




Olfactory and taste dysfunction (OD, TD) have been considered symptoms of SARS-CoV-2 infection. However, its presence in certain populations, especially those with mild clinical symptoms, has not been clarified. The objective was to estimate the frequency of OD and TD, and its predictive validity in patients detected in Primary Care.
Patients and methodsA cross-sectional study was carried out in the Spanish National Health System. An epidemiological survey was administered to patients who were requested the PCR test for SARS-CoV-2. Odds ratio (OR) were estimated to measure the magnitude of the association between OD and TD and the existence of SARS-CoV-2 infection. The sensitivity, specificity, and positive and negative predictive values (PPV, NPV) of these symptoms in SARS-CoV-2 infection were calculated.
ResultsOf 1038 patients screened, 20.1% had SARS-CoV-2 infection. OD and DG were present in 64.4% (95% CI 56.0–72.1) and 56.2% (95% CI 47.9–64.2) of the subjects with infection, respectively. The OR for OD was 12.2 (95% CI 8.26–18.06) and for TD was 7.95 (95% CI 5.48–11.53). TD presented a sensitivity of 41.1% (95% CI 34.4–46.1), a specificity of 91.9% (95% CI 89.8–93.7), a PPV of 56.2% (95% CI48.0–64.2) and a NPV of 86.1% (95% CI 83.6–88.3), while the OD showed a sensitivity of 45.0% (95% CI 37.6–51.5), a specificity of 93.7% (95% CI 91.8–95.0), a PPV of 64.4% (95% CI 56.0–72.1) and a NPV of 87.1% (95% CI 84.7–89.2).
ConclusionsMore than half of the subjects with SARS-CoV-2 infection have OD or TD. The presence of OD or TD could be of diagnostic utility due to its ability to predict infection in more than half of the cases.
La disfunción olfatoria (DO) y gustativa (DG) han demostrado ser síntomas de la infección por SARS-CoV-2. Sin embargo, su presencia en determinadas poblaciones, sobre todo en aquellas con cuadros clínicos leves, aún debe aclararse. El objetivo fue estimar la frecuencia de DO y DG, y su validez predictiva en pacientes detectados en Atención Primaria.
Pacientes y métodosSe realizó un estudio transversal en el Sistema Nacional de Salud español. Se administró una encuesta epidemiológica dirigida a pacientes a los que se les solicitó la prueba PCR para SARS-CoV-2. Se estimaron las odds ratio (OR) para medir la magnitud de la asociación entre la DO y DG y la existencia de infección por SARS-CoV-2. Se calculó la sensibilidad, la especificidad y los valores predictivos positivos (VPP) y negativos (VPN) de estos síntomas en la infección por SARS-CoV-2.
ResultadosSe captaron 1.038 pacientes, de los cuales el 20,1% presentaban infección por SARS-CoV-2. Las DO y DG estuvieron presentes en el 64,4% (IC 95% 56,0–72,1) y el 56,2% (IC 95% 47,9–64,2) de los sujetos con infección, respectivamente. La OR para la DO fue de 12,2 (IC 95% 8,26−18,06) y para la DG de 7,95 (IC 95% 5,48−11.53). La DG presentó una sensibilidad del 41,1% (IC 95% 34,4–46,1), una especificidad del 91,9% (IC 95% 89,8–93,7), un VPP del 56,2% (IC 95% 48,0–64,2) y un VPN de 86,1% (IC 95% 83,6–88,3), mientras que la DO mostró una sensibilidad del 45,0% (IC 95% 37,6–51,5), una especificidad del 93,7% (IC 95% 91,8–95,0), un VPP del 64,4% (IC 95% 56,0–72,1) y un VPN del 87,1% (IC 95% 84,7–89,2).
ConclusionesMás de la mitad de los sujetos con infección por SARS-CoV-2 presentan DO o DG. La presencia de DO o de DG podría ser de utilidad diagnostica por su capacidad para predecir la infección en más de la mitad de las ocasiones.
Since the emergence of the first cases in Wuhan City, China, coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2), has spread rapidly,1 generating a total of 38,620,496 cases and 1,093,921 deaths worldwide as of October 2020.2 With the declaration of an international health emergency on 30th January and pandemic notification on 11th March, COVID-19 disease remains a global health challenge.3
SARS-CoV-2 infection can be asymptomatic (especially in younger patients) or produce mild, moderate, or severe clinical manifestations, with a wide and diverse array of symptoms.4 In Spain, the most commonly described symptoms are fever (69%), cough (68%), sore throat (24%), dyspnoea (31%), and chills (27%).5 In addition, other symptoms related to different organs and systems have been identified, among which olfactory dysfunction (OD) and taste dysfunction (TD) stand out.6 The frequency with which hyposmia-anosmia and hypogeusia-dysgeusia occur ranges from 5% to 88% of patients according to international series.7–9 Preliminary results from the first seroprevalence study in Spain indicate that the prevalence of anosmia in patients diagnosed by COVID-19 was 43.3% (95% CI 39.9–46.8).10
Recent studies reveal that the variation in OD in the population is due to the expression of angiotensin converting enzyme 2 (ACE-2) in the nasal mucosa,11 which can vary substantially between populations,12 which could explain the possible higher prevalence of OD in the European population affected by COVID-19 compared to the Asian population,13 given the higher expression of this enzyme in the nasal mucosa of the European population.14 With regard to TD, recently Xu et al.15 described the high expression of ACE-2 in the epithelial cells of the oral cavity, which could justify the entry of the virus into the taste nerve endings.
Various studies have indicated that OD or TD may be one of the initial symptoms of the disease.16–18 A study carried out in 180 COVID-positive patients in Italy showed that 46.7% of the patients presented OD as the initial symptom of the disease, thus suggesting that OD may be the initial manifestation of the disease.16 Similarly, a multicenter pilot study carried out in Spain indicated that OD or TD occurred in 35.5% of cases as the onset symptom.18
Research conducted in patients with suspected COVID-19, registered through a mobile application in the United Kingdom and the USA, showed that loss of taste and smell is a potential predictor of COVID-19 disease.8 A subsequent study by the same research group showed that the predictive ability of loss of smell and taste was superior to that identified for other symptoms such as fever or persistent cough.19 Along the same lines, a European investigation carried out in patients with mild-moderate COVID-19 disease indicated that OD is a "key symptom" in COVID-19 infection and is influenced by age and sex, its manifestation being higher in women and in young people.20
Despite the impact that COVID-19 disease has had in Spain, there is still a high level of ignorance about the prevalence and clinical relevance of these symptoms in relation to this disease, especially among patients with mild symptoms who are detected in the Primary Care (PC) setting, despite the fact that they represent more than 80% of the reported cases.21
The main objective of the study was to estimate the frequency of OD and TD in patients with SARS-CoV-2 infection, detected in the PC setting. As secondary objectives, we aimed to determine the socio-demographic and clinical characteristics of these patients and the degree of association between OD and TD and SARS-CoV-2 infection, and to assess the criterion validity of these symptoms in the prediction of COVID-19.
Material and methodsA cross-sectional observational study was designed, using a control group for comparison. The study was carried out following the recommendations of the STROBE guidelines.22
The scope of the study was, on the one hand, the South Healthcare Management Area of Córdoba and the Córdoba and Guadalquivir Healthcare District (both institutions belonging to the Andalusian Health Service [SAS]), and on the other, the whole of the Spanish territory, through the Spanish Society of Family and Community Medicine (semFYC). Subjects who underwent a PCR test (real-time polymerase chain reaction [RT-PCR] in a nasal/pharyngeal swab) for the detection of SARS-CoV-2 during the period between 28th March and 31st May 2020 were recruited.
The sample size was calculated accepting an alpha risk of 0.05 and a beta risk of 0.2, in a bilateral contrast, to detect a minimum odds ratio (OR) of two, assuming that the rate of patients with OD or DG in the control group (patients without SARS-CoV-2 infection) would be 14%, and a ratio between the group of cases (patients with SARS-CoV-2 infection) and that of controls of 1:4. With these premises it was estimated that 163 cases with COVID-19 and 652 in the control group would be required (calculations made with the Granmo v.7.12® software (https://www.imim.cat/ofertadeserveis/software-public/granmo/).
Two methods were used to obtain the information. In the first phase, patients recruited in the above-mentioned health areas, who had a nasopharyngeal sample taken for COVID-19 diagnosis, were given a personal telephone interview to inform them of the result and to go through an epidemiological questionnaire. In the second phase, data were obtained by means of a self-completed survey filled in by the patient on-line. To this end, the heads of research of the semFYC member societies were contacted, inviting them to participate in the dissemination of the study and the recruitment of professionals who met the inclusion criteria (having had a PCR test for SARS-CoV-2). Finally, 12 of the 17 Autonomous Regions of Spain (Andalusia, Aragon, Asturias, Balearic Islands, Castilla-León, Castilla-La Mancha, Euskadi, Galicia, Madrid, Murcia, Navarra, and La Rioja) participated. The questionnaire was created using the Google Forms tool in Drive® (https://docs.google.com/forms/d/e/1FAIpQLSeYTw5lmJnQKNN6SDp73KN5M0e7kFIFTZkOSOdDuEpKcZkUuA/viewform), collecting the following variables data: sociodemographic (age, sex, area of residence [urban: town/city ≥20,000 inhabitants vs. rural], institutionalized vs. non-institutionalized), profession (healthcare personnel vs. non-healthcare), type of health coverage (public or private health insurance or both), symptoms present in recent weeks (including OD or TD), and result of the PCR test for the SARS-CoV-2 coronavirus (positive, negative or inconclusive).
A univariate and bivariate statistical analysis was performed, comparing the characteristics of both groups (positive cases of SARS-CoV-2 versus negative cases), using a hypothesis contrast test, such as the χ2 test or Fisher's exact test, and the Student's t test (after checking the normal distribution fitness, applying the Kolmogorov–Smirnov test). To estimate the magnitude or strength of association between the presence of OD and/or TD and the SARS-CoV-2 infection, ORs were calculated. To analyse the predictive validity of OD and TD to detect COVID-19 infection, the sensitivity and specificity parameters were calculated, as well as the positive predictive values (PPV) and negative predictive values (NPV) of these symptoms, with their 95% confidence intervals (95% CI). Finally, a binary logistic regression analysis was performed, taking into account the presence of SARS-CoV-2 infection (Yes/No) as the dependent variable, and sex, age, and profession as independent variables. The goodness-of-fit of the model was verified with the Hosmer-Lemeshow test. The statistical analysis was done with the SPSS v.17.0® and EPIDAT 4.2® software.
The project complied with the standards of good clinical practice (art.34 RD 223/2004; EU directive 2001/20/EC), and with the protection of personal data and confidentiality (European Data Protection Regulation, and in accordance with Organic Law 3/2018 on the Protection of Personal Data and Guarantee of Digital Rights).
The study was authorized by the Córdoba and Guadalquivir Healthcare District and by the South Córdoba Health Management Area and approved by the Clinical Research Ethics Committee of the Reina Sofía Hospital in Córdoba. All patients were asked for their informed consent before completing the epidemiological survey.
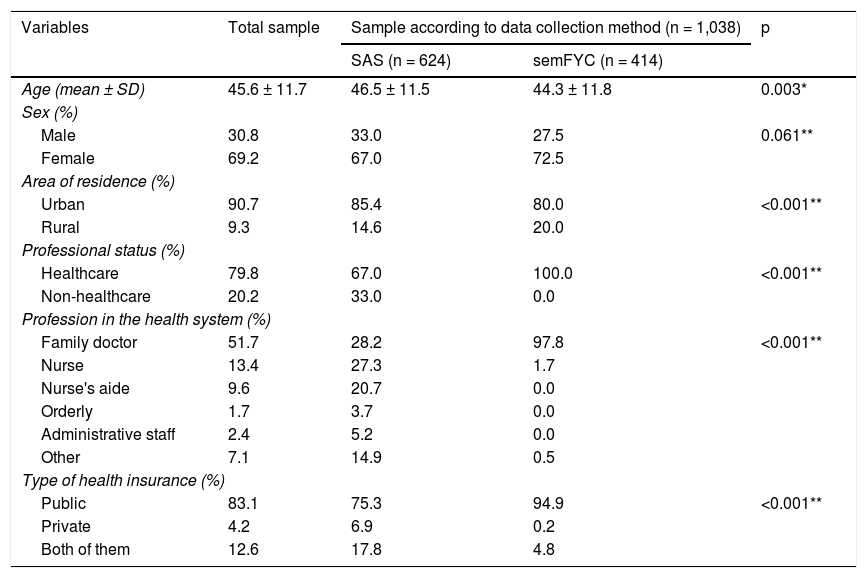
ResultsA total of 1,038 subjects were evaluated, of whom 624 were interviewed by the Epidemiology Department of the SAS, and 414 by mail sent to the members of the participating semFYC affiliated societies. Table 1 shows the socio-demographic and employment characteristics of the subjects studied, according to the method for collecting and obtaining the information. The global mean age (±standard deviation) was 45.6 ± 11.7 years (limits 12–94); 69.2% were women. 79.8% were professionals who worked in PC, and of these, 51.7% were family doctors.
Sociodemographic and employment characteristics of the subjects studied, according to the method for collecting and obtaining the information.
| Variables | Total sample | Sample according to data collection method (n = 1,038) | p | |
|---|---|---|---|---|
| SAS (n = 624) | semFYC (n = 414) | |||
| Age (mean ± SD) | 45.6 ± 11.7 | 46.5 ± 11.5 | 44.3 ± 11.8 | 0.003* |
| Sex (%) | ||||
| Male | 30.8 | 33.0 | 27.5 | 0.061** |
| Female | 69.2 | 67.0 | 72.5 | |
| Area of residence (%) | ||||
| Urban | 90.7 | 85.4 | 80.0 | <0.001** |
| Rural | 9.3 | 14.6 | 20.0 | |
| Professional status (%) | ||||
| Healthcare | 79.8 | 67.0 | 100.0 | <0.001** |
| Non-healthcare | 20.2 | 33.0 | 0.0 | |
| Profession in the health system (%) | ||||
| Family doctor | 51.7 | 28.2 | 97.8 | <0.001** |
| Nurse | 13.4 | 27.3 | 1.7 | |
| Nurse's aide | 9.6 | 20.7 | 0.0 | |
| Orderly | 1.7 | 3.7 | 0.0 | |
| Administrative staff | 2.4 | 5.2 | 0.0 | |
| Other | 7.1 | 14.9 | 0.5 | |
| Type of health insurance (%) | ||||
| Public | 83.1 | 75.3 | 94.9 | <0.001** |
| Private | 4.2 | 6.9 | 0.2 | |
| Both of them | 12.6 | 17.8 | 4.8 | |
SD: standard deviation; SAS: Andalusian Health Service; semFYC: Spanish Society of Family and Community Medicine.
A total of 209 positive cases (20.1%) and 829 negative cases (79.9%) were recruited. The group of SAS participants had a significantly higher prevalence of SARS-CoV-2 infection (26.0%) than those participating through the semFYC (11.4%; p < 0.001).
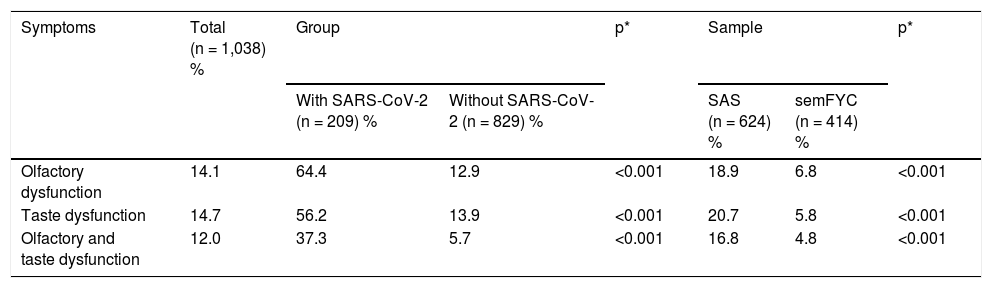
As can be seen in Table 2, OD and TD were present in 14.1% (95% CI 11.9–16.2%) and 14.7% (95% CI 12.0–16.3%) of all study subjects, respectively. 12.0% of the patients (95% CI 10.1–14.2) reported having OD and TD simultaneously. OD and TD were the onset symptoms of the clinical condition in 2.1% and 1.1% of cases, respectively. Both the frequency of OD and TD was higher in the group with COVID-19 than in the controls, with a crude OR of 12.2 (95% CI 8.2–18.6) in the case of OD, and a crude OR of 7.9 (95% CI 5.5–11.5) in TD, as well as with the presence of both abnormalities jointly (OR 9.90; 95% CI 6.6–14.9).
Frequency of olfactory and taste abnormalities according to the study group and the type of sample.
| Symptoms | Total (n = 1,038) % | Group | p* | Sample | p* | ||
|---|---|---|---|---|---|---|---|
| With SARS-CoV-2 (n = 209) % | Without SARS-CoV-2 (n = 829) % | SAS (n = 624) % | semFYC (n = 414) % | ||||
| Olfactory dysfunction | 14.1 | 64.4 | 12.9 | <0.001 | 18.9 | 6.8 | <0.001 |
| Taste dysfunction | 14.7 | 56.2 | 13.9 | <0.001 | 20.7 | 5.8 | <0.001 |
| Olfactory and taste dysfunction | 12.0 | 37.3 | 5.7 | <0.001 | 16.8 | 4.8 | <0.001 |
SAS: Andalusian Health Service; semFYC: Spanish Society of Family and Community Medicine.
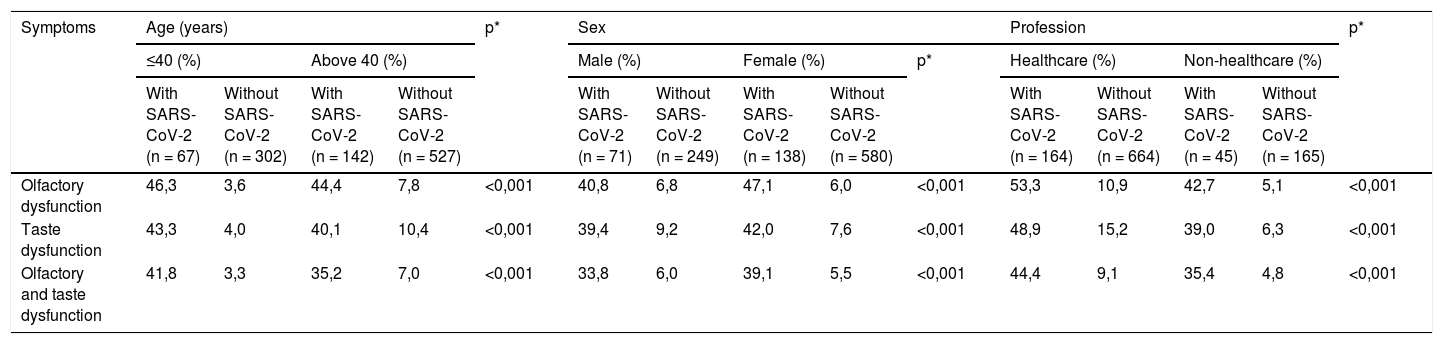
Table 3 shows the frequencies of OD and TD, according to age, sex, and profession in each of the groups compared. Statistically significant differences were observed in the proportions of OD and TD with respect to age (p = 0.001; higher frequency in patients aged 40 or younger), gender (p = 0.001; higher frequency in women) and profession (p = 0.001; higher frequency in healthcare professionals).
Frequency of olfactory and taste abnormalities according to age, sex, and profession in each of the groups.
| Symptoms | Age (years) | p* | Sex | Profession | p* | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤40 (%) | Above 40 (%) | Male (%) | Female (%) | p* | Healthcare (%) | Non-healthcare (%) | |||||||||
| With SARS-CoV-2 (n = 67) | Without SARS-CoV-2 (n = 302) | With SARS-CoV-2 (n = 142) | Without SARS-CoV-2 (n = 527) | With SARS-CoV-2 (n = 71) | Without SARS-CoV-2 (n = 249) | With SARS-CoV-2 (n = 138) | Without SARS-CoV-2 (n = 580) | With SARS-CoV-2 (n = 164) | Without SARS-CoV-2 (n = 664) | With SARS-CoV-2 (n = 45) | Without SARS-CoV-2 (n = 165) | ||||
| Olfactory dysfunction | 46,3 | 3,6 | 44,4 | 7,8 | <0,001 | 40,8 | 6,8 | 47,1 | 6,0 | <0,001 | 53,3 | 10,9 | 42,7 | 5,1 | <0,001 |
| Taste dysfunction | 43,3 | 4,0 | 40,1 | 10,4 | <0,001 | 39,4 | 9,2 | 42,0 | 7,6 | <0,001 | 48,9 | 15,2 | 39,0 | 6,3 | <0,001 |
| Olfactory and taste dysfunction | 41,8 | 3,3 | 35,2 | 7,0 | <0,001 | 33,8 | 6,0 | 39,1 | 5,5 | <0,001 | 44,4 | 9,1 | 35,4 | 4,8 | <0,001 |
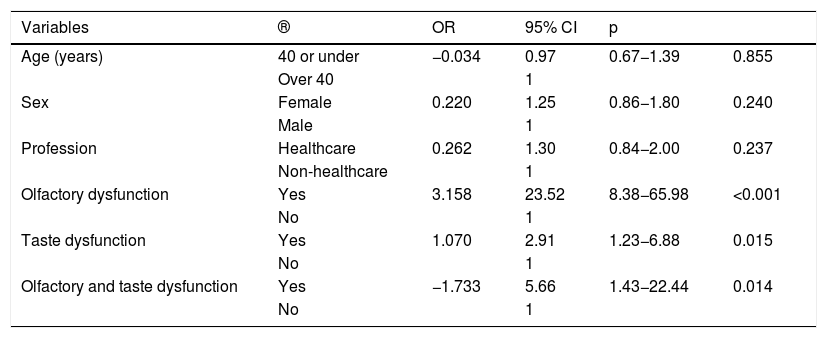
Table 4 shows the results of the binary logistic regression model. Although no statistical significance is observed with regard to age, sex and profession, significant differences are observed with regard to the presence of OD (OR 23.52; 95% CI 8.38−65.98; p = <0.001), TD (OR 2.91; 95% CI 23–6.88; p = 0.015) and both (OR 5.66; 95% CI 1.43–22.44; p = 0.014).
Variables related to the presence of SARS-CoV-2 infection. Binary logistic regression model.
| Variables | ® | OR | 95% CI | p | |
|---|---|---|---|---|---|
| Age (years) | 40 or under | −0.034 | 0.97 | 0.67−1.39 | 0.855 |
| Over 40 | 1 | ||||
| Sex | Female | 0.220 | 1.25 | 0.86−1.80 | 0.240 |
| Male | 1 | ||||
| Profession | Healthcare | 0.262 | 1.30 | 0.84−2.00 | 0.237 |
| Non-healthcare | 1 | ||||
| Olfactory dysfunction | Yes | 3.158 | 23.52 | 8.38−65.98 | <0.001 |
| No | 1 | ||||
| Taste dysfunction | Yes | 1.070 | 2.91 | 1.23−6.88 | 0.015 |
| No | 1 | ||||
| Olfactory and taste dysfunction | Yes | −1.733 | 5.66 | 1.43−22.44 | 0.014 |
| No | 1 |
OR: odds ratio; 95% CI: 95% confidence interval; Hosmer and Lemeshow test 8,770; p = 0.119.
Dependent variable: SARS-CoV-2 infection (Yes/No).
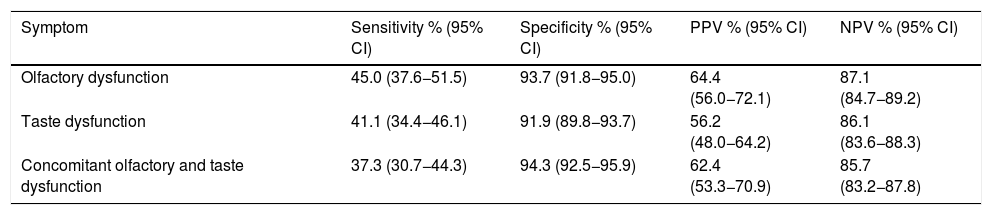
Table 5 shows the results of the criterion validity of the TD and OD, using the result of the PCR as the gold standard. Sensitivity for TD was 41.1% and specificity 96.1%, while for OD sensitivity was 45.0% and specificity 93.7%.
Diagnostic validity of olfactory and taste dysfunction to predict SARS-CoV-2 infection.
| Symptom | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) |
|---|---|---|---|---|
| Olfactory dysfunction | 45.0 (37.6−51.5) | 93.7 (91.8−95.0) | 64.4 (56.0−72.1) | 87.1 (84.7−89.2) |
| Taste dysfunction | 41.1 (34.4−46.1) | 91.9 (89.8−93.7) | 56.2 (48.0−64.2) | 86.1 (83.6−88.3) |
| Concomitant olfactory and taste dysfunction | 37.3 (30.7−44.3) | 94.3 (92.5−95.9) | 62.4 (53.3−70.9) | 85.7 (83.2−87.8) |
95% CI: 95% confidence interval; NPV: negative predictive value; PPV: positive predictive value.
The present study shows the frequency of OD and TD in patients with SARS-CoV-2 infection, as well as the criterion and predictive validity of OD and TD in a sample of Spanish patients recruited through the SAS and the state-wide scientific society semFYC. Our results reveal that more than half of the subjects with SARS-CoV-2 infection show OD or TD. In addition, OD or TD are predictive symptoms of disease in half of the cases, in line with the results obtained in other countries, such as Italy or the USA.
The first clinical records from the Asian continent indicated that the most common symptoms of COVID-19 disease were fever, dry cough, dyspnoea, myalgias, arthralgias, headache, diarrhoea, rhinorrhoea and sore throat.23 Subsequent research has identified an atypical presentation of the disease that includes OD and TD,6,24,25 which seem to be present in patients with mild or moderate symptoms of the disease.
The frequency of OD and TD varies substantially in international series. The European prevalence of OD ranges between 31.6–85.6%, depending on the country: 47% of 114 COVID-19 patients in France,26 31.6% of 79 patients with COVID-19 in Spain,18 and 64.4% of 202 COVID-19 patients in Italy. However, larger-scale research in Europe (conducted in Belgium, France, Spain, and Italy) reveals that 85.6% of 417 mild to moderate COVID-19 patients had OD.6 In the United States, this prevalence was 68% in 59 patients.27 Contrary to previous articles, only 5.1% of 214 patients had OD in China.9 Regarding the prevalence of TD, differences have also been identified in the series, ranging from 35.4% in Spain,18 71% in the US27 and 88.8% in a European study.6 On the other hand, a meta-analysis carried out by Ibekwe et al. reveals that the frequency of OD was 48.5% and 41.5% for TD, and the proportion for both symptoms was 35%.28 Although it is difficult to draw conclusions with the results published internationally, our findings seem to follow the line of studies conducted in Italy or the USA.
Symptoms described as possible early manifestations of COVID-19 disease include OD and TD.16–18 A study carried out in patients with SARS-CoV-2 in Germany showed that the loss of smell presented a sensitivity of 65%, a specificity of 90%, a PPV of 32% and a NPV of 97%, using the RT-PCR test as the gold standard.7 For its part, another study carried out in the United Kingdom showed that the major predictors of disease were OD and TD, with a sensitivity of 65%, a specificity of 85%, a PPV of 47% and a NPV of approximately 90%, using the «SARS-CoV-2 swab test» as the gold standard.19 The results of our study, in comparison with previous articles, show similar sensitivity, specificity and NPV (except that the PPV is lower in the German7 and UK19 studies). These findings indicate that OD and TD symptoms can be considered fairly specific and predictive of COVID-19 disease.
Although the factors associated with the presence of OD and TD are still not totally clear, various studies suggest that age and gender may influence the development of these symptoms.11,17 Several studies have found that women experience OD more often than men.6,17,26 Although various theories have been put forward to try to explain this phenomenon,29 the exact reason for these findings is not yet known. Regarding age, several studies describe the presence of OD and TD in younger patients.11 The findings of this study regarding the age and gender of patients with SARS-Cov-2 infection are consistent with those of the articles published to date.
Among the limitations of the study, it is worth noting a possible selection bias, since 79% of the sample were healthcare professionals. Although this was a highly motivated group, it is to be expected that the health professionals most interested in and aware of COVID-19 disease would be the most likely to participate in the study. In turn, the healthcare population constitutes a population group more exposed to the virus,30 compared to the general population, which could overestimate the true prevalence of SARS-CoV-2 infection. On the other hand, it is necessary to indicate that a significant number of the observational studies reviewed had a small sample size, which limits their generalizability; for this reason, we must be cautious when comparing the results of our study with the findings identified in international series. Another limitation, common to almost all observational studies, is that statistical calculations (such as 95% CIs) are made on the assumption of randomised sampling, which is not the case, so that the uncertainty of the results may be greater than what these intervals reflect.
It would be important to conduct a comparative study of the estimated frequency of OD and TD in patients who have had mild to moderate symptoms and those who have had severe symptoms because, although there is literature suggesting that the frequency of OD and TD is higher in subjects with mild symptoms,31 such an analysis has not been carried out in Spain to date. Another possible limitation of the study lies in the method of reporting the symptoms of SARS-CoV-2 infection. The clinical-epidemiological registry was developed through the self-reporting of sensory symptoms by the participants themselves, without using olfactory or taste tests.
Given the results obtained in our study, there is a need for future research to identify the factors associated with OD and TD, which would provide more information on the early identification of COVID-19 disease. Longitudinal studies assessing the presence and duration of these symptoms, both in patients with mild or moderate clinical conditions and in those with severe conditions, would also be relevant.32
In conclusion, the study shows the high frequency of olfactory and taste dysfunction in patients with SARS-CoV-2 infection identified in PC, demonstrating that more than half of the subjects have these sensory disorders, in line with the findings published to date. Moreover, these symptoms seem to be important disease-specific predictors in the selected Spanish population. For this reason, given the current limitations of population screening for SARS-CoV-2 infection, and the probable recirculation of the virus until an effective vaccine is achieved, OD and TD are symptoms that should be considered when COVID-19 is suspected, as their early detection can help to better guide diagnosis and prompt preventive measures to try to reduce the progression of disease transmission and contribute to curbing the pandemic.
FundingThe study has not received any type of funding.
Conflicts of interestThe authors declare no conflict of interest.
We wish to thank the Board of Directors of the semFYC for endorsing this project and collaborating in the recruitment of participants. The management team of the Córdoba and Guadalquivir Healthcare District, for supporting this study.
Inmaculada Olaya Caro, Sara Ares Blanco, Jaime Barrio Cortes, Francisco Javier Bartolomé Resano, Ana Clavería Fontá, Ana Dosio Revenga, Yolanda González Silva, Jorge Lema Bartolomé, Carmen Martínez Cervell, Bernardino Oliva Fanlo, Santiago Poveda Siles, Raquel Regla Marín, Rubén Villa Estébanez.
Please cite this article as: Pérula de Torres LÁ, González-Lama J, Jiménez García C, Sánchez Montero R, Rider Garrido F, Ortega López Y, et al. Frecuencia de aparición y validez predictiva de la disfunción olfatoria y del gusto en pacientes con infección por SARS-CoV-2. Med Clin (Barc). 2021;156:595–601.
