Un porcentaje importante de pacientes finalmente diagnosticados de amiloidosis cardIaca por transtirretina (ATTR) fueron previamente diagnosticados de cardiopatía hipertensiva (CHTA), ya que ambas enfermedades suelen cursar con insuficiencia cardíaca (IC) con fracción de eyección preservada (ICFEp) e hipertrofia ventricular. Nuestros objetivos fueron evaluar las diferencias clínicas, electrocardiográficas y ecocardiográficas, y analizar si existe un pronóstico diferencial entre ambas entidades nosológicas.
Material y métodosSe incluyeron retrospectivamente todos los pacientes con CHTA a los que se solicitó una gammagrafía cardíaca con 99mTc-Difosfonatos (GDPD) y estudio de cadenas ligeras en sangre y orina para despistaje de ATTR en nuestro centro, en el periodo 2016-2021. Para el análisis, se excluyeron aquellos diagnosticados de otros tipos de amiloidosis.
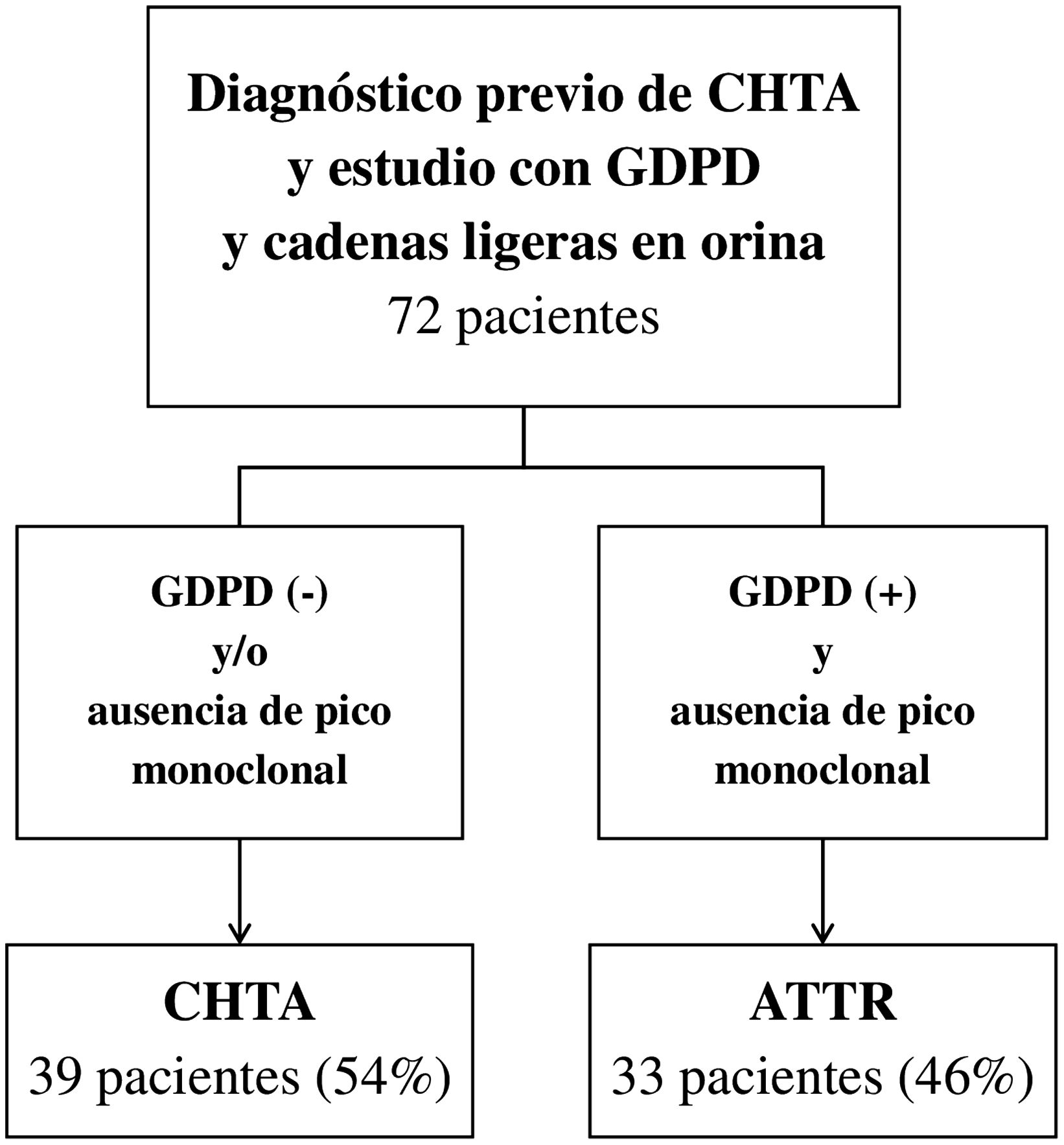
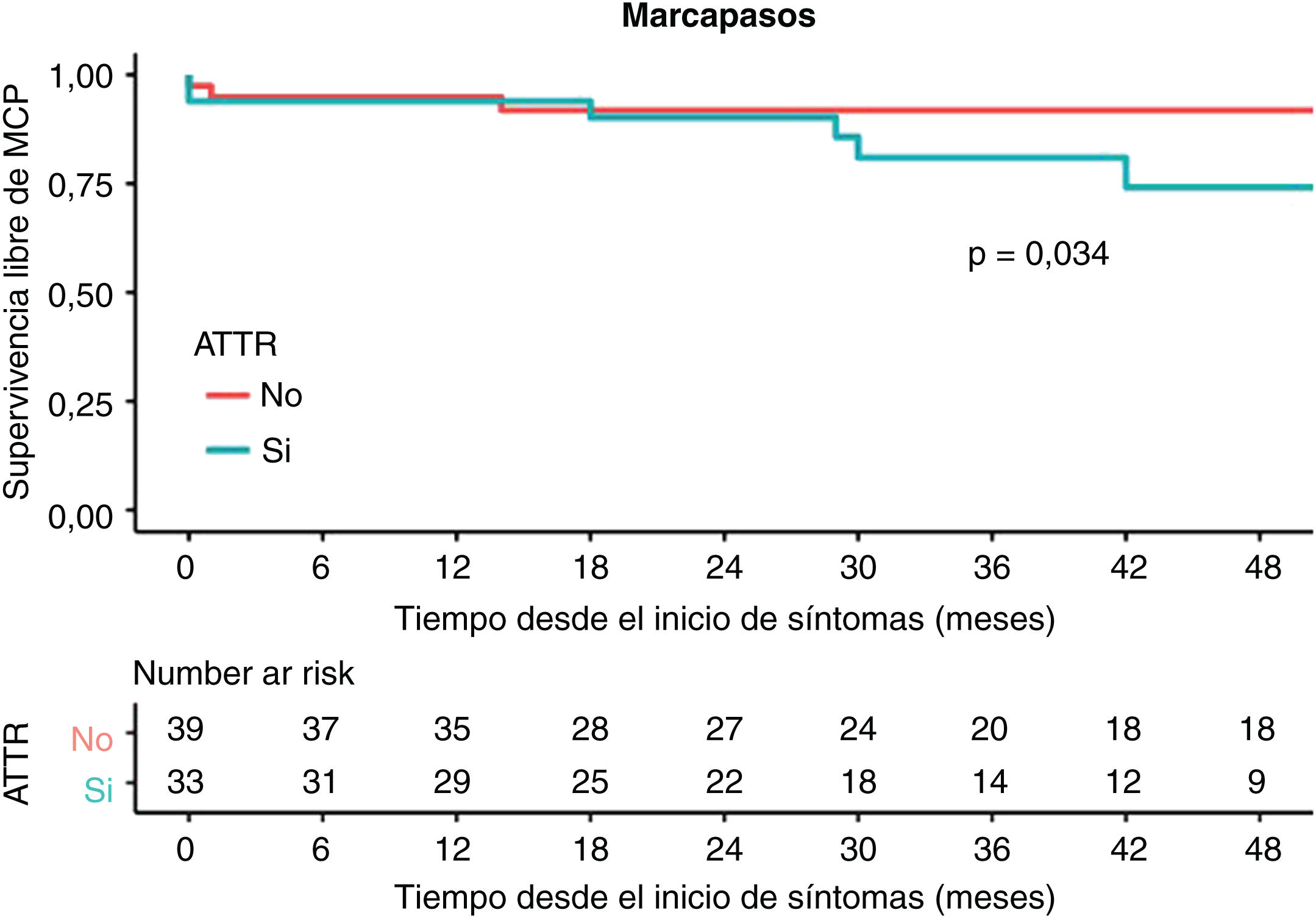
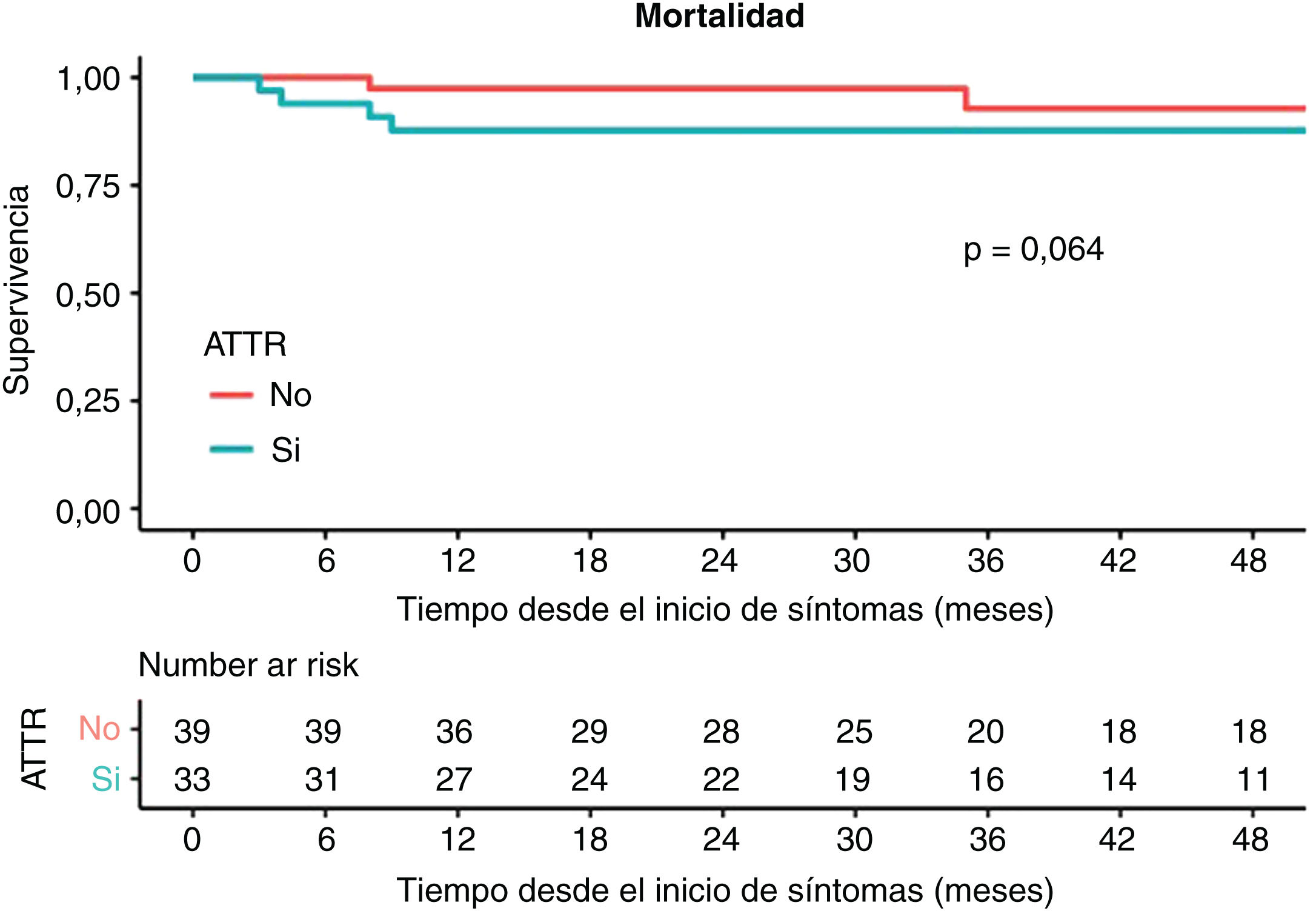
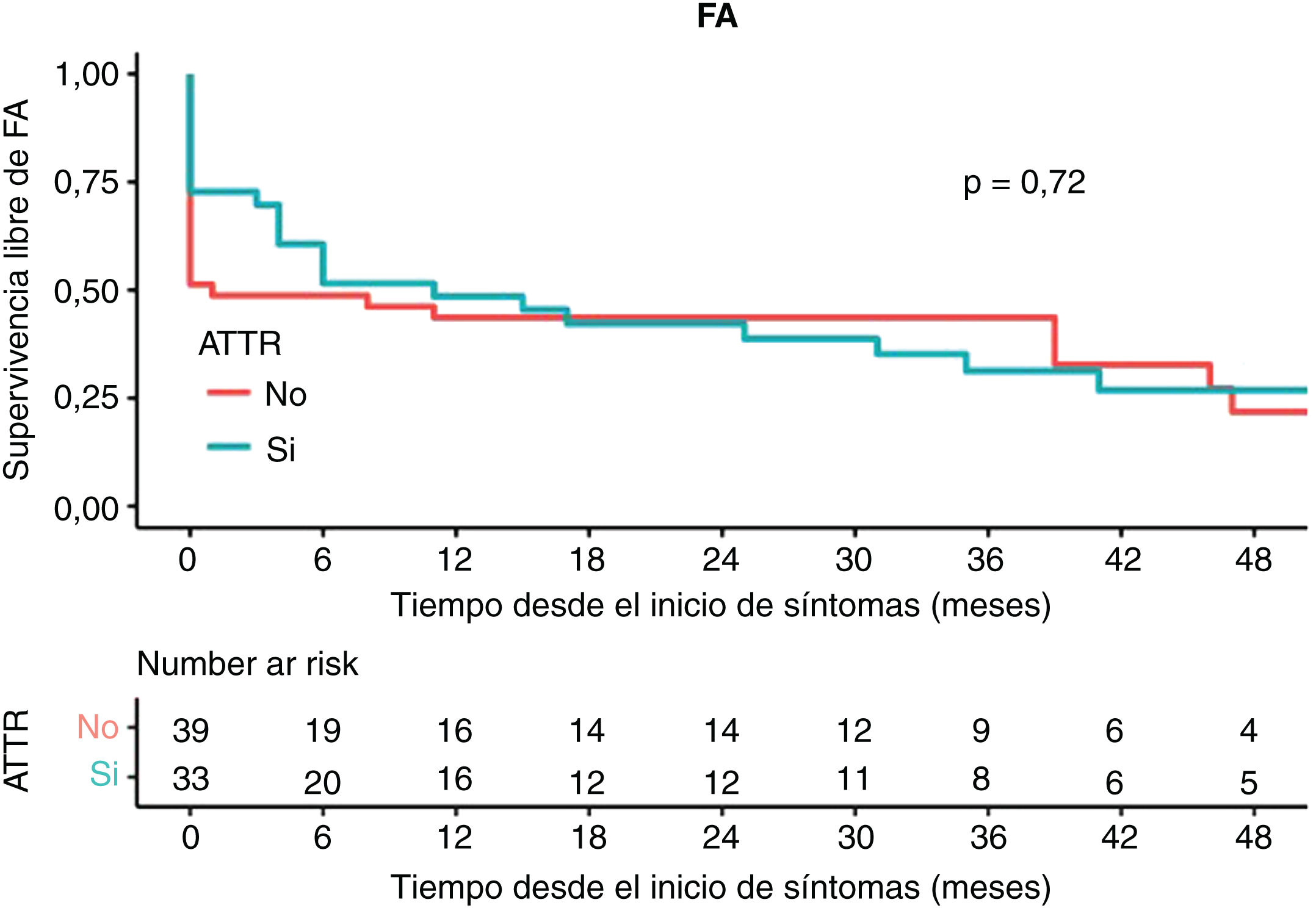
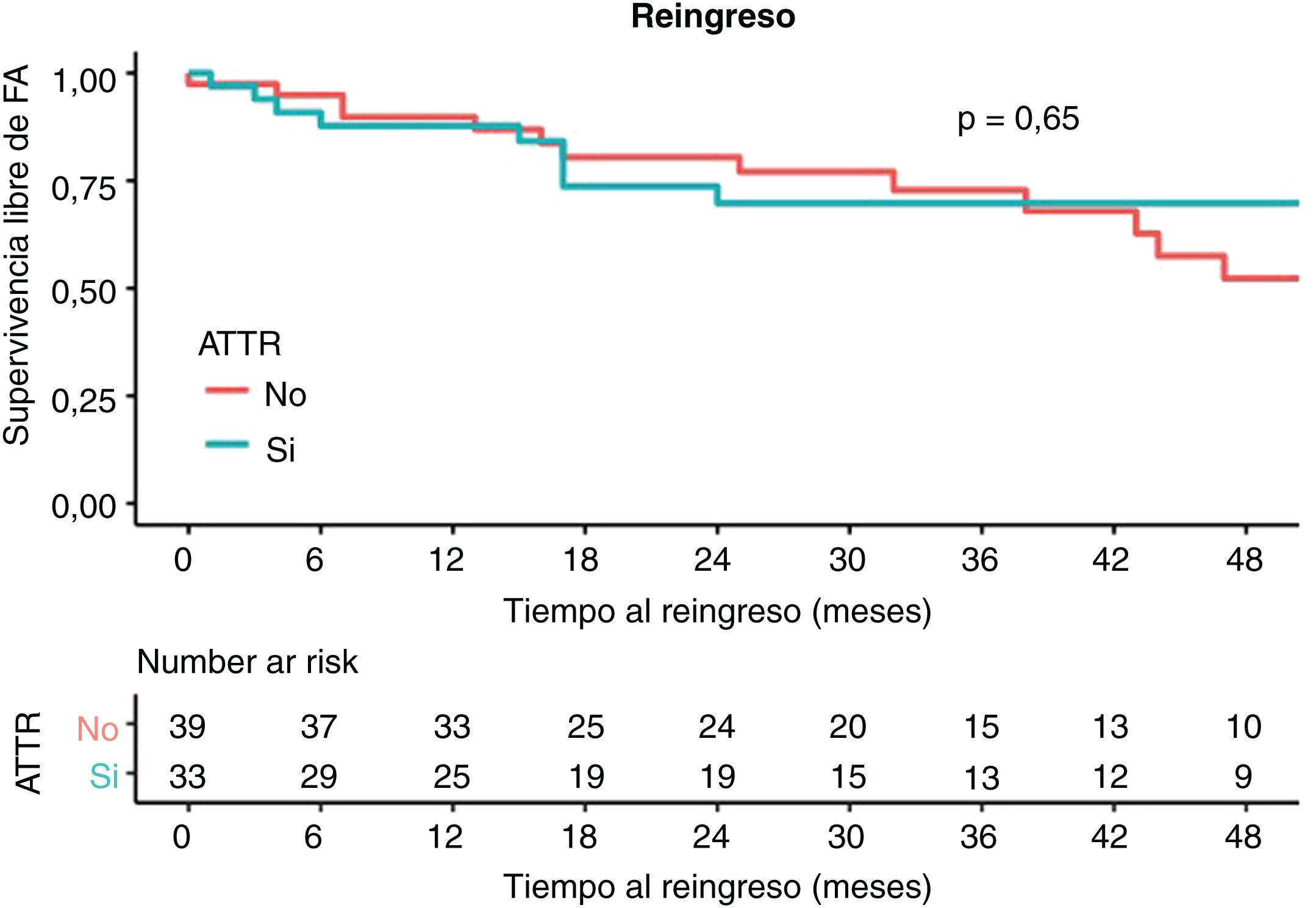
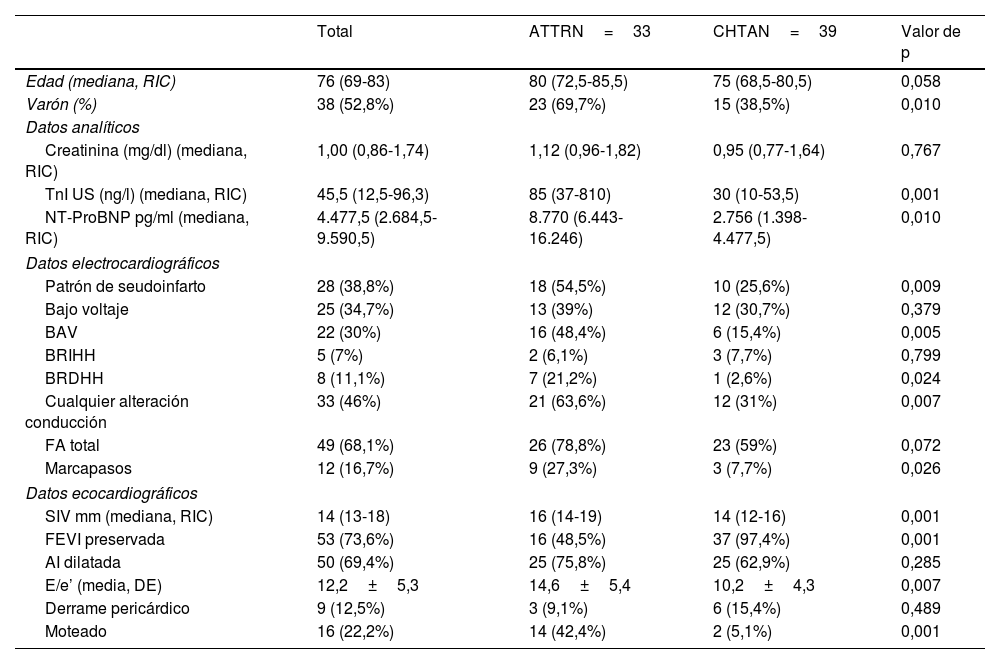
ResultadosSe analizaron un total de 72 pacientes: 33 fueron diagnosticados de ATTR y 39 de CHTA, finalmente. Los pacientes con ATTR presentaron mayores niveles de troponina I ultrasensible (TnI-US) y propéptido natriurético cerebral N-terminal (NT-ProBNP); en electrocardiograma (ECG) presentaron más frecuentemente patrón de seudoinfarto y alteraciones de la conducción; en ecocardiograma transtorácico (ETT) presentaron mayor grado de hipertrofia ventricular, disfunción ventricular izquierda y parámetros de peor función diastólica, con presiones de llenado más elevadas. En el seguimiento a 4 años, el grupo de ATTR mostró mayor necesidad de marcapasos (MCP), sin evidenciarse evidencias en cuanto a mortalidad, desarrollo de fibrilación auricular o más ingresos por IC.
ConclusionesEn nuestra serie, los pacientes con ATTR presentaron diferencias clínicas, electrocardiográficas y ecocardiográficas respecto a aquellos con CHTA, con mayor riesgo necesidad de MCP en el seguimiento.
A significant percentage of patients eventually diagnosed with cardiac transthyretin amyloidosis (TTRA) was previously diagnosed with hypertensive heart disease (HHD), since both conditions usually present with heart failure (HF) with preserved ejection fraction (HFpEF) and ventricular hypertrophy. Our objectives were to evaluate the clinical, electrocardiographic and echocardiographic differences, and to analyse whether there exists a differential prognosis between these two nosological entities.
Materials and methodsWe retrospectively included all patients with HHD for whom a cardiac scintigraphy with 99mTc-diphosphonate (GDPD) and a free light chains test in blood and urine were ordered for ATTR screening in our centre, in the period between 2016 and 2021. Those diagnosed with other types of amyloidosis were excluded from the analysis.
ResultsA total of 72 patients were analyzed: 33 were finally diagnosed with TTRA and 39 with CHTA. Patients with TTRA had higher levels of ultrasensitive troponin I (TnI-US) and N-terminal brain natriuretic propeptide (NT-ProBNP); in electrocardiography (ECG) they presented a pseudo-infarction pattern more frequently as well as conduction disturbances; in echocardiography (TTE) they presented a higher degree of ventricular hypertrophy, left ventricular dysfunction and worse diastolic function parameters, with elevated filling pressures. In the 4-year follow-up, the ATTR group showed greater need for pacemaker (PCM), with no evidence regarding mortality, development of atrial fibrillation (AF), or more admissions for heart failure (HF).
ConclusionsIn our series, patients with TTRA showed clinical, electrocardiographic and echocardiographic differences compared to patients with HHD, with increased risk of need for PCM.