/6 drops/12 h.
During his hospital stay, the patient's condition improved, with a progressive reduction of the erythema on his body, and confirmed by an improvement in his analytical markers with C-reactive protein (150.10 mg/l), leucocytosis (11.83 × 1,000/μl) and neutrophilia (8.10 × 1,000/μl).
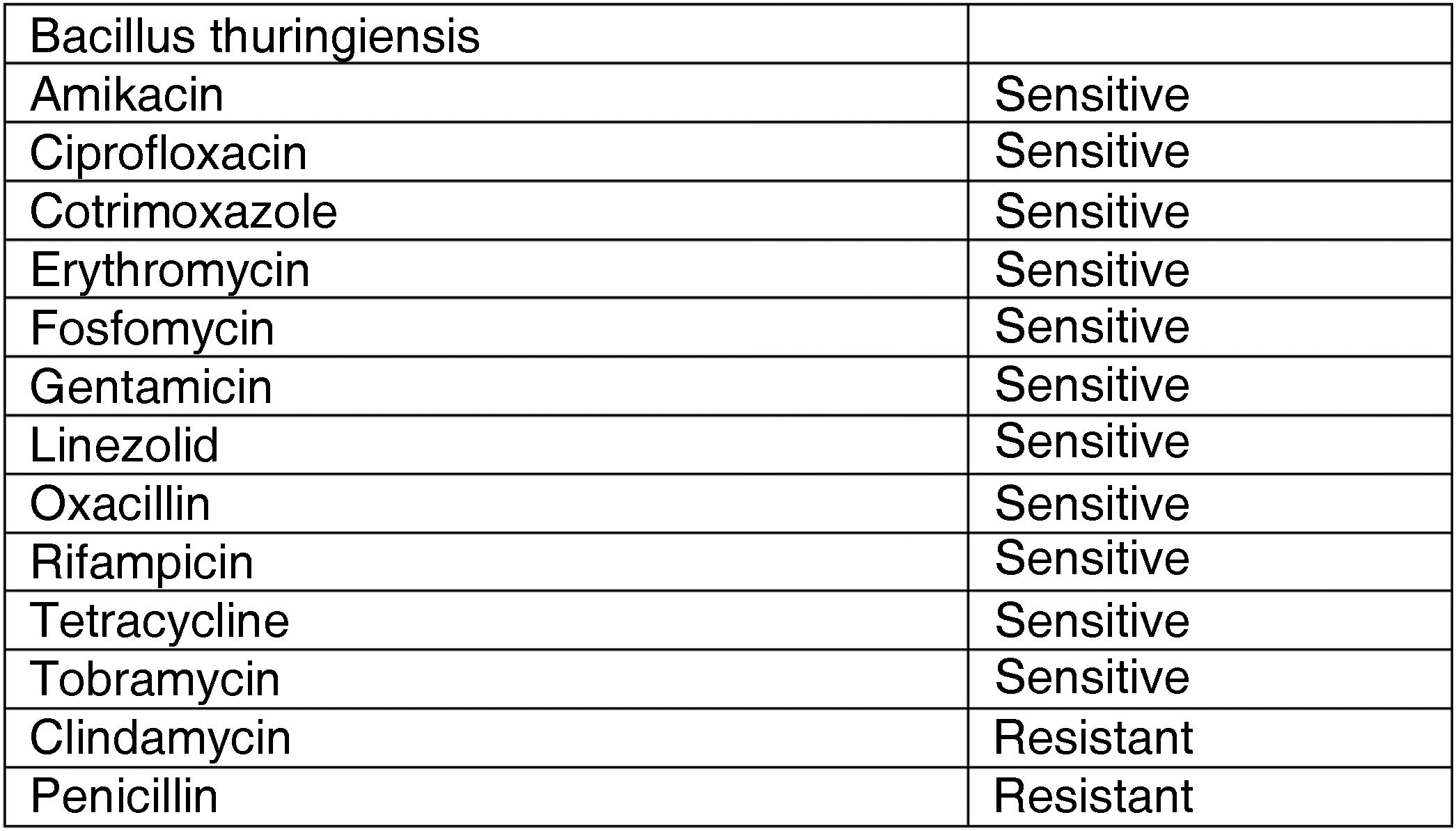
In addition to this, the results of the bacteriological cultures of the ear canal showed the presence of Bacillus thuringiensis, sensitive to the treatments given (Fig. 1).

Given his good clinical progress, with virtual resolution of his analytical parameters, with C-reactive protein (10.30 mg/l), leucocytosis (11.03 × 1,000/μl) and neutrophilia (6.88 × 1,000/μl), the patient was sent home on ciprofloxacin 500 mg/12 h and linezolid 600 mg/12 h, with subsequent follow-up at the Infectious Diseases Unit clinic.
The condition was classified as craniofacial cellulitis with perichondritis, external otitis and erythematous irradiation towards cervical/thoracic regions. The pathogen isolated was B. thuringiensis, an unusual germ as a skin isolate, but related to the patient's agricultural work.
B. thuringiensis is the most used biological insecticide worldwide. The pesticidal mechanism of this gram-positive bacteria1 is based on the production of crystalline protein bodies, which are toxic to different invertebrates, especially their larvae.2,3 These proteins are called Cry. The crystals of B. thuringiensis are ingested and solubilised in the insect's digestive system, after which the crystalline proteins are released in the form of protoxins, which are processed by intestinal proteases to form active larvicidal proteins. This process consists of a cadherin-mediated reaction and its subsequent induction fed back by a magnesium-mediated cascade, which is ultimately responsible for the cell lysis in the ingestor.4,5
Most natural insecticides contain spores and crystals from the pathogen, obtained through gene transfer, but third-generation bioinsecticides contain the bacteria themselves genetically modified to enhance their virulence.
The toxic effect on humans is almost non-existent. The skin and eye regions are the most affected, if such an effect occurs, in the form of erythema and local irritation. An increased toxic risk is to be expected in patients suffering from immunosuppressive states, diabetes mellitus or lack of skin turgor.
FundingNo funding was received for this study.
Conflicts of interestThe authors declare that they have no conflicts of interest.
