




On 31st January 2020, the first case of COVID-19 was reported in our country, on the island of La Gomera. On 24th February, the first case on the Spanish mainland was recorded, and subsequently there was an exponential increase in the number of people infected, resulting in the establishment of the state of alarm by the authorities.1
The saturation of the health system, on the verge of collapse in many cases, has led to a restructuring of care processes, as well as a relocation of physical and material resources. Doctors from different specialties have assisted in this crisis, in many cases becoming part of multidisciplinary care units, created to address the number of hospital admissions caused by SARS-CoV-2. Despite the significant impact on the health system, its implications from a care point of view have not yet been studied and may be of interest in the management of eventual outbreaks.
We report the data from our site, which is a county referral hospital in the care of severe heart patients and in interventional cardiology procedures. For this, all the patients admitted to cardiology between 4th March (first case of SARS-CoV-2 in the county was reported) and 19th April 2020, were analyzed, date on which the situation of the center allowed the reorganization of the departments to its usual set-up. An equivalent period prior to the reporting of the first case was considered as control (from 17th January to 3rd March 2020). Scheduled procedures were carried out at the discretion of the corresponding units where the procedure was performed, following the recommendations in force.2–4
During the pandemic, there were a total of 67 cardiology admissions in our center (1.46admissions/day), which meant a 69.9% reduction in the number of admissions compared to the same period prior to the pandemic, when 223 admissions took place (4.4admissions/day).
The mean age of the patients admitted was 66.2±15years, similar in both periods (65.4±15 vs. 68.4±13years; p=0.22). In the pandemic period, a reduction in admissions was detected for all coded aetiologies (Table 1). Those processes related to acute ischemic heart disease decreased by 56.8% overall, showing the greatest decrease in the number of acute ST elevation myocardial infarction (STEMI). Admissions for acute heart failure showed a reduction of 83.6%. It is noteworthy that during the pandemic there was no admission for myocarditis. Regarding emergency arrhythmic pathology, a 60% reduction was observed, more significant in admissions for tachyarrhythmias than for bradyarrhythmias. The number of elective admissions decreased by 85%. The number of procedures performed on admitted patients was reduced by 71.4% (314 vs. 92; p<0.01), although the procedure/patient ratio was similar in both periods (1.41 vs. 1.37; p=0.43).
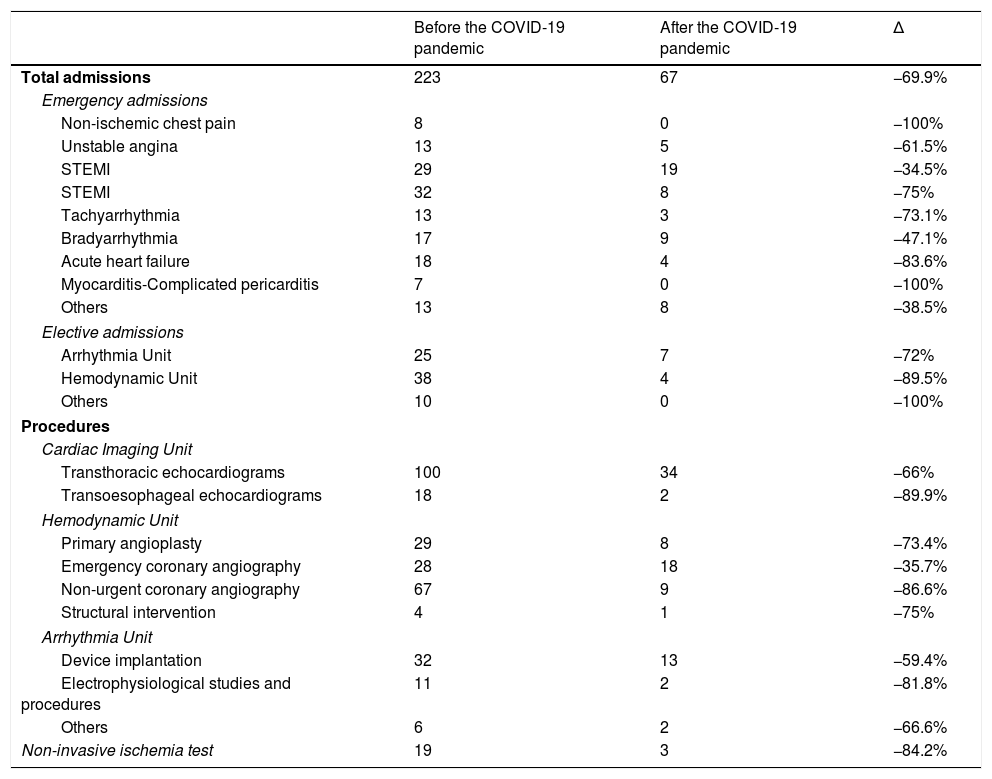
Hospital admissions in the cardiology department and procedures performed.
| Before the COVID-19 pandemic | After the COVID-19 pandemic | Δ | |
|---|---|---|---|
| Total admissions | 223 | 67 | −69.9% |
| Emergency admissions | |||
| Non-ischemic chest pain | 8 | 0 | −100% |
| Unstable angina | 13 | 5 | −61.5% |
| STEMI | 29 | 19 | −34.5% |
| STEMI | 32 | 8 | −75% |
| Tachyarrhythmia | 13 | 3 | −73.1% |
| Bradyarrhythmia | 17 | 9 | −47.1% |
| Acute heart failure | 18 | 4 | −83.6% |
| Myocarditis-Complicated pericarditis | 7 | 0 | −100% |
| Others | 13 | 8 | −38.5% |
| Elective admissions | |||
| Arrhythmia Unit | 25 | 7 | −72% |
| Hemodynamic Unit | 38 | 4 | −89.5% |
| Others | 10 | 0 | −100% |
| Procedures | |||
| Cardiac Imaging Unit | |||
| Transthoracic echocardiograms | 100 | 34 | −66% |
| Transoesophageal echocardiograms | 18 | 2 | −89.9% |
| Hemodynamic Unit | |||
| Primary angioplasty | 29 | 8 | −73.4% |
| Emergency coronary angiography | 28 | 18 | −35.7% |
| Non-urgent coronary angiography | 67 | 9 | −86.6% |
| Structural intervention | 4 | 1 | −75% |
| Arrhythmia Unit | |||
| Device implantation | 32 | 13 | −59.4% |
| Electrophysiological studies and procedures | 11 | 2 | −81.8% |
| Others | 6 | 2 | −66.6% |
| Non-invasive ischemia test | 19 | 3 | −84.2% |
STEMI: acute myocardial infarction with ST-segment elevation; STEMI: ST elevation myocardial infarction.
These data show a significant reduction in hospital admissions in the cardiology department. This trend, expected in elective procedures, is difficult to address in relation to emergency pathology. Although the implementation of teleconsultation could have prevented a certain number of admissions by optimizing medical treatment and limiting emergency care only in those most necessary cases, a significant number of patients may have delayed or omitted contact with healthcare.
A recent study estimates a 40% reduction in the number of emergency revascularizations performed in the context of STEMI in a multicenter cohort in our country after the start of the pandemic. The authors of the study pay attention to the multifactorial origin of this reduction, emphasizing the delay or absence of demand for emergency care, although they point to a probable underdiagnosis of acute cardiovascular disease at a time when the majority of resources were devoted to the detection of infection and its complications.5 Our data confirm the trend observed in said study for our autonomous community. Unfortunately, we do not have similar data related to other medical specialties that allow us to make comparative references.
Please cite this article as: Negreira Caamaño M, Piqueras Flores J, Mateo Gómez C. Impacto de la pandemia COVID-19 sobre los ingresos hospitalarios en cardiología. Med Clin (Barc). 2020;155:179–180.
