




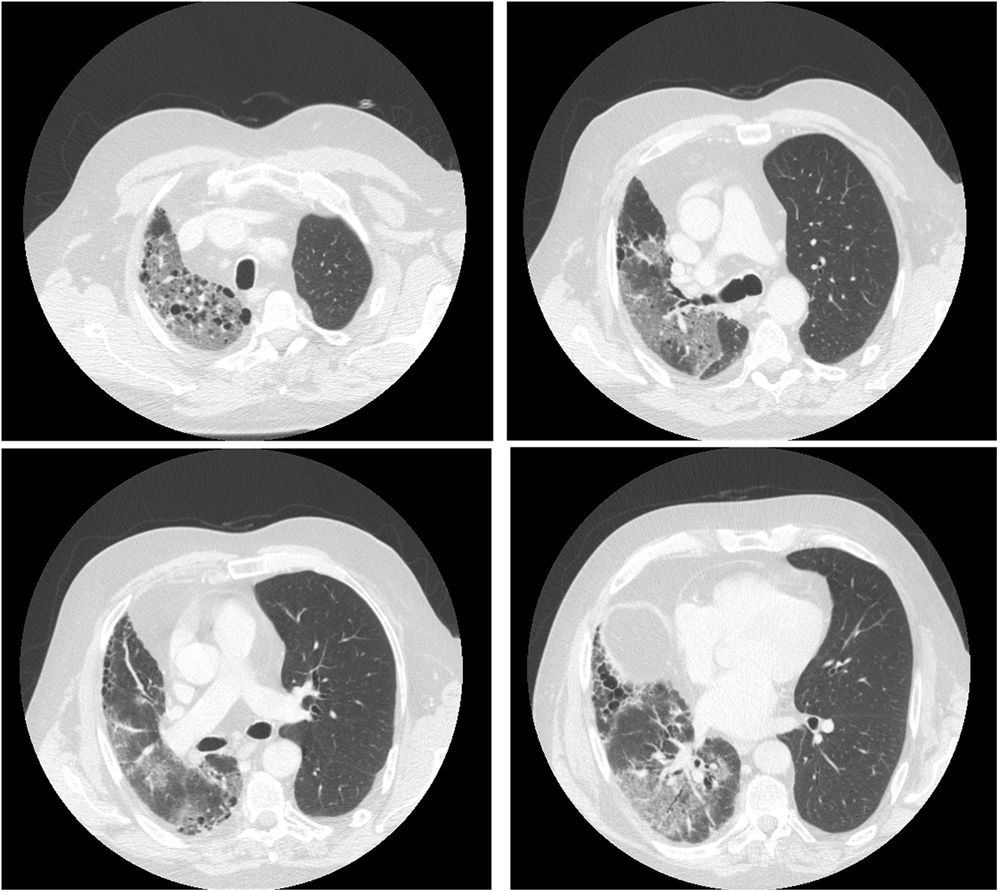
58-year-old male patient with single-lung transplantation in March 2018 due to idiopathic pulmonary fibrosis. No relevant complications after transplantation, good functional status and an m-MRC functional class of 0 points. The patient had a confirmed SARS-CoV-2 infection 7 days prior to hospital admission. The symptoms included high fever, dry irritative cough and dyspnoea, as well as O2 desaturation and confirmed hypoxemic respiratory failure on arterial blood gas analysis. Chest CT demonstrated the presence of ground glass areas in the native lung, compatible with COVID-19 pneumonia, without involvement of the transplanted lung (Fig. 1). Other causes, such as infection by Cytomegalovirus (CMV) or bacterial pneumonia, were ruled out. The fact that it presents with exclusive involvement of the native lung, while sparing the transplanted lung, suggests that there must be molecular mechanisms by which the virus has a greater affinity for some hosts than others. This mechanism of exclusive involvement of the native lung has been described in other viruses such as CMV but has not been described in SARS-CoV-2, which has had a major impact among lung transplant patients.1,2 Fortunately, a satisfactory function and the absence of involvement in the transplanted lung allowed him to make good progress and was discharged from hospital in 10 days.

Please cite this article as: Mora Cuesta VM, Iturbe Fernández D, González Ramos L. Neumonía por COVID-19 que afecta solo al pulmón nativo en trasplante unipulmonar. Med Clin (Barc). 2021;157:e324.
