





To analyse the psychometric properties of the Parents’ Perception of Uncertainty in Illness Scale, parents/children, adapted to Spanish.
MethodA descriptive methodological study involving the translation into Spanish of the Parents’ Perception of Uncertainty in Illness Scale, parents/children, and analysis of their face validity, content validity, construct validity and internal consistency.
ResultsThe original version of the scale in English was translated into Spanish, and approved by its author. Six face validity items with comprehension difficulty were reported; which were reviewed and adapted, keeping its structure. The global content validity index with expert appraisal was 0.94. In the exploratory analysis of factors, 3 dimensions were identified: ambiguity and lack of information, unpredictability and lack of clarity, with a KMO=0.846, which accumulated 91.5% of the explained variance. The internal consistency of the scale yielded a Cronbach alpha of 0.86 demonstrating a good level of correlation between items.
ConclusionThe Spanish version of “Parent's Perception of Uncertainty in Illness Scale” is a valid and reliable tool that can be used to determine the level of uncertainty of parents facing the illness of their children.
Analizar las propiedades psicométricas de la Escala de Percepción de la Incertidumbre en la Enfermedad-forma padres/hijos, adaptada al español.
MétodoEstudio descriptivo, metodológico que incluyó la traducción al español de la Escala de Percepción de la Incertidumbre en la Enfermedad-forma padres/hijos y el análisis de su validez facial, validez de contenido, exploración de la validez de los constructos y la consistencia interna.
ResultadosLa versión original de la escala en inglés se tradujo al español, siendo aprobada por la autora del mismo. La validación facial reportó 6 ítems con dificultad de comprensión que fueron revisados y adaptados, manteniendo la estructura. El índice de validez de contenido global con apoyo de expertos fue de 0,94. En el análisis exploratorio de factores se identificaron 3 dimensiones: ambigüedad y falta de información, imprevisibilidad y falta de claridad, con un KMO=0,846 que acumularon el 91,5% de la varianza explicada. La consistencia interna total de la escala arrojó un alfa de Cronbach de 0,86 lo que demostró un buen nivel de correlación entre los ítems.
ConclusiónLa Escala de Percepción de la Incertidumbre en la Enfermedad–forma padres/hijos adaptada al español de manera exploratoria muestra ser una herramienta válida y confiable que puede ser utilizada para determinar el nivel de incertidumbre de los padres frente a la enfermedad de sus hijos.
The Parent's Perception Uncertainty in Illness Scale (PPUS) measures the uncertainty of parents with acutely and chronically ill and/or hospitalised children. Its original version in English was designed by Mishel (1983), and has proven to have good validity and reliability indices. It has been widely used with parents of critically ill hospitalised children, preterm babies, children with leukaemia, children with cystic fibrosis and children with diverse chronic illnesses.
Since there is no existing version in Spanish we are providing this version with good indicators of face validity, content and reliability, consistent with the original English version. Regarding the result of construct validity, a proposal for factorial structure is provided but requires further exploratory analysis and subsequently confirmatory analysis to help corroborate the proposed factorial structure. This is a major tool for medical practice and for future investigations wishing to assess the uncertainly level and generate strategies for to modulate it.
Implications of the studyIn clinical practice and care management this version of the scale will promote the measurement of uncertainty in parents with ill children as a basis for the generation of interdisciplinary intervention strategies to modulate the levels of uncertainty directly or indirectly and to strengthen institutional policies that provide clear proof of the humanisation of care as a key to quality. For research purposes, the Spanish version will help to measure this construct in Spanish texts prior to transcultural validation. It will also support the development of quantitative studies which include the uncertainly of parents as a variable. In teaching it will support the process of training of pre- and post graduate students aiding comprehension of phenomena relating to health from the use of objective tools.
Illness and hospitalisation affect children and families. They are events which trigger different emotional responses that make it difficult for parents to adapt because they compromise the the child. During the hospitalisation experience, whether this be in the paediatric, intensive care or critical care departments, several factors such as difficulty in communicating with the child, the change in parents’ role, limitations for accompanying the child, lack of familiarity with the technical environment, an existing weak social support, concern for the child's health status, lack of information on prognosis and treatment, the subjection of the child to painful medical procedures, restriction of timetables and visits, and lack of health staff time, all complicate this situation for both parents and child making it difficult to interpret and handle.1–5
One of the emotional responses which parents experience in this situation is uncertainty. This was defined by Mishel as the inability to determine the significance of events relating to the illness. It is also a cognitive state created when the individual is unable to structure or classify the events relating to the illness and treatment which occurs in ambiguous, complex, unpredictable situations or when there is no information available or it is inconsistent.6 It becomes a negative experience associated with emotional anguish and with poor psychosocial adjustment for the patients and their family members.7 Mishel suggests that uncertainty in general and the uncertainty that parents of ill and/or hospitalised children share 4 dimensions: ambiguity with regard to the illness; unpredictability for the course and prognosis of each individual; lack of information regarding the illness, treatment and health system and complexity or lack of clarity of the information.6
Stewart and Mishel8 conducted a state of the art study of the parents of ill children, finding that uncertainty was influenced by the characteristics of the person, the illness and the environment. The parents of the youngest, smallest children presented with higher levels of uncertainty and it has been reported that the diagnosis stae is considered the one when greatest uncertainty is felt. Likewise, the care environment of the child, and particularly the novelty and confusion of the initial phase of the illness, is also related to uncertainty. Despite the importance of research findings reported, little has been studied on the interactions between parental uncertainty and the uncertainty of the child or the effects of this uncertainty on the child itself, when it is ill. However, it is known that changes in the level of uncertainty of the parents affects the child's health status.8,9
To respond to the needs of parents’ suffering from uncertainty and thereby foster the care context of the children, the healthcare team should assess and create strategies to keep them informed, facilitate interaction with their children and prepare for the child's discharge from hospital so as to reduce negative feelings the illness may cause and aid adaptation to the hospital environment.8,10–12 The background, consequences and challenges relating to the uncertainty parents feel need to be identified so as to incorporate comprehensive intervention strategies that foster processes of recovery of the family nucleus. To do so requires valid and reliable assessment tools.7,8,13
Mishel designed a battery of instruments for measuring uncertainty: in ill and hospitalised adults (MUIS-A), in individuals or family members of people with chronic illness who are not hospitalised and who are not receiving medical intervention (MUIS-C) and in the spouses or family members of ill people (MUIS-FC). The different forms of these scales have been widely used in people with different acute and chronic illnesses such as cancer, HIV, lung and heart diseases, congenital diseases, and surgical procedures. They have been translated into several languages including Swiss, German, Korean, Hebrew, Mandarin, Spanish and Greek. The validity and reliability data have been reported from the different patient and family member samples in situations of illness, diagnosis and treatment.14
The scale which was originally called the Parent's Perception Uncertainty in Illness Scale (PPUS) designed by Mishel (1983), contained 31 items distributed into 4 factors called ambiguity (13 items), lack of clarity (9 items), lack of information (5 items), and unpredictability (4 items). The scores ranged from 31 to 155 with a Likert type response scale which varied between 1 and 5, indicating that the higher the score the higher the degree of uncertainty. This scale has proven to have good indices of global internal validity and consistency, between .81 and .93. It also has internal consistency for each of the factors making up the original scale, Cronbach's alpha of .87 for ambiguity; .81 for the low clarity factor; .73 for the lack of information factor and .72 for the unpredictability factor.14 Additionally, internal consistency was reported to be .90 for the PPUS and there was a significant correlation between this and the scale called Illness Intrusiveness Scale Parent version (p<.05).15
Since there is currently no Spanish version with assessment of its psychometric properties, something which limits the assessment of uncertainty in parents and in this way its use in medical practise and research, in the Spanish speaking population, the aim of our study was to analyse the psychometric properties of the parent's perception of uncertainty in illness scale, parents/children, adapted to Spanish.
MethodA descriptive, methodological quantitative study involving two phases: translation and review of the Parent's Perception of Uncertainty in Illness scale, parents/children; analysis of their face validity, content validity, construct validity and definition of internal consistency and exploratory factorial analysis to assess the construct validity.
Direct translation was undertaken from the original language (English) to the language of application (Spanish) with the 2 versions made by different individuals being available (translator A and translator B). These translations were reviewed to assess if the significance of the re-translated items coincided with those of the original scale to ensure semantic equivalence and the final version obtained was submitted to inverse translation by an expert and qualified translator. In keeping with Luján and Cardona criteria, this version was approved by the author of the original scale.16
Face validity, known also as apparent, facies or representation validity, was defined with Morales’17 criteria and its objective was to determine the comprehension and clarity of one of the items. To do this, the scale was applied to a simple random sample of 310 subjects who were over 18. 92.2% were women and 7.7% were men with an average age of 29.5 years (SD: 10.58), and of different educational and socio cultural levels, who had attended a public health hospital centre during the period between February and April 2015 and had agreed to participate. Morales17 recommends using a sample 10 times higher than the number of variables or items (n=10k were k is the number of items or variables).
With this proposal, a format containing 31 items with 3 parallel boxes for each item was distributed and each participant was invited to read each statement carefully and qualify it by using one of the 3 boxes to indicate whether they understood the item, or they did not and for further precision, to include an observation in the third box.
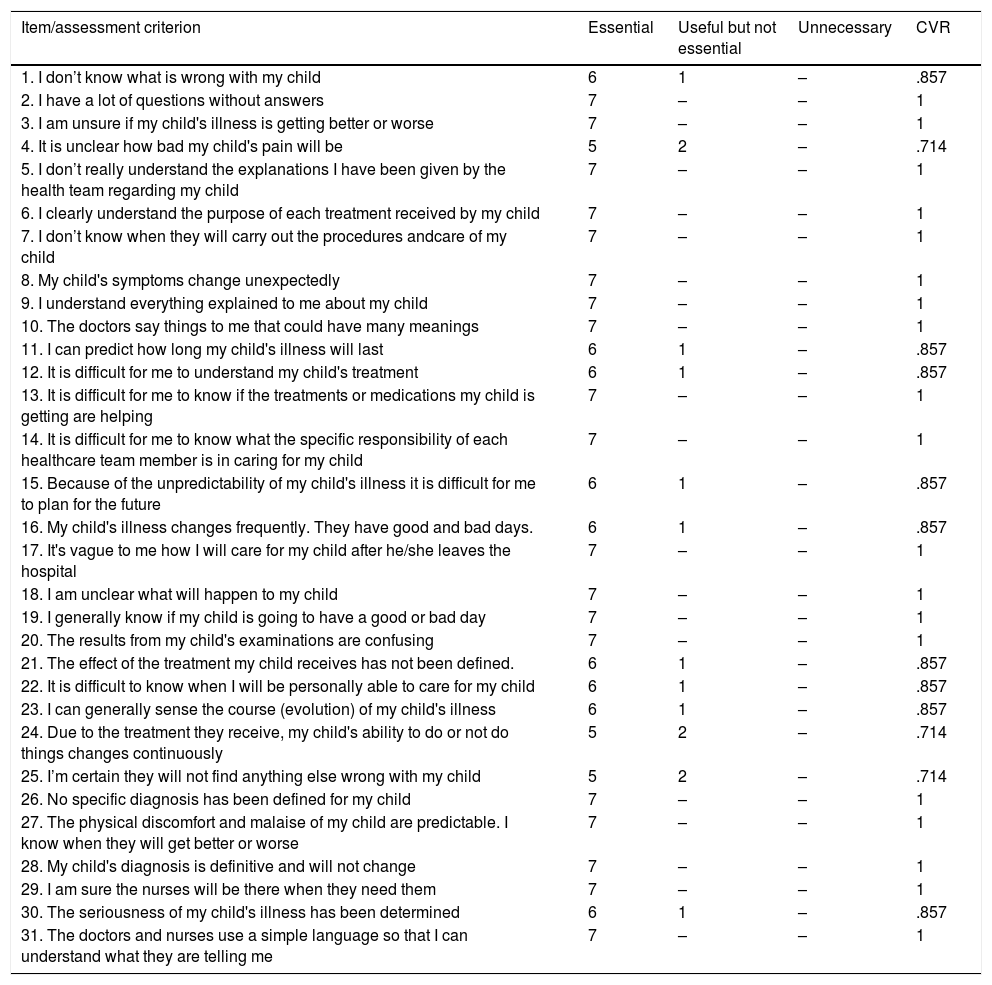
To determine content validity, by adhering to the proposal of Lawshe modified by Tristán,18 the scale was submitted to a panel of experts, comprising 7 nurses with teacher training or a doctorate in nursing, care professional experience and teaching experience in the area of caring for children and their families, and professionals who were familiar with the Theory of Uncertainty in Illness, to determine whether the scale explored all dimension or domains pertinent to the underlying construct. For this they assessed each item with 3 classification criteria: essential, useful but not essential or unnecessary. Content validity reasoning (CVR) was calculated for each item and this was understood to be the proportion of agreement of the judges in the essential classification over the total number of participant judges. To accept the agreement of the judges in each of the items, a CVR higher or equal to .58 had to be obtained for each of the items. After this, the content validity index of the global instrument was calculated, understood as the average value obtained. Aiken's19 coefficient V was used as confirmatory proof.
Construct validity was made using Morales’17 criteria again, from a non-probalistic by convenience sample, of 154 mothers with children who were hospitalised for different illnesses in paediatric departments or intensive care units in 2 health institutions, one public and the other private, during the period between February and September 2016 and who agreed to participate. Here we explored the correspondence between the factorial structure of the reponses to the items and the proposed theoretical dimensions. Calculation of the sample size for this analysis was made based on the minimum recommendation to use samples of at least 150 or 200 subjects variables (items) could be very few, establishing the minimum number of subjects as 100 and bearing in mind that the number of subjects had to be at least double the number of variables.17
As a preliminary exploration phase, we used the sample appropriateness test of Kaiser–Meyer–Olkin (KMO), the correlation matrix analysis and exploratory factorial analysis from estimation of the factorial loading matrix by the main component method and promax rotation. This methodological decision was taken because with regard to the theoretical construction and values of interfactor correlation, correlation was assumed to exist between the dimensions used and it was observed that the varimax and equamax orthogonals were not the most appropriate.20
The components with individual values superior to the unit were retrieved, which reported at least 10% of variation. For factor analysis standardised regression coefficients above four units21 were identified.
The reliability level was reviewed from the data of our sample described in the previous point and internal consistency of the global scale and the dimensions or factors were assessed using Cronbach's alpha coefficient. The cut-off point for this measurement22,23 was .7. Statistical analysis was performed in Microsoft Excel, Statistical Analysis System SAS version 9.4 and Statistical Package for the Social Sciences SPSS, version 22, with institutional licence for its usage.
This project adhered to the ethical and environmental guidelines established by the University of La Sabana. Also adhered to were the international ethical guidelines for biomedical research in human beings established by the Council for International Organisations of Medical Sciencies,24 and the regulations of the 1993 Resolution 8430 of the Colombian Ministry of Health.25
Validation of the scale for generic use for the parents of ill and hospitalised children forms part of a broader research project called the “effect of an interdisciplinary intervention on the level of uncertainty of mothers with hospitalised children in a paediatric intensive care unit of a private clinic in Bogota”, endorsed by the Ethics Committee of the University of La Sabana and financed by the Convocatoria Interna de Menor Cuantía, Code ENF-15-2013 in the same institution.
ResultsDuring the translation phase the Spanish version of 31 items was obtained, with no changes to structure and content from the original version.
Face or apparent validity of the scale reported 6 items with comprehension difficulty, judged by those who presented with a percentage of acceptability under 80% (Table 1). These items received a new process of exploration and review, obtaining an adjusted version which maintained the 31 items of the original scale.
Analysis of face or appearance validity from the percentage of acceptance of the items.
| Percentage of acceptance of the items | Number of items | Items |
|---|---|---|
| Items with 100% acceptance, % | 0 | |
| Items with over 90% acceptance, % | 12 | 5, 6, 9, 12, 13, 14, 16, 17, 21, 29, 30, 31 |
| Items with over 80% acceptance, % | 12 | 1, 2, 3, 4, 7, 10, 15, 18, 20, 25, 26, 28 |
| Items with over 60% acceptance, % | 7 | 8, 11, 19, 22, 23, 24, 27 |
In the content validity analysis using the CVR calculation for each of the items, none obtained a value under .58 and the original 31 item version was therefore maintained with an overall content validity index of .94, the criterion of which was verified with the obtainment of Aiken's coefficient V (Table 2).
Calculation of the content validity reasoning for each item.
| Item/assessment criterion | Essential | Useful but not essential | Unnecessary | CVR |
|---|---|---|---|---|
| 1. I don’t know what is wrong with my child | 6 | 1 | – | .857 |
| 2. I have a lot of questions without answers | 7 | – | – | 1 |
| 3. I am unsure if my child's illness is getting better or worse | 7 | – | – | 1 |
| 4. It is unclear how bad my child's pain will be | 5 | 2 | – | .714 |
| 5. I don’t really understand the explanations I have been given by the health team regarding my child | 7 | – | – | 1 |
| 6. I clearly understand the purpose of each treatment received by my child | 7 | – | – | 1 |
| 7. I don’t know when they will carry out the procedures andcare of my child | 7 | – | – | 1 |
| 8. My child's symptoms change unexpectedly | 7 | – | – | 1 |
| 9. I understand everything explained to me about my child | 7 | – | – | 1 |
| 10. The doctors say things to me that could have many meanings | 7 | – | – | 1 |
| 11. I can predict how long my child's illness will last | 6 | 1 | – | .857 |
| 12. It is difficult for me to understand my child's treatment | 6 | 1 | – | .857 |
| 13. It is difficult for me to know if the treatments or medications my child is getting are helping | 7 | – | – | 1 |
| 14. It is difficult for me to know what the specific responsibility of each healthcare team member is in caring for my child | 7 | – | – | 1 |
| 15. Because of the unpredictability of my child's illness it is difficult for me to plan for the future | 6 | 1 | – | .857 |
| 16. My child's illness changes frequently. They have good and bad days. | 6 | 1 | – | .857 |
| 17. It's vague to me how I will care for my child after he/she leaves the hospital | 7 | – | – | 1 |
| 18. I am unclear what will happen to my child | 7 | – | – | 1 |
| 19. I generally know if my child is going to have a good or bad day | 7 | – | – | 1 |
| 20. The results from my child's examinations are confusing | 7 | – | – | 1 |
| 21. The effect of the treatment my child receives has not been defined. | 6 | 1 | – | .857 |
| 22. It is difficult to know when I will be personally able to care for my child | 6 | 1 | – | .857 |
| 23. I can generally sense the course (evolution) of my child's illness | 6 | 1 | – | .857 |
| 24. Due to the treatment they receive, my child's ability to do or not do things changes continuously | 5 | 2 | – | .714 |
| 25. I’m certain they will not find anything else wrong with my child | 5 | 2 | – | .714 |
| 26. No specific diagnosis has been defined for my child | 7 | – | – | 1 |
| 27. The physical discomfort and malaise of my child are predictable. I know when they will get better or worse | 7 | – | – | 1 |
| 28. My child's diagnosis is definitive and will not change | 7 | – | – | 1 |
| 29. I am sure the nurses will be there when they need them | 7 | – | – | 1 |
| 30. The seriousness of my child's illness has been determined | 6 | 1 | – | .857 |
| 31. The doctors and nurses use a simple language so that I can understand what they are telling me | 7 | – | – | 1 |
The exploration of correspondence evidences between the factorial structure of response to items and dimensions proposed in the theory, reviewed using Barlett's sphericity test, enabled the null hypothesis “that the correlation matrix is the identity matrix” to be rejected, which led to sufficient statistical evidence being confirmed to guarantee that the correlations outside the diagonal were significantly different from zero (p value<.001).
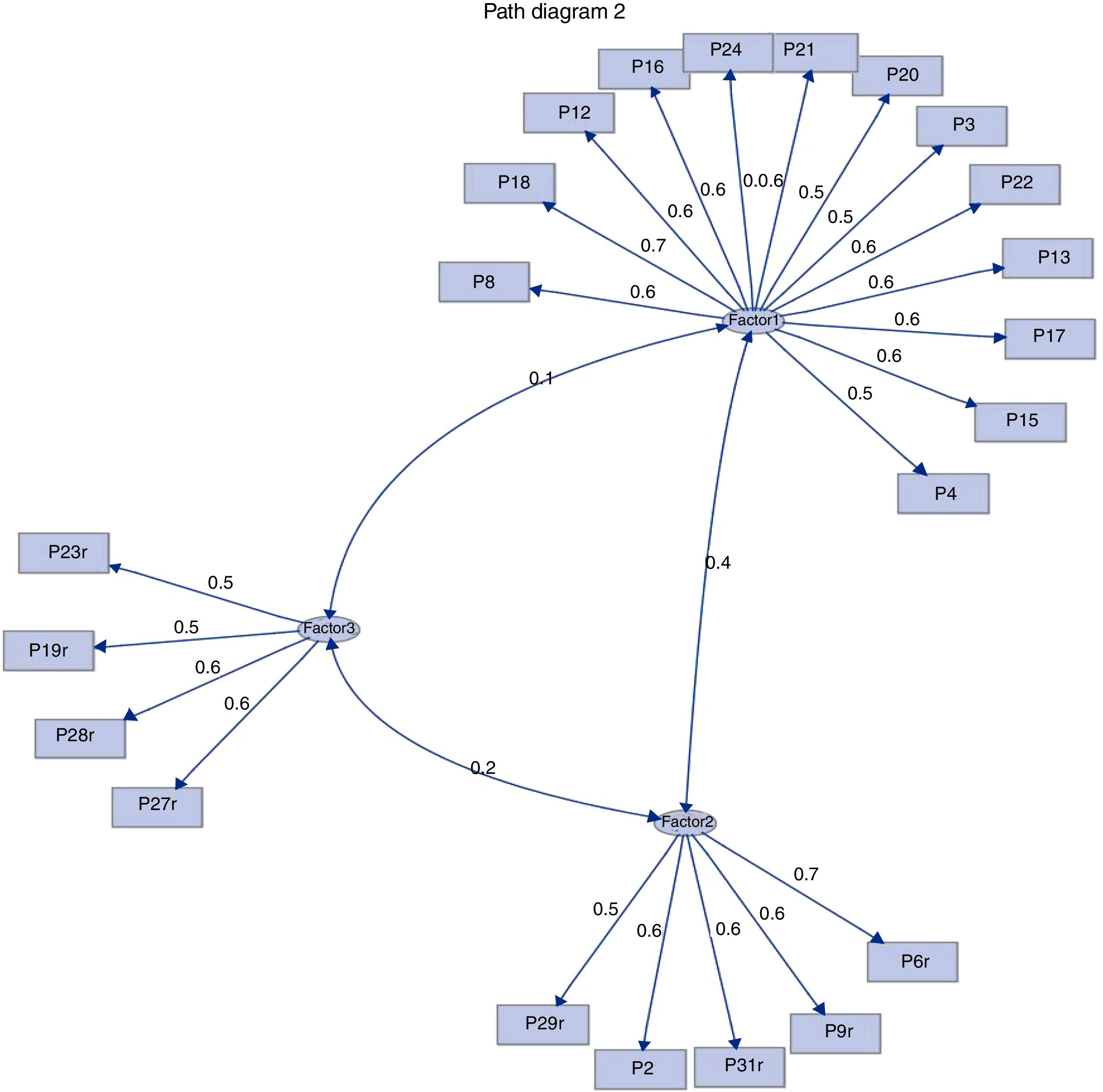
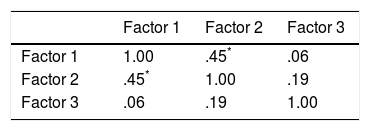
Exploratory factorial analysis was undertaken by assessing the 4 factors contained in the original version of the PPUS, with only 3 being identified that met with the criterion of own value above 1. The 3 criteria identified retained 91.53% of the total content of the original version in the following way: factor 1 retains ambiguity (59.68%), factor 2 corresponds to lack of clarity (19.12%), and factor 3 to unpredictability (12.73%). In addition to this, and in keeping with the analysis, a positive correlation was found to exist between factors 1 and 2 (Table 3).
To establish the correlation between the questions and the factors, we had to take into account standardised regression coefficients which were higher than .4 units; the questions were organised in the following way in accordance with the degree of correlation found with the 3 factors identified (Fig. 1 and Table 4):
Factor 1 – ambiguity: questions 3, 4, 8, 12, 13, 15, 16, 17, 18, 20, 21, 22 and 24.
Factor 2 – lack of clarity: questions 2, 6, 9, 29 and 31.
Factor 3 – unpredictability: questions 19, 23, 27 and 28.

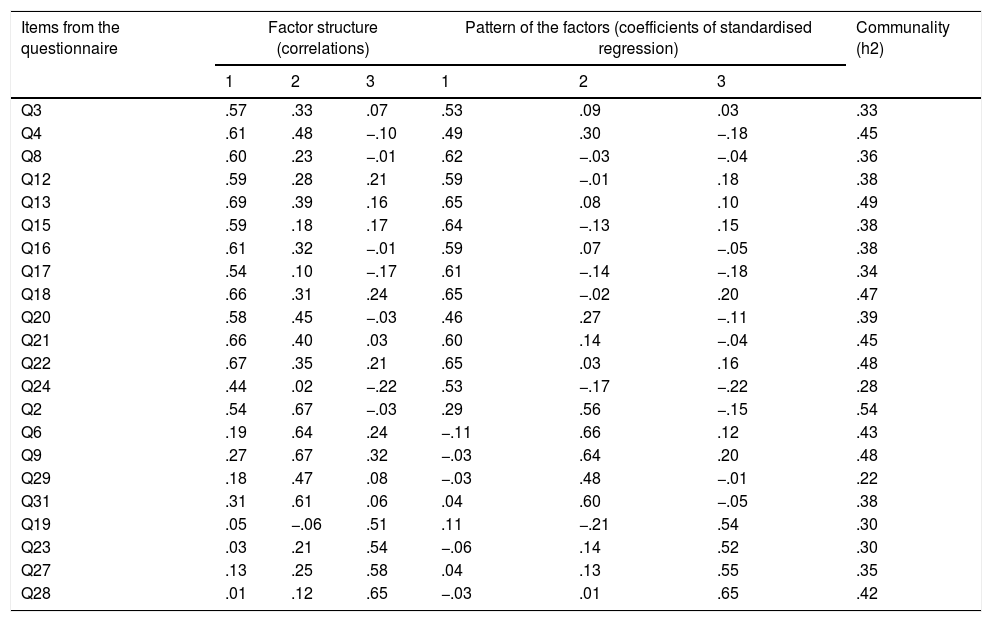
Items from the questionnaire: factorial loadings of the matrix of rotated factor patterns and of the matrix of factor structure and communality values (n=153).
| Items from the questionnaire | Factor structure (correlations) | Pattern of the factors (coefficients of standardised regression) | Communality (h2) | ||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | ||
| Q3 | .57 | .33 | .07 | .53 | .09 | .03 | .33 |
| Q4 | .61 | .48 | −.10 | .49 | .30 | −.18 | .45 |
| Q8 | .60 | .23 | −.01 | .62 | −.03 | −.04 | .36 |
| Q12 | .59 | .28 | .21 | .59 | −.01 | .18 | .38 |
| Q13 | .69 | .39 | .16 | .65 | .08 | .10 | .49 |
| Q15 | .59 | .18 | .17 | .64 | −.13 | .15 | .38 |
| Q16 | .61 | .32 | −.01 | .59 | .07 | −.05 | .38 |
| Q17 | .54 | .10 | −.17 | .61 | −.14 | −.18 | .34 |
| Q18 | .66 | .31 | .24 | .65 | −.02 | .20 | .47 |
| Q20 | .58 | .45 | −.03 | .46 | .27 | −.11 | .39 |
| Q21 | .66 | .40 | .03 | .60 | .14 | −.04 | .45 |
| Q22 | .67 | .35 | .21 | .65 | .03 | .16 | .48 |
| Q24 | .44 | .02 | −.22 | .53 | −.17 | −.22 | .28 |
| Q2 | .54 | .67 | −.03 | .29 | .56 | −.15 | .54 |
| Q6 | .19 | .64 | .24 | −.11 | .66 | .12 | .43 |
| Q9 | .27 | .67 | .32 | −.03 | .64 | .20 | .48 |
| Q29 | .18 | .47 | .08 | −.03 | .48 | −.01 | .22 |
| Q31 | .31 | .61 | .06 | .04 | .60 | −.05 | .38 |
| Q19 | .05 | −.06 | .51 | .11 | −.21 | .54 | .30 |
| Q23 | .03 | .21 | .54 | −.06 | .14 | .52 | .30 |
| Q27 | .13 | .25 | .58 | .04 | .13 | .55 | .35 |
| Q28 | .01 | .12 | .65 | −.03 | .01 | .65 | .42 |
Questions 1, 5, 7, 10, 11, 14, 25, 26 and 30 obtained factorial loadings below .4 units, indicating that no important correlation with any of the identified factors was present.
The general KMO value was .85 which would indicate a good level of samples adequacy (SAS, 2017),26 individually, the KMO values fluctuated between .61 for question 19 and .93 for question 18. As this was an exploratory analysis of factors no adjustment indices were generated, only the KMO and factorial loadings (regression coefficients) were shown and the factor structure which shows the general panorama with interfactorial correlations, and communalities.
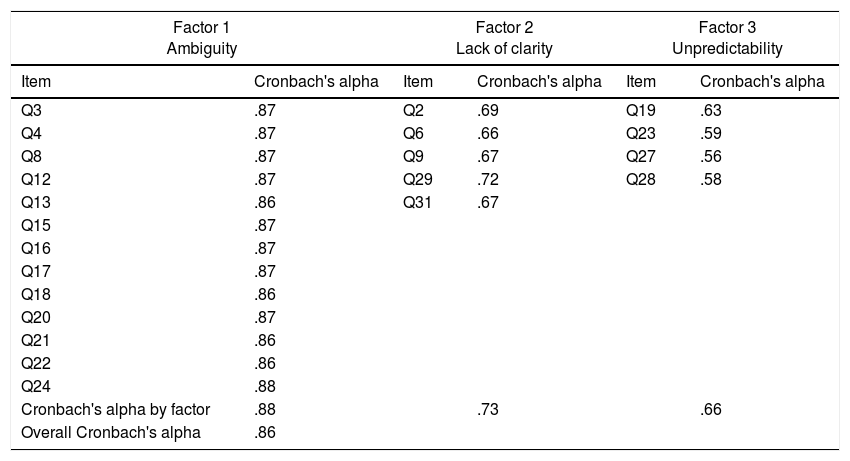
In accordance with the proposed objective for measuring the overall construct, reliability analysis was performed using the estimation of the internal consistency through Cronbach's alpha which reported a value of .86; for each of the factors identified. Cronbach's alpha ranged between .66 and .88 (Table 5).
Internal global consistence and by factors.
| Factor 1 Ambiguity | Factor 2 Lack of clarity | Factor 3 Unpredictability | |||
|---|---|---|---|---|---|
| Item | Cronbach's alpha | Item | Cronbach's alpha | Item | Cronbach's alpha |
| Q3 | .87 | Q2 | .69 | Q19 | .63 |
| Q4 | .87 | Q6 | .66 | Q23 | .59 |
| Q8 | .87 | Q9 | .67 | Q27 | .56 |
| Q12 | .87 | Q29 | .72 | Q28 | .58 |
| Q13 | .86 | Q31 | .67 | ||
| Q15 | .87 | ||||
| Q16 | .87 | ||||
| Q17 | .87 | ||||
| Q18 | .86 | ||||
| Q20 | .87 | ||||
| Q21 | .86 | ||||
| Q22 | .86 | ||||
| Q24 | .88 | ||||
| Cronbach's alpha by factor | .88 | .73 | .66 | ||
| Overall Cronbach's alpha | .86 | ||||
The design and validation of instruments for measuring phenomena relating to the care of people in a cultural context is a crucial aspect for research. Using instruments without validity and/or reliability leads to the measurement of theoretical aspects being invalid and prevents the advance of theoretical development in evidence-based practice.27
The scale reported good face or apparent and content validity, with the result being congruent with the data reported by the author. The original instrument reported an adequate construct validity from conventional factorial analysis techniques and varimax rotation in a sample of parents of hospitalised children and their findings provided proof of the grouping of the 31 items into a four-factor structure14; this finding differs from the factorial structure of responses obtained from the study sample of this research study, where 3 factors were identified. Questions 1, 5, 7, 10, 11, 14, 25, 26 and 30 did not mark any major correlation with any of the factors identified, and its review is recommended to optimise the correlation with the measured construct. Question 28, which in its original version belongs to the lack of information factor delivered a major correlation with the unpredictability factor, which suggests it could be included in the unpredictability factor instead, identified as the third in this study.
Initially with these findings it would not seem pertinent to rename factor 1 – ambiguity, since it retained 12 items of the 13 of the original version and only added one item belonging to another factor (item 12 – factor 3).
Similarly, the authors do not recommend eliminating the items which have no correlation with any factor. Although factor 2 (lack of clarity) only retained 5 out of the 9 original items and factor 3 (lack of information) did not retain any of its 5 items, meticulous review is required because from a theoretical viewpoint, these 2 factors refer to aspects of quantity and clarity of information which the person, in this case, the parents, have at their disposal, to comprehend the significance of the health status of their children in terms of diagnosis, treatment and prognosis. Sufficiency and relevance of information are crucial for explaining uncertainty which according to Mishel6 presents when information is insufficient, inappropriate or inconsistent. With the results from this validation and considering the limitations of this sample type and size, we consider it necessary to carry out a new factorial analysis with a larger sample size and then to perform confirmatory factorial analysis in a different sample to confirm the proposed factorial structure.
Overall reliability found in this work concurs with the data reported by Mishel. When applying the PPUS on parents of children with leukaemia, Mishel's14 results reflect that this is internally consistent with Cronbach's alpha .90; similar to that of Santacroce,28 who studied parents with children recently diagnosed with cancer, reporting on their study, an index of .88 for the total scale. With regard to reliability of the ambiguity factor, a similar value to that reported by Mishel was obtained. In contrast, in low clarity and unpredictability factors the values obtained for Cronbach's alpha were inferior to those reported by the original version of the scale.14
Among the limitations the sample size used for the development of factorial analysis stands out and the possible differences relating to the child's health status and the mother's cultural situation, which may affect the degree of uncertainty. The limited possibility of generalisation of the parents is also recognised because the sample only included the mothers.
We would recommend the continuous use and assessment of the scale to highlight its use in the world of healthcare practice. We also believe it necessary to repeat validation of the scale bearing in mind the use of a larger sample size and variations given in different linguistic contexts to confirm cultural equivalence in counties where Spanish is the main language.
Since it has been reported that negative emotions and feelings such as uncertainty may provoke sensations of impotence and inability to help loved ones,29 the Spanish version of the Parent's Perception of Uncertainly in Illness Scale is an important tool for medical practice and for future research studies aimed at assessing the level of uncertainty and generating strategies to regulate it.
FinancingThis project forms part of the so-called “effect of an interdisciplinary intervention on the level of uncertainty of mothers with hospitalised children in a paediatric intensive care unit of a presage clinical in Bogota, financed by the Convocatoria Interna de Menor Cuantía, University of La Sabana, code ENF-15-2013.
Conflict of interestsThe authors have no conflict of interests to declare.
The authors would like to thank the Fundación Cardioinfantil – Instituto de Cardiología (Bogota – Colombia), the Hospital de Suba E.S.E. (Bogota – Colombia) and the mothers who participated in allowing us to collect baseline information for the completion of this study.
Please cite this article as: Suarez-Acuña CE, Carvajal-Carrascal G, Serrano-Gómez ME. Escala de incertidumbre en la enfermedad – forma padres/hijos: validación de la adaptación al español. Enferm Intensiva. 2018;29:149–157.

