




Management of osteoporotic fractures becomes challenging because of its multiple associated factors as well as poor bone quality. Therefore, assessments of the risk factors of osteoporotic fractures among low impact trauma client is a matter of great concern which can be addressed properly to reduce their occurrence in future.
MethodThirty patients with single or multiple fractures were selected purposively for descriptive survey study between January 2018 to December 2018. Their ages varied from 41 to 80 years. There were 26 female and four males. 24 patients have single fracture and six had multiple fractures following low impact trauma. The demographic parameters were studied by structured interview schedule, and the research variable, the risk factors were studied by interview, biophysical assessment and records of BMD value through DEXA and serum level of vitamin D. Socio-demographic variables like age, sex, body weight, Body mass index (BMI), etc. were selected and their relationship were assessed to find out the risk factors of fragility fractures in society by research variables like risk factors of osteoporotic fractures. For statistical analysis of determination of association between such factors and fragility fractures, non-parametric Fisher exact test and Odds ratio was used.
ResultsIn our study, osteoporotic fractures occurred majority (86.66%) among female maximally among 60–69 years age group. Whereas in relatively younger age (40–60 years), abnormal BMI (low or high) is responsible for fragility fracture as 46.6% of such fractures occurred in this group as 20% fracture are associated with underweight and 40.66% with overweight BMI. Tobacco smoking increases the risk of fragility fractures twice (as relative risk ratio 2) and rheumatoid arthritis increases the six-fold (as relative risk ratio 6). All 100% had history of fall. Level of serum vitamin D, low DEXA scan value (less than −2.5) and fall on ground resulting in low impact injuries shows strong association between those and fragility fractures. On the other hand, all the risk factors remain same for the recent and old fractures.
ConclusionSeveral risk factors need to be addressed properly apart from medical managements to reduce the risk of occurrence of osteoporotic fractures.
Any fracture when present with diagnosed osteoporosis (fragility fracture) pose a challenging problem because osteoporosis is a multifactorial disease, commonly associated with several co-morbidities with compromised functions of multiple systems.
Moreover over 50 years of age one in three women and one in five male experience fragility fracture.1–4 Such fracture commonly occurs in dorsa lumber vertebra and among non-vertebral fractures affecting distal radius, neck of femur, proximal humours, etc. As per study of western society, there are multiple factors commonly associated with such fractures like elderly age, female, co-existing disease, and intake of glucocorticoid as well as fall on ground resulting from trivial trauma.5 But there is no adequate published study with Indian population for finding out the risk factors associated with osteoporosis.6 Therefore, we attempted to find out such factors among Indian population which may be properly addressed for reduction of occurrence of such fractures in the Indian society.
MethodThirty patients with their ages varied from 41 to 80 (mean age 59) years were selected by non-probable purposive method using specific criteria for descriptive survey design study presented in orthopaedic outpatient department of IPGME&R, SSKM medical college from January 2018 to December 2018. The inclusion criteria were single or multiple fractures following low impact trauma in the age group 40–90 years. The high impact trauma and any fractures beyond the above age range were excluded. Sample size was calculated by using formula of descriptive study design by Master 2.0 (Dept of Biostatistics, CMC Vellore, India 2011). Socio-demographic variables like age, sex, body weight, Body Mass Index (BMI), etc. were selected and their relationship were assessed to find out the risk factors of fragility fractures in society by research variables like risk factors of osteoporotic fractures. Socio-demographic variables like, age, sex of the patients, number of fragility fractures, their site, habit of smoking, alcohol intake more than 3 peg per day, associated co-morbid disease, like, rheumatoid arthritis, visual, auditory, depth of perception impairment, hypertension, intake of glucocorticoid, history of tendency to fall were encountered by tool of structured interview schedule which was properly validated by nine different experts, not involved with this study. The research variable of our study (risk factors of osteoporotic fractures) was assessed by three tools by interviewing with structured interview schedule, bio-physical assessment by physical examination formula, weight machine, tape measure, and analysis of record of bone mineral density (BMD) level using dual energy X-ray absorptiometry (DEXA) and serum vitamin D3 label. For statistical analysis of determination of association between such factors and fragility fractures, non-parametric Fisher exact test and Odds ratio was used.
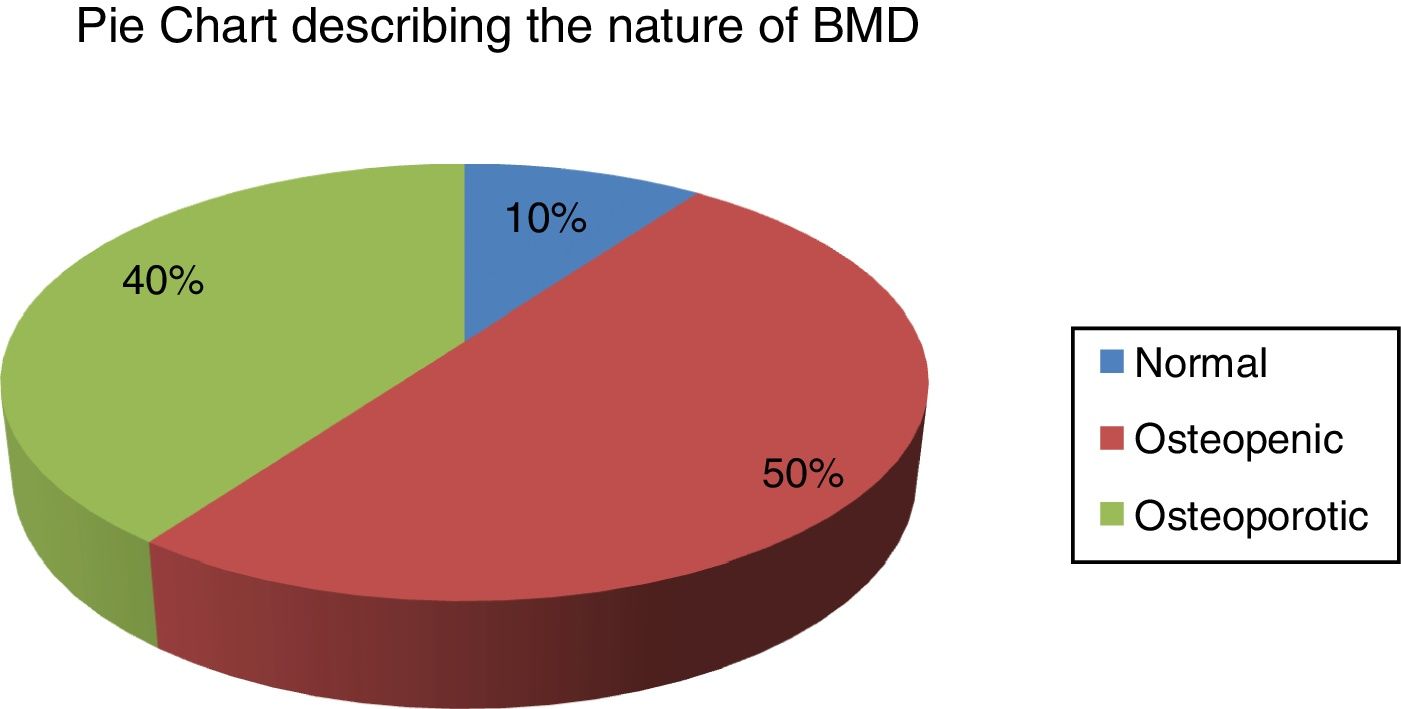
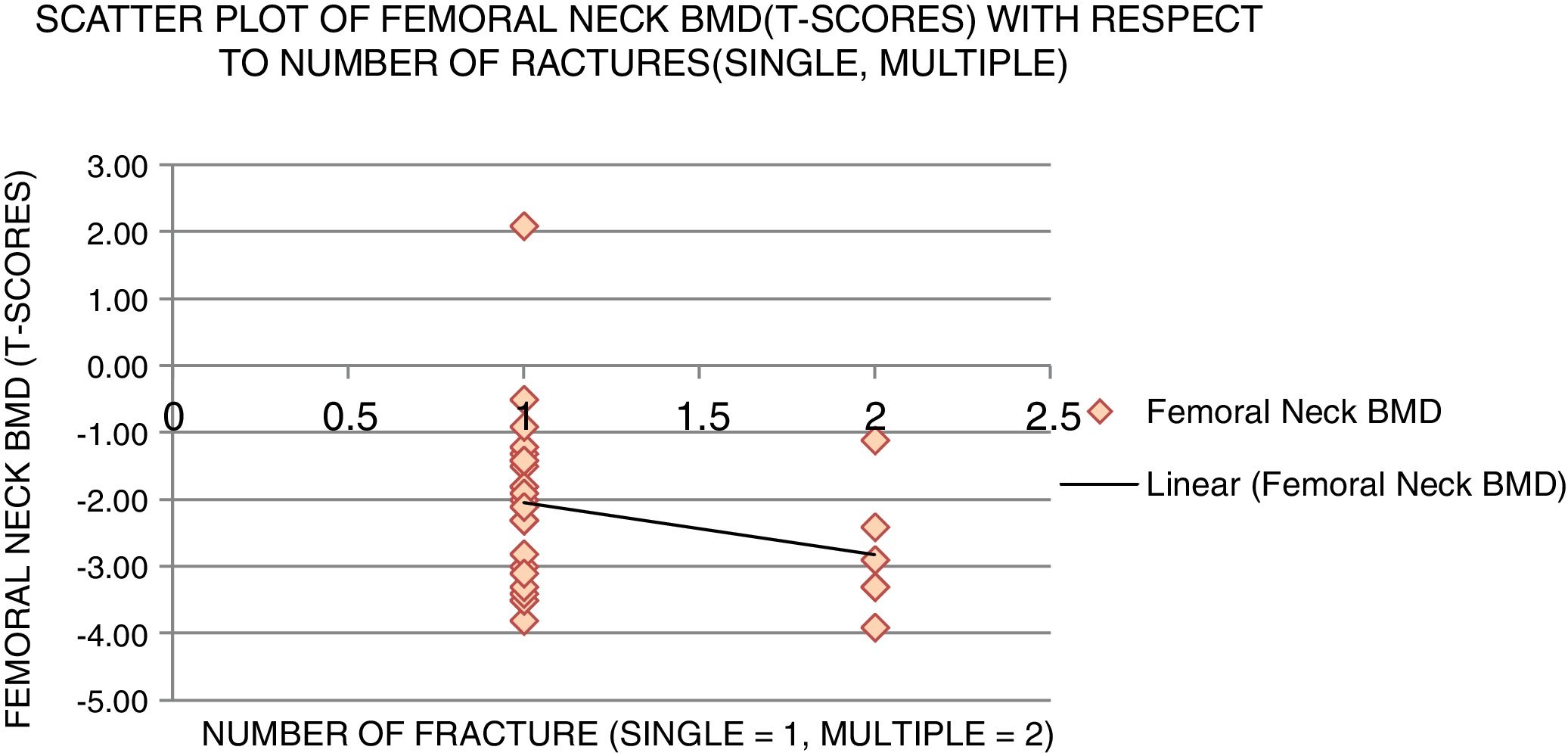
ResultsIn the study, we observed fragility fractures occurred majority among female (87%) as seen in Table 1. Majority of fragility fracture (43.33%) seen between (60–69) years age group. Abnormal BMI was responsible for majority (66.6%) of fragility fracture irrespective of age and sex, of which 20% (6 patients) fractures were associated with low BMI and 40.6% with high BMI (overweight in 12 patients and two among obese). Following BMD study 50% fragility fractures showed osteopenia (DEXA scan between −1 to −2.4), 40% osteoporotic (DEXA scan less than −2.5) and 10% normal (Fig. 1). Only moderate positive correlation (Co-efficient of correlation 0.4) was found between femoral neck BMD and BMI. On the other hand, point biserial coefficient between femoral neck BMD and number of fractures was found to be −0.25 which indicated weak negative correlation (Fig. 2). Multiple fractures occurred in six patients which did not associated with advanced age, but relative risk ratio of intake of tobacco, alcohol was 2 and co-morbid disease like rheumatoid arthritis was 6 as presence of rheumatoid arthritis was associated with 50% multiple fractures in contrast to <20% single fractures. Single fracture patients exposed to tobacco/smoking habits were twice at risk of getting multiple fractures as compared to single fracture patients not exposed to tobacco/smoking habits.
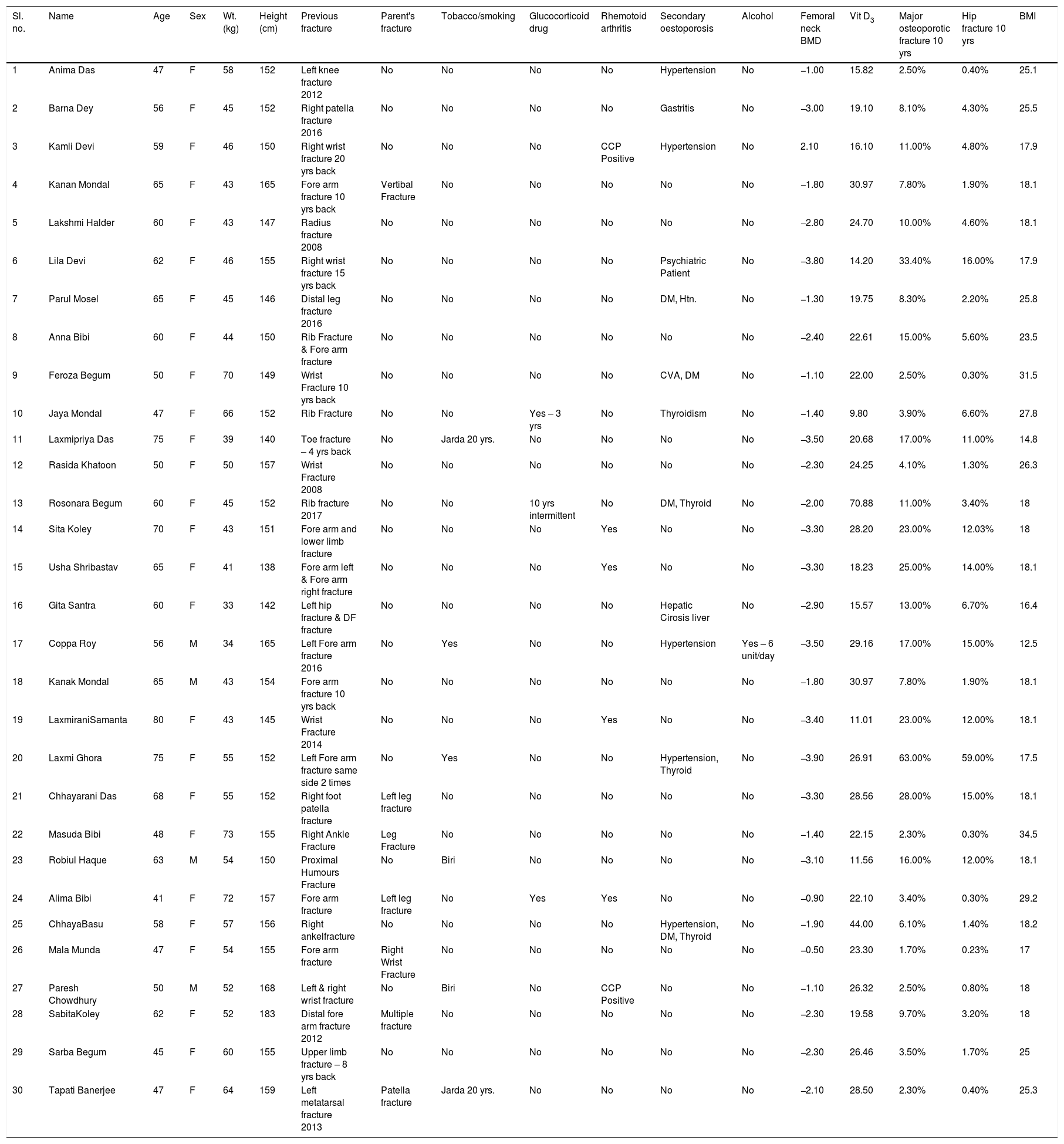
Showing all information of all 30 patients.
| Sl. no. | Name | Age | Sex | Wt. (kg) | Height (cm) | Previous fracture | Parent's fracture | Tobacco/smoking | Glucocorticoid drug | Rhemotoid arthritis | Secondary oestoporosis | Alcohol | Femoral neck BMD | Vit D3 | Major osteoporotic fracture 10 yrs | Hip fracture 10 yrs | BMI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Anima Das | 47 | F | 58 | 152 | Left knee fracture 2012 | No | No | No | No | Hypertension | No | −1.00 | 15.82 | 2.50% | 0.40% | 25.1 |
| 2 | Barna Dey | 56 | F | 45 | 152 | Right patella fracture 2016 | No | No | No | No | Gastritis | No | −3.00 | 19.10 | 8.10% | 4.30% | 25.5 |
| 3 | Kamli Devi | 59 | F | 46 | 150 | Right wrist fracture 20 yrs back | No | No | No | CCP Positive | Hypertension | No | 2.10 | 16.10 | 11.00% | 4.80% | 17.9 |
| 4 | Kanan Mondal | 65 | F | 43 | 165 | Fore arm fracture 10 yrs back | Vertibal Fracture | No | No | No | No | No | −1.80 | 30.97 | 7.80% | 1.90% | 18.1 |
| 5 | Lakshmi Halder | 60 | F | 43 | 147 | Radius fracture 2008 | No | No | No | No | No | No | −2.80 | 24.70 | 10.00% | 4.60% | 18.1 |
| 6 | Lila Devi | 62 | F | 46 | 155 | Right wrist fracture 15 yrs back | No | No | No | No | Psychiatric Patient | No | −3.80 | 14.20 | 33.40% | 16.00% | 17.9 |
| 7 | Parul Mosel | 65 | F | 45 | 146 | Distal leg fracture 2016 | No | No | No | No | DM, Htn. | No | −1.30 | 19.75 | 8.30% | 2.20% | 25.8 |
| 8 | Anna Bibi | 60 | F | 44 | 150 | Rib Fracture & Fore arm fracture | No | No | No | No | No | No | −2.40 | 22.61 | 15.00% | 5.60% | 23.5 |
| 9 | Feroza Begum | 50 | F | 70 | 149 | Wrist Fracture 10 yrs back | No | No | No | No | CVA, DM | No | −1.10 | 22.00 | 2.50% | 0.30% | 31.5 |
| 10 | Jaya Mondal | 47 | F | 66 | 152 | Rib Fracture | No | No | Yes – 3 yrs | No | Thyroidism | No | −1.40 | 9.80 | 3.90% | 6.60% | 27.8 |
| 11 | Laxmipriya Das | 75 | F | 39 | 140 | Toe fracture – 4 yrs back | No | Jarda 20 yrs. | No | No | No | No | −3.50 | 20.68 | 17.00% | 11.00% | 14.8 |
| 12 | Rasida Khatoon | 50 | F | 50 | 157 | Wrist Fracture 2008 | No | No | No | No | No | No | −2.30 | 24.25 | 4.10% | 1.30% | 26.3 |
| 13 | Rosonara Begum | 60 | F | 45 | 152 | Rib fracture 2017 | No | No | 10 yrs intermittent | No | DM, Thyroid | No | −2.00 | 70.88 | 11.00% | 3.40% | 18 |
| 14 | Sita Koley | 70 | F | 43 | 151 | Fore arm and lower limb fracture | No | No | No | Yes | No | No | −3.30 | 28.20 | 23.00% | 12.03% | 18 |
| 15 | Usha Shribastav | 65 | F | 41 | 138 | Fore arm left & Fore arm right fracture | No | No | No | Yes | No | No | −3.30 | 18.23 | 25.00% | 14.00% | 18.1 |
| 16 | Gita Santra | 60 | F | 33 | 142 | Left hip fracture & DF fracture | No | No | No | No | Hepatic Cirosis liver | No | −2.90 | 15.57 | 13.00% | 6.70% | 16.4 |
| 17 | Coppa Roy | 56 | M | 34 | 165 | Left Fore arm fracture 2016 | No | Yes | No | No | Hypertension | Yes – 6 unit/day | −3.50 | 29.16 | 17.00% | 15.00% | 12.5 |
| 18 | Kanak Mondal | 65 | M | 43 | 154 | Fore arm fracture 10 yrs back | No | No | No | No | No | No | −1.80 | 30.97 | 7.80% | 1.90% | 18.1 |
| 19 | LaxmiraniSamanta | 80 | F | 43 | 145 | Wrist Fracture 2014 | No | No | No | Yes | No | No | −3.40 | 11.01 | 23.00% | 12.00% | 18.1 |
| 20 | Laxmi Ghora | 75 | F | 55 | 152 | Left Fore arm fracture same side 2 times | No | Yes | No | No | Hypertension, Thyroid | No | −3.90 | 26.91 | 63.00% | 59.00% | 17.5 |
| 21 | Chhayarani Das | 68 | F | 55 | 152 | Right foot patella fracture | Left leg fracture | No | No | No | No | No | −3.30 | 28.56 | 28.00% | 15.00% | 18.1 |
| 22 | Masuda Bibi | 48 | F | 73 | 155 | Right Ankle Fracture | Leg Fracture | No | No | No | No | No | −1.40 | 22.15 | 2.30% | 0.30% | 34.5 |
| 23 | Robiul Haque | 63 | M | 54 | 150 | Proximal Humours Fracture | No | Biri | No | No | No | No | −3.10 | 11.56 | 16.00% | 12.00% | 18.1 |
| 24 | Alima Bibi | 41 | F | 72 | 157 | Fore arm fracture | Left leg fracture | No | Yes | Yes | No | No | −0.90 | 22.10 | 3.40% | 0.30% | 29.2 |
| 25 | ChhayaBasu | 58 | F | 57 | 156 | Right ankelfracture | No | No | No | No | Hypertension, DM, Thyroid | No | −1.90 | 44.00 | 6.10% | 1.40% | 18.2 |
| 26 | Mala Munda | 47 | F | 54 | 155 | Fore arm fracture | Right Wrist Fracture | No | No | No | No | No | −0.50 | 23.30 | 1.70% | 0.23% | 17 |
| 27 | Paresh Chowdhury | 50 | M | 52 | 168 | Left & right wrist fracture | No | Biri | No | CCP Positive | No | No | −1.10 | 26.32 | 2.50% | 0.80% | 18 |
| 28 | SabitaKoley | 62 | F | 52 | 183 | Distal fore arm fracture 2012 | Multiple fracture | No | No | No | No | No | −2.30 | 19.58 | 9.70% | 3.20% | 18 |
| 29 | Sarba Begum | 45 | F | 60 | 155 | Upper limb fracture – 8 yrs back | No | No | No | No | No | No | −2.30 | 26.46 | 3.50% | 1.70% | 25 |
| 30 | Tapati Banerjee | 47 | F | 64 | 159 | Left metatarsal fracture 2013 | Patella fracture | Jarda 20 yrs. | No | No | No | No | −2.10 | 28.50 | 2.30% | 0.40% | 25.3 |

 is a dichotomous variable. Hence, point biserial correlation coefficient was computed and found to be −0.25.")
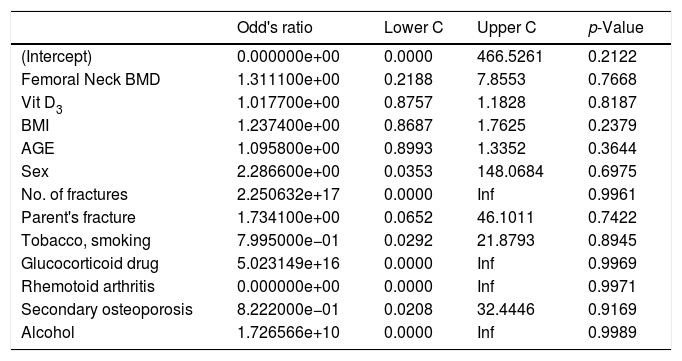
Thirteen patients (43.3%) had associated single or multiple co-morbidities of which cardiovascular disease was maximally associated in six (20%) patients. However, all the risk factors remain same for recent or old fracture using the Odds ratio (Table 2). The Fisher's exact test at 2df was used to see the association bet single/multiple fragility fracture and BMD through DEXA scan which shows calculated value 0.00003 which is significant (p<0.05) suggesting significant association between osteoporosis and association of fragility fractures. Similarly, Fisher exact test at 1df association was estimated between single/multiple fragility fracture and value of serum vitamin D which showed calculated value 0.000054 (p<0.05) suggesting strong association between them. All patients had history of trivial trauma or low impact injury following fall on ground.
Exploring the relationship of the risk factors with respect to the recent and old fragility fracture.
| Odd's ratio | Lower C | Upper C | p-Value | |
|---|---|---|---|---|
| (Intercept) | 0.000000e+00 | 0.0000 | 466.5261 | 0.2122 |
| Femoral Neck BMD | 1.311100e+00 | 0.2188 | 7.8553 | 0.7668 |
| Vit D3 | 1.017700e+00 | 0.8757 | 1.1828 | 0.8187 |
| BMI | 1.237400e+00 | 0.8687 | 1.7625 | 0.2379 |
| AGE | 1.095800e+00 | 0.8993 | 1.3352 | 0.3644 |
| Sex | 2.286600e+00 | 0.0353 | 148.0684 | 0.6975 |
| No. of fractures | 2.250632e+17 | 0.0000 | Inf | 0.9961 |
| Parent's fracture | 1.734100e+00 | 0.0652 | 46.1011 | 0.7422 |
| Tobacco, smoking | 7.995000e−01 | 0.0292 | 21.8793 | 0.8945 |
| Glucocorticoid drug | 5.023149e+16 | 0.0000 | Inf | 0.9969 |
| Rhemotoid arthritis | 0.000000e+00 | 0.0000 | Inf | 0.9971 |
| Secondary osteoporosis | 8.222000e−01 | 0.0208 | 32.4446 | 0.9169 |
| Alcohol | 1.726566e+10 | 0.0000 | Inf | 0.9989 |
Response: Period of fracture (recent/past).
Risk factors: Sex, number of fractures, Parent's fracture, Tobacco, Smoking, Alcohol, Glucocorticoid drug, Rheumatoid arthritis, Secondary osteoporosis, Femoral neck BMD, Vit D3, BMI, AGE.
Method for assessing the risk factors: fit logistic regression model of response on categorical risk factors.
Predictors Summary Obtained multivariate OR (95% CI) for all predictors of the fitted model.
Comment: the odds of the recent fractures to the odds of past fractures, based on the risk factors or predictors are not significant at 0.05 level of significance as p-value >0.05.
Osteoporosis appears to be a silent epidemic worldwide and its burden is increasing exponentially in daily life. Unfortunately, it remains relatively silent till fracture occurs. Therefore, early diagnosis of osteoporosis and their associated risk factors are of great concern and carries immense importance for reduction of such devastating consequences in the society. This study among Indian population showed valuable demographic association. Elderly female remains the constant victim of fragility fracture. Six decade of life remain the common age group irrespective of sex having fragility fracture most probably due to withdrawal of sex hormone in both sexes in that age with maintenance of outdoor activity without adequate physical fitness resulting in trivial trauma in presence of co-morbidities. Whereas in relatively younger age (40–60 years), abnormal BMI (low or high) is responsible for fragility fracture as 46.6% of such fractures occurred in this group. This reiterate the fact that abnormal BMI (low or high) can be responsible for fragility fracture irrespective of age and sex.
As per estimation of DEXA scan value, only 40% patients have osteoporosis (DEXA T score less than −2.5). The Fisher exact test value suggests strong association between osteoporosis DEXA value and fragility fracture, but weak negative correlation between number of fractures and BMD indicate the patient with lower BMD is more prone to develop multiple fragility fracture. Tobacco smoking increases the risk of fragility fractures twice (as relative risk ratio 2). Though among the associated co-morbidities, cardiovascular problems are commonest, but the presence of rheumatoid arthritis increases the six-fold (as relative risk ratio 6) risk of getting multiple fracture compared to single fracture not having rheumatoid arthritis. Only level of serum vitamin D3 and fall on ground resulting in low impact injuries shows strong association between those and fragility fractures. On the other hand, all the risk factors remain same for the recent and old fractures (Table 2), suggesting all the risk factors will have to take into account equally for patients with past history of fragility fractures and also those with recently developed fractures to reduce the risk of developing further fragility fractures in same individual in future. However, we have to give special emphasis on those factors which can cause multiple fragility factors like low DEXA scan, low vitamin D, rheumatoid arthritis and history or tendency to fall. Though small sample size remains the limitation of our study, but pointing out of factors strongly associated with fragility factors remained our strength which will require further study among large population to formulate a comprehensive management protocol addressing those responsible factors to reduce the risk of dreaded fragility fracture in the society.
Therefore, elderly female of which age, abnormal BMI and smoking carries mild correlation, low DEXA moderate and fall on ground, low vitamin D3, rheumatoid arthritis carries strong correlation of occurrence of multiple fragility fractures or recent/new fragility fracture in spite of having past history of such fracture. All the risk factors will have to take into account with formulation of comprehensive treatment protocol for reduction of risk of fragility fractures in Indian society.
FundingNone.
Conflict of interestsThe authors declare no conflict of interest.
MSVP of IPGMER, SSKM Medical College & Hospital.
Peer-review under responsibility of the scientific committee of the 3rd International Conference on Healthcare and Allied Sciences (2019). Full-text and the content of it is under responsibility of authors of the article.
