To assess the changes induced by the COVID-19 lockdown on cardiac biometric variables recorded using an implantable cardiac monitor (ICM) in a patient population monitored for syncope work-up, as well to assess whether there has been an effect on arrhythmic events among the patients.
MethodsLongitudinal cohort study. We included 245 adult patients monitored with an ICM indicated for the investigation of syncope. The records from days 1 to 12 March 2020 (prior to the institution of lockdown by the state government) with days 16 to 28 March 2020 were compared.
ResultsDaily physical exercise reduced markedly after the imposition of lockdown (132 [55–233] minutes vs. 78 [21–154] minutes). The mean daytime HR prior to lockdown was 77 [69–85] bpm, whereas during lockdown it was 74 [66–81] bpm. During the lockdown period, a drop in the variability in heart rate (114 [94–136] ms vs. 111 [92–133] ms) was observed. Although the incidence of AF was similar over both periods, the daily AF burden was significantly higher post-lockdown (405 [391–425] minutes vs. 423 [423–537] minutes). No differences in the number of other arrhythmias were found.
ConclusionsThe establishment of mandatory lockdown has led to a marked drop in daily physical activity in this population which probably explains changes observed in other cardiac biometric variables. Although, in the short term, we have not documented an increased risk of arrhythmia, we cannot rule out an effect in the medium to long term or in other populations of at-risk patients.
Evaluar los cambios inducidos por el confinamiento durante la pandemia de COVID-19 en las variables biométricas cardiacas registradas, utilizando un monitor cardíaco implantable (ICM) en una población de pacientes monitorizada para el diagnóstico de síncope, así como evaluar si ha habido un efecto sobre los eventos arrítmicos.
MétodosEstudio de cohorte prospectivo. Se incluyeron 245 pacientes adultos monitorizados con un ICM indicado para la investigación del síncope. Se compararon los registros de los días uno al 12 de marzo del 2020 (antes del establecimiento del confinamiento por parte del gobierno estatal) con los días 16 al 28 de marzo del 2020.
ResultadosEl ejercicio físico diario se redujo notablemente después de la imposición del confinamiento (132 [55 a 233] vs. 78 [21 a 154] min). La frecuencia cardiaca diurna media antes del confinamiento fue de 77 (69 a 85) lpm, mientras que durante el mismo fue de 74 (66 a 81) lpm. Durante el período de confinamiento, se observó una disminución de la variabilidad de la frecuencia cardiaca (114 [94 a 136] vs. 111 [92 a 133] ms). Aunque la incidencia de fibrilación auricular (FA) fue similar en ambos períodos, la carga diaria de FA fue significativamente mayor después del bloqueo (405 [391 a 425] vs. 423 [423 a 537] min). No se encontraron diferencias en el número de otras arritmias.
ConclusionesEl establecimiento de un confinamiento obligatorio ha provocado un marcado descenso de la actividad física diaria en esta población, lo que probablemente explica los cambios observados en otras variables biométricas cardiacas. Si bien, a corto plazo, no se ha documentado un aumento del riesgo de arritmia, no podemos descartar un efecto a medio-largo plazo o en otras poblaciones de pacientes de riesgo.
On March 14, 2020, the Spanish state government declared a state of emergency and instituted mandatory home lockdown for the population with a view to combatting the exceptional situation of the SARS-CoV-2 pandemic. This state of affairs, which has doubtless had an effect on controlling the epidemic, has also had collateral implications in many aspects of today's society. Several of these changes may have a significant impact on the population's health. For example, we have observed a clear reduction in pollution levels in major cities following the reduction of travel.1 To date, the impact on arrhythmic burden, physical exercise and cardiac biometric variables during lockdown and its possible consequences is unknown.
Prolonged electrocardiographic monitoring is mainly indicated for the work-up of syncope,2 palpitations3 and cryptogenic stroke.4,5 New generations of implantable cardiac monitors (ICMs) are subcutaneous implantable devices allowing not only for electrocardiographic monitoring, but also for other biometric variables as daily physical exercise.
The goal of this study was to assess the changes induced by the COVID-19 lockdown on cardiac biometric variables recorded using an ICM in a patient population monitored for syncope work-up, as well to assess whether there has been an effect on arrhythmic events among the patients.
The study complies with the Helsinki declaration and was approved by the center's ethics committee.
MethodsIn this longitudinal study carried out in a tertiary Spanish hospital, we included all consecutive adult patients monitored with a latest generation ICM (Reveal Linq™, Medtronic, Inc. Minneapolis. USA) indicated for the investigation of syncope as per applicable clinical practice guidelines2 and who had remotely sent the device records corresponding to the period from 1 to 28 March 2020 to the hospital. To summarize, ICM is indicated in patients in whom the full syncope work-up does not reach a certain diagnosis and they are considered at risk due to the clinical characteristics of the syncope, the presence of structural heart disease or conduction disorders.2,6 In selected patients with repeated reflex syncope it is indicated to guide treatment.
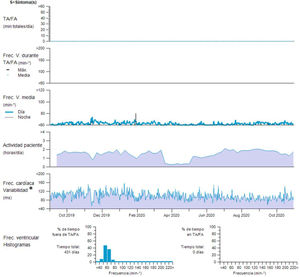
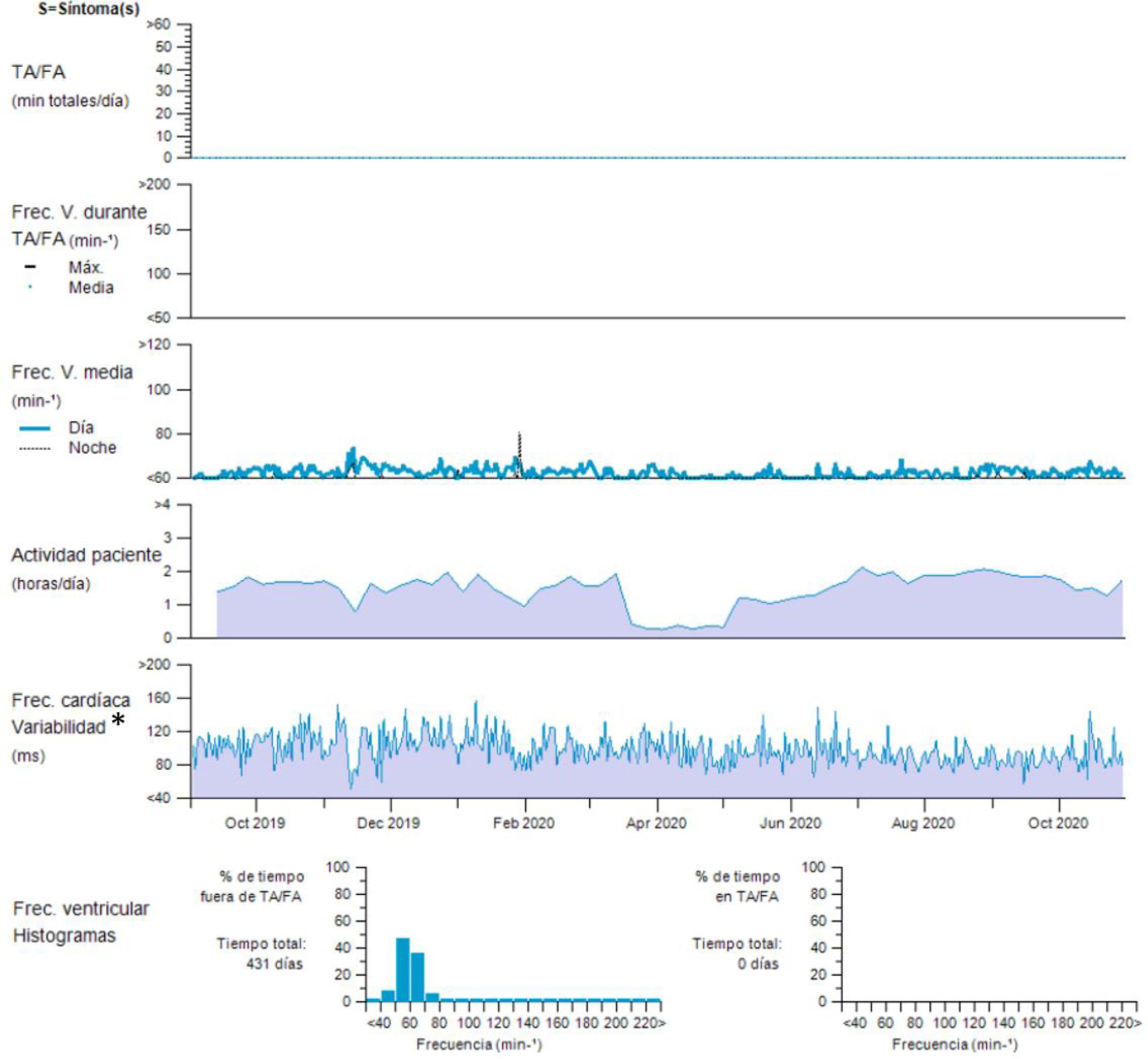
The ICM was programmed with the preconfigured settings for syncope. With these settings, the detection of atrial fibrillation is based both on irregularity of the RR interval and a P wave morphology indicated with a minimum episode duration of 6min. HR variability was measured by the device calculating the median ventricular interval every 5min. It then calculates and plots a variability value (in ms) for each day (supplementary figure).
We compared the records from days 1 to 12 March 2020 (prior to the institution of lockdown by the state government) with days 16–28 March 2020. The categorical variables are presented as an absolute number (N) and percentages and the continuous quantitative variables are presented as a median and interquartile range [IQR]. For the statistical analysis, we used paired data analysis. 95% confidence interval (CI) for the median of the differences between during and prior the lockdown period is reported. Non-paired data analysis was used where appropriate. All of the statistical tests were performed using Stata, version 15.1.0 (StataCorp LLC College Station, Texas, USA.).
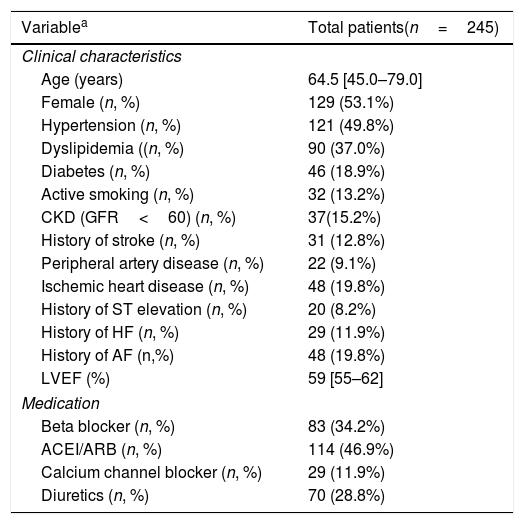
ResultsWe included a total of 245 patients. Table 1 summarizes the patients’ baseline characteristics. The median patient age at the time of inclusion was 64.5 years [IQR 45.0–79.0] and 129 (53.1%) were female.
Baseline characteristics.
| Variablea | Total patients(n=245) |
|---|---|
| Clinical characteristics | |
| Age (years) | 64.5 [45.0–79.0] |
| Female (n, %) | 129 (53.1%) |
| Hypertension (n, %) | 121 (49.8%) |
| Dyslipidemia ((n, %) | 90 (37.0%) |
| Diabetes (n, %) | 46 (18.9%) |
| Active smoking (n, %) | 32 (13.2%) |
| CKD (GFR<60) (n, %) | 37(15.2%) |
| History of stroke (n, %) | 31 (12.8%) |
| Peripheral artery disease (n, %) | 22 (9.1%) |
| Ischemic heart disease (n, %) | 48 (19.8%) |
| History of ST elevation (n, %) | 20 (8.2%) |
| History of HF (n, %) | 29 (11.9%) |
| History of AF (n,%) | 48 (19.8%) |
| LVEF (%) | 59 [55–62] |
| Medication | |
| Beta blocker (n, %) | 83 (34.2%) |
| ACEI/ARB (n, %) | 114 (46.9%) |
| Calcium channel blocker (n, %) | 29 (11.9%) |
| Diuretics (n, %) | 70 (28.8%) |
CKD: chronic kidney disease. GFR: glomerular filtration rate. HF: heart failure. LVEF: left ventricular ejection fraction.
aThe quantitative variables are expressed as a median [interquartile range].
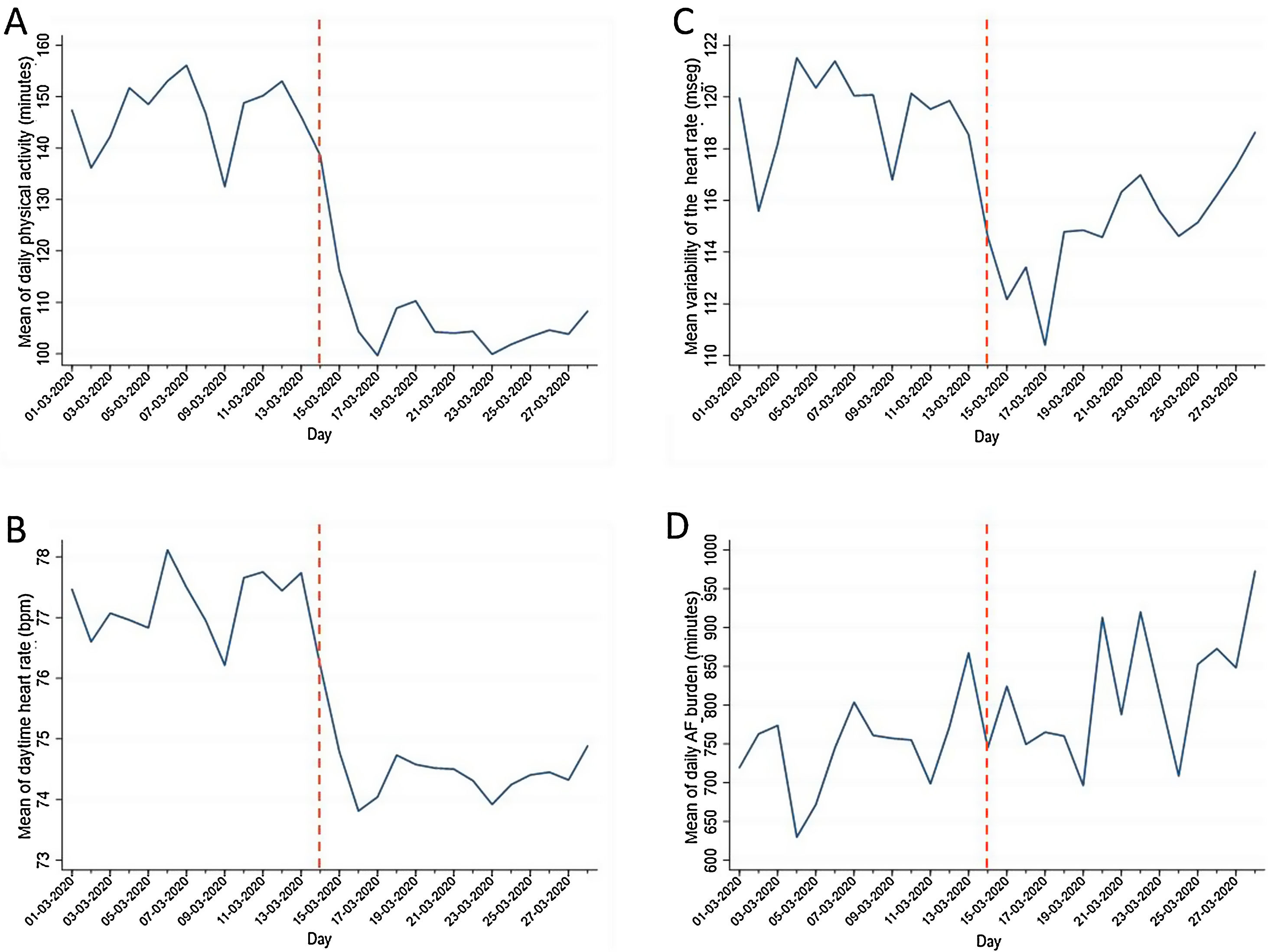
Daily physical exercise reduced markedly after the imposition of lockdown (132 [55–233] minutes prior the lockdown vs. 78 [21–154] minutes during to lockdown, median of the differences 33 [7–67] minutes; 95% CI from 25 to 41min) (Panel A, Fig. 1). The mean daytime HR prior to lockdown was 77 [69–85] bpm, whereas during lockdown it was 74 [66–81] bpm (median of the differences of 3 [0.2–5] bpm; 95% CI from 2 to 3.3min). During the lockdown period, a slight but significant drop in the variability in heart rate (114 [94–136] ms vs. 111 [92–133] ms; median of the differences of 3 [−3–9] ms; 95% CI from 1 to 5ms) was observed. This drop was more pronounced over the first few days of lockdown, and tended to normalize subsequently (Panel C Figure).
 Time graph showing the evolution of the average of daily physical activity, measured in minutes. Daily physical exercise reduced markedly after the imposition of lockdown. (B) Time graph showing the evolution of the mean daytime heart rate, measured in beats per minute. The mean daytime HR prior to lockdown was higher than during lockdown. (C) Time graph showing the evolution of the mean variability of the HR, measured in milliseconds. During the lockdown period, a slight drop in the variability in heart rate was observed. This drop was more pronounced over the first few days of lockdown and tended to normalize subsequently. (D) Time graph showing the average daily AF burden in patients who presented with AF crises, measured in minutes. Daily AF burden of the episodes was higher post-lockdown. The dashed red line marks March 14, 2020, the beginning of mandatory confinement. (AF: atrial fibrillation).")
(A) Time graph showing the evolution of the average of daily physical activity, measured in minutes. Daily physical exercise reduced markedly after the imposition of lockdown. (B) Time graph showing the evolution of the mean daytime heart rate, measured in beats per minute. The mean daytime HR prior to lockdown was higher than during lockdown. (C) Time graph showing the evolution of the mean variability of the HR, measured in milliseconds. During the lockdown period, a slight drop in the variability in heart rate was observed. This drop was more pronounced over the first few days of lockdown and tended to normalize subsequently. (D) Time graph showing the average daily AF burden in patients who presented with AF crises, measured in minutes. Daily AF burden of the episodes was higher post-lockdown. The dashed red line marks March 14, 2020, the beginning of mandatory confinement. (AF: atrial fibrillation).
In a total of 45 (18.4%) patients, we recorded atrial fibrillation (AF) during the study period. Of these, 7 (16%) were permanent and the rest were paroxysmal. Although the incidence of AF was similar over both periods, the duration (daily AF burden) of the episodes was higher post-lockdown (405 [391–425] min vs. 433 [423–537] min, with an increase of 28min; 95% CI from 18 to 45min) (Panel D and Table 2).
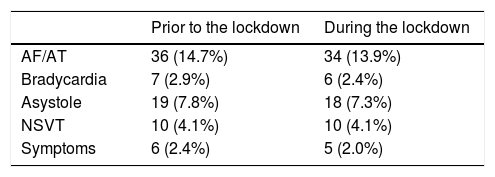
Number of patients with automatic events and activations due to symptoms detected by the ICM prior and during the lockdown.
| Prior to the lockdown | During the lockdown | |
|---|---|---|
| AF/AT | 36 (14.7%) | 34 (13.9%) |
| Bradycardia | 7 (2.9%) | 6 (2.4%) |
| Asystole | 19 (7.8%) | 18 (7.3%) |
| NSVT | 10 (4.1%) | 10 (4.1%) |
| Symptoms | 6 (2.4%) | 5 (2.0%) |
AF: atrial fibrillation; AT: Atrial tachycardia; NSVT: unsustained ventricular tachycardia.
A total of 7 patients activated the device due to symptoms. Their distribution was homogeneous over both periods. Similarly, we did not find any significant differences in the number of asymptomatic arrhythmias detected by the device (Table 2).
DiscussionTo our knowledge, this is the first case series exploring changes in cardiac biometric variables physical exercise and arrhythmic burden secondary to mandatory lockdown in the context of the SARS-CoV-2 epidemic and exploring its implications on arrhythmic burden.
In our project, based on a patient cohort monitored with an ICM as part of syncope work-up, we observed a marked reduction in daily physical exercise after declaration of the state of emergency. This fact probably explains the change observed in other biometric variables examined, such as mean daytime HR, which also significantly dropped in parallel with physical activity. In this sense, it is of interest to mention the evolution of heart rate variability (HRV). HRV is a measurement related to activity of the autonomic nervous system on cardiac function and it has been shown to be of prognostic value in different pathologies, as well as in the general population.7 It is known that prolonged sedentary lifestyle significantly reduces HRV.8,9 In our study, we observed a marked drop in HRV just after the start of lockdown, which tended to normalize progressively over the following days, which suggests there is a physiological adaptation to the situation. The clinical and prognostic implications of this behavior are unknown. In our project, we carried out an exploratory study on the effect on arrhythmic events. We did not find any significant differences in this population during the first days of lockdown, other than a greater duration of paroxysms of AF, although it would be interesting to assess the possible implications that these changes may have in the medium to long term.
ConclusionsThe declaration of the state of emergency and the instauration of mandatory lockdown have led to a marked drop in daily physical activity in this population which probably explains changes observed in other cardiac biometric variables. Although, in the short term, we have not documented an increased risk of arrhythmia, we cannot rule out an effect in the medium to long term or in other populations of at-risk patients. The data provided should be taken into account when planning similar strategies in the future should they be necessary.
Conflicts of interestThe authors have no conflicts to disclose.
The authors would like to thank Mr. Raúl Aguilar for his essential assistance in collecting the data, as well as Mr. Felix Ballesteros, Mr. Gonzalo Sánchez and Ms. Elena Fierro from Medtronic España for their technical support, as well as all of the staff in the arrhythmia unit for their daily work with these patients.