




SARS-CoV-2 infection is clinically very heterogeneous, varying from asymptomatic to severe clinical conditions with a fatal outcome. Some studies suggests that the ABO blood group could be a biological marker of susceptibility for the development of the disease.
Material and methodsWe collected data from patients admitted with COVID-19 infection who had ABO blood group recorded, and analyzed the incidence by groups, compared with the global population in Navarre, as well as their main complications and evolution.
ResultsGroup O was proportionally less represented in the hospitalized patients with respect to the global population, although the difference was not statistically significant. Group B had significantly higher rates of thrombotic complications and required more admissions in intensive care units.
ConclusionThe study suggests a lower susceptibility to infection in group O and a higher risk of complications in group B. Studies with a larger sample size are required in order to obtain significant results.
La infección por SARS-CoV-2, presenta gran heterogeneidad clínica, desde asintomática hasta cuadros clínicos graves con un desenlace fatal. Algunos autores refieren el grupo sanguíneo ABO como posible marcador biológico de susceptibilidad para la enfermedad.
Pacientes y métodosSe han recogido los pacientes ingresados con infección por COVID-19 y se ha analizado la incidencia por grupos en relación con la base poblacional de la Comunidad Foral de Navarra, así como sus principales complicaciones y evolución.
ResultadosLos pacientes de grupo O ingresados con infección por COVID-19 son proporcionalmente menos respecto a la base poblacional sin ser la diferencia estadísticamente significativa. Los grupos AB y B son un 38% más en el grupo de infectados que en la población. El grupo B ha presentado significación estadística en cuanto al número de complicaciones trombóticas junto con mayor tasa de ingreso en unidades de cuidados intensivos.
ConclusiónEl estudio sugiere menor susceptibilidad a la infección de los pacientes de grupos O y mayor riesgo de complicaciones en el grupo B. Hacen falta estudios con mayor tamaño muestral para poder obtener resultados significativos.
SARS-CoV-2 infection generally causes mild symptoms (80%), although mortality increases (50%) in patients who require admission to Intensive Care Units (ICU) with invasive mechanical ventilation.1 Older age, male gender, and certain chronic diseases predispose to increased risk of infection and severity, and thromboembolic events.
Some authors point to the ABO blood group as a possible biological marker of susceptibility to COVID-19, suggesting that group O people have a lower probability of infection.2
ABO antigenic determinants are also expressed in cells of certain endothelial and epithelial tissues such as the respiratory system. The presence of A and B antigens is associated with greater susceptibility to infections, cardiovascular diseases, and cancer, while group O is usually associated with greater resistance to diseases.3
COVID-19 patients often have thrombotic complications, even when using prophylaxis.4 Von Willebrand factor (VWF) is a glycoprotein linked to haemostasis whose plasma levels are influenced by various factors, including ABO loci, which determine approximately 30% of its total plasma levels.5 Group O patients have lower levels of VWF, which may contribute to fewer thrombotic complications in COVID-19 affected O patients.
Our objective is to describe the distribution of the COVID-19 disease and its complications by blood groups in the population of Navarra and to try to determine a possible relationship with the ABO group.
Patients and methodsWe analysed patients with COVID-19 (PCR positive nasopharyngeal swab) and previously recorded blood group, admitted to 2 public hospitals during the first half of April 2020.
We reviewed demographic data, laboratory parameters and clinical data, including infectious and thrombotic complications.
Population ABO blood group distribution data was extracted from the donor and transfusion management application e-Delphyn BB version 8.0.17.2 (Hemasoft®, Valladolid, Spain). A common and unique database for transfusion centres and services in the Navarra public network, which allows us to have a representative sample of our population.
Analytical data were reviewed using the Cobas program® Infinity IT solutions version 2.5.3.3596 (Roche Diagnostics [Schweiz] AG Industriestrasse 7 CH-6343 Rotkreuz) and the clinical data were collected from the Computerized Medical Record application (Property of the Navarra Health Service-Osansunbidea). The database has been anonymized in compliance with the data protection laws.
To compare the distribution by blood groups, we show frequencies and percentages of each blood group in the general population and in patients with COVID-19, calculating the relative risks of belonging to each group and the chi-square test for goodness of fit. Demographic and clinical data are described by frequencies and percentages for categorical variables and using mean and standard deviation or median and interquartile range for quantitative variables. Quantitative variables were compared by blood group using the Anova test or Kruskal-Wallis test and categorical variables using Fisher's test. To study differences in complications by group, multivariate logistic models were estimated, adjusting for sex and age, and to study the analytical evolution, linear models were used, adjusting for sex, age, and blood group. The comparisons were two-tailed assuming a significance level of 0.05. The analysis was performed with IBM SPSS v. 25.0 and R v.3.4.3 software. (SNS-O License).
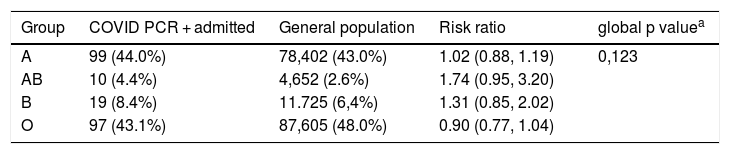
ResultsWe analysed 226 patients with a mean age of 70.9 years, of which 17.9% were admitted to the ICU and 16.3% died. The chi-square test for goodness of fit does not show significant differences in our community for the distribution of the ABO group in the population with COVID versus the general population (Table 1). We observed a higher percentage of groups AB and B in patients, but the effect is not significant, and these are groups with few cases. Pooling groups AB and B, the global p value of goodness of fit is still not significant, but the risk ratio or relative risk of the combined group AB + B is on the verge of significance, there is 38% more presence of these groups in COVID patients than in the general population.
Population vs. COVID-19 patients blood group distribution comparison.
| Group | COVID PCR + admitted | General population | Risk ratio | global p valuea |
|---|---|---|---|---|
| A | 99 (44.0%) | 78,402 (43.0%) | 1.02 (0.88, 1.19) | 0,123 |
| AB | 10 (4.4%) | 4,652 (2.6%) | 1.74 (0.95, 3.20) | |
| B | 19 (8.4%) | 11.725 (6,4%) | 1.31 (0.85, 2.02) | |
| O | 97 (43.1%) | 87,605 (48.0%) | 0.90 (0.77, 1.04) |
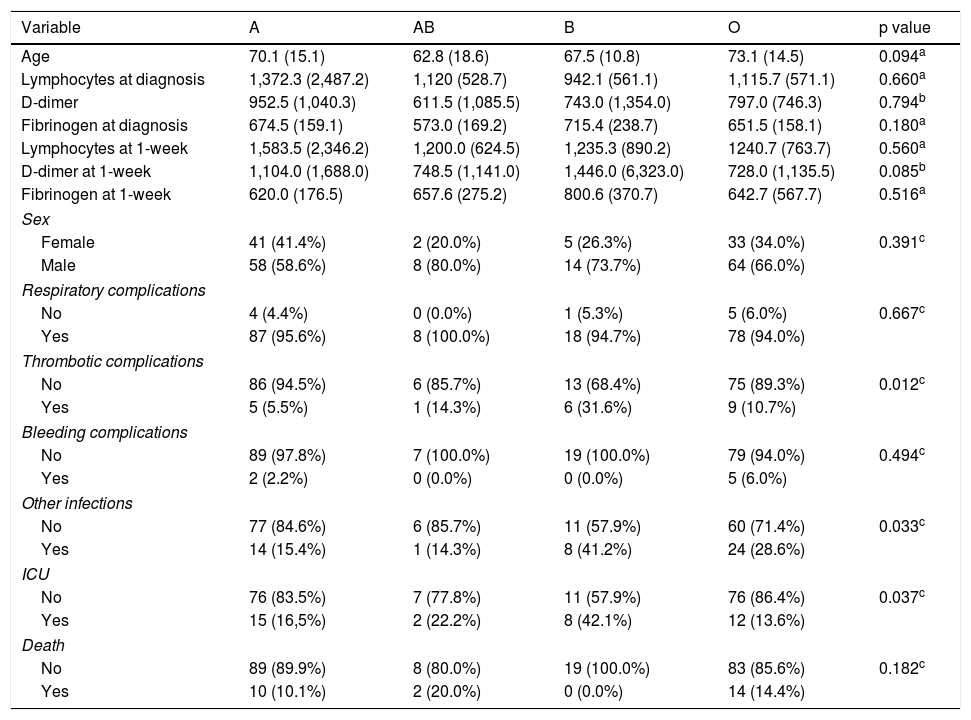
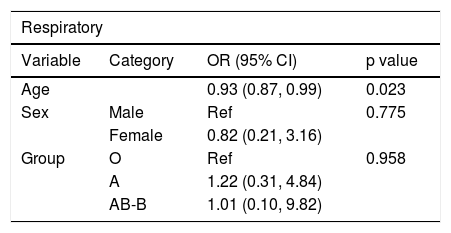
There are no significant differences in distribution by sex, age, or blood group. Both respiratory complications and deaths increase with age, but without significant differences by blood group. There is more risk of developing other infections in patients admitted to the ICU and in groups AB-B (Tables 2 and 3).
Comparisons of variables by group.
| Variable | A | AB | B | O | p value |
|---|---|---|---|---|---|
| Age | 70.1 (15.1) | 62.8 (18.6) | 67.5 (10.8) | 73.1 (14.5) | 0.094a |
| Lymphocytes at diagnosis | 1,372.3 (2,487.2) | 1,120 (528.7) | 942.1 (561.1) | 1,115.7 (571.1) | 0.660a |
| D-dimer | 952.5 (1,040.3) | 611.5 (1,085.5) | 743.0 (1,354.0) | 797.0 (746.3) | 0.794b |
| Fibrinogen at diagnosis | 674.5 (159.1) | 573.0 (169.2) | 715.4 (238.7) | 651.5 (158.1) | 0.180a |
| Lymphocytes at 1-week | 1,583.5 (2,346.2) | 1,200.0 (624.5) | 1,235.3 (890.2) | 1240.7 (763.7) | 0.560a |
| D-dimer at 1-week | 1,104.0 (1,688.0) | 748.5 (1,141.0) | 1,446.0 (6,323.0) | 728.0 (1,135.5) | 0.085b |
| Fibrinogen at 1-week | 620.0 (176.5) | 657.6 (275.2) | 800.6 (370.7) | 642.7 (567.7) | 0.516a |
| Sex | |||||
| Female | 41 (41.4%) | 2 (20.0%) | 5 (26.3%) | 33 (34.0%) | 0.391c |
| Male | 58 (58.6%) | 8 (80.0%) | 14 (73.7%) | 64 (66.0%) | |
| Respiratory complications | |||||
| No | 4 (4.4%) | 0 (0.0%) | 1 (5.3%) | 5 (6.0%) | 0.667c |
| Yes | 87 (95.6%) | 8 (100.0%) | 18 (94.7%) | 78 (94.0%) | |
| Thrombotic complications | |||||
| No | 86 (94.5%) | 6 (85.7%) | 13 (68.4%) | 75 (89.3%) | 0.012c |
| Yes | 5 (5.5%) | 1 (14.3%) | 6 (31.6%) | 9 (10.7%) | |
| Bleeding complications | |||||
| No | 89 (97.8%) | 7 (100.0%) | 19 (100.0%) | 79 (94.0%) | 0.494c |
| Yes | 2 (2.2%) | 0 (0.0%) | 0 (0.0%) | 5 (6.0%) | |
| Other infections | |||||
| No | 77 (84.6%) | 6 (85.7%) | 11 (57.9%) | 60 (71.4%) | 0.033c |
| Yes | 14 (15.4%) | 1 (14.3%) | 8 (41.2%) | 24 (28.6%) | |
| ICU | |||||
| No | 76 (83.5%) | 7 (77.8%) | 11 (57.9%) | 76 (86.4%) | 0.037c |
| Yes | 15 (16,5%) | 2 (22.2%) | 8 (42.1%) | 12 (13.6%) | |
| Death | |||||
| No | 89 (89.9%) | 8 (80.0%) | 19 (100.0%) | 83 (85.6%) | 0.182c |
| Yes | 10 (10.1%) | 2 (20.0%) | 0 (0.0%) | 14 (14.4%) | |
Complications by groups.
| Respiratory | |||
|---|---|---|---|
| Variable | Category | OR (95% CI) | p value |
| Age | 0.93 (0.87, 0.99) | 0.023 | |
| Sex | Male | Ref | 0.775 |
| Female | 0.82 (0.21, 3.16) | ||
| Group | O | Ref | 0.958 |
| A | 1.22 (0.31, 4.84) | ||
| AB-B | 1.01 (0.10, 9.82) | ||
| Thrombotic | |||
|---|---|---|---|
| Variable | Category | OR (95% CI) | p value |
| Age | 0.99 (0.96, 1.02) | 0.627 | |
| Sex | Male | Ref | 0.970 |
| Female | 0.98 (0.36, 2.65) | ||
| Group | A | Ref | 0.017 |
| AB-B | 6.16 (1.75, 21.8) | ||
| O | 2.09 (0.67, 6.54) | ||
| Other infections | |||
|---|---|---|---|
| Variable | Category | OR (95% CI) | p value |
| Age | 0.99 (0.97, 1.01) | 0.254 | |
| Sex | Male | Ref | 0.114 |
| Female | 1.74 (0.88, 3.48) | ||
| Group | A | Ref | 0.035 |
| AB-B | 3.05 (1.11, 8.39) | ||
| O | 2.36 (1.11, 5.01) | ||
Ref: reference; OR: odds ratio; CI: confidence interval.
We observed a statistically significant association between thrombotic complications and admission to the ICU with blood group. Group B developed more thrombosis (28.6%) with an OR of 6.16 (1.75, 21.8) and required more admission to the ICU (38.1%), with group O being the least admitted in the ICU. D-dimer increases more in group A compared to O (significant difference; beta = 2392.7) and fibrinogen increased significantly more in groups AB-B than in O (Appendix B annex, supplementary table). No differences were found in bleeding complications, though this is of little significance due to the small sample size.
DiscussionIn our population, the least prevalent group among hospitalised COVID-19 patients and with the lowest incidence of ICU admission is O, observing a higher incidence of SARS-CoV-2 infection among groups AB and B.
The inheritance of ABH antigens is associated with a predisposition to certain diseases or the risk of infections.3 There are studies that link group B with severe asthma,6 while natural anti-A antibodies have been described as protective against certain infections. Group O has also been assigned a protective role against malaria, while group B is associated with a higher risk of severe malaria infection.
The relationship of the ABO groups was studied for other coronaviruses with findings similar to those found for SARS-CoV-2, finding lower rates of infection in group O.7 SARS-CoV-2 replicates in respiratory and digestive epithelial cells with the ability to synthesize ABH carbohydrate epitopes, so virion S protein could bind to carbohydrate epitopes A or B.
Coronaviruses are RNA viruses whose binding domain bears important similarities to the angiotensin-converting enzyme 2 (ACE2) receptor. Natural anti-A or anti-B antibodies could bind to viral S protein and block its interaction with ACE2, providing protection by blocking the interaction between the virus and its receptor. A 2008 mathematical model on the dynamics of virus transmission indicated that the ABO polymorphism could contribute to substantially reduce viral transmission, affecting both the number of infected individuals and the kinetics of the epidemic.8
Another interesting fact observed is the higher percentage of thrombotic complications diagnosed in group B (28.6%), also coinciding with a higher proportion of admission to the ICU (38.1%). The evolutionary analysis of D-dimer in these patients shows a greater increase one week after admission in group A and a greater increase in fibrinogen in groups AB and B compared to group O. Subjects in group O have a VIII factor and VWF titre lower than average, which could justify it.9 The deceased COVID-19 patients had significantly higher levels of D-dimer and 71.4% of the deceased met the criteria for disseminated intravascular coagulation compared to 0.6% of those who survived the infection.6 If the relationship of the ABO group with D-dimer levels is confirmed with larger studies, the ABO group could also be used as a risk factor in a similar way to what the study by Zhou et al. suggests, which concludes that a value of D-dimer greater than 1 μg/l would allow the identification of patients with a worse prognosis in early stages.10
We conclude that there may be a relationship between blood group and predisposition to COVID-19 and its complications, with a lower incidence in group O and a worse progression of group B patients. However, we consider that this is a study of modest size on a population located in a limited geographical area, which calls for multicentre, larger sample size studies.
EthicsNo animal testing has been carried out. The Declaration of Helsinki was observed.
An informed consent exemption has been requested for the collection of retrospective data from patients who are still alive, have died or have been lost to follow-up. The authors justify this procedure based on 2 principles: the first one is that at the time of data collection for this study, several patients had died. The second is that the investigators consider that, even though an effort may be made to locate living patients, contacting them or the relatives of already deceased patients entails an unnecessary emotional burden and they do not consider it justified, since the study is based on the retrospective observational collection of data already available and has no therapeutic or prognostic implications for patients.
FundingNone for this job.
Conflict of interestsNone for this study. The authors have carried out this study under their own initiative, with no economic pressure.
We wish to thank the Hemasoft IT Support Team® for data exploitation, the laboratory technician Mrs. Blanca Apesteguia and to Dr. D. José Manuel Sánchez, from the Haematology and Hemotherapy Department for their collaboration in data collection.
The following is Supplementary data to this article:
Please cite this article as: Zalba Marcos S, Antelo ML, Galbete A, Etayo M, Ongay E, García-Erce JA. Infección y trombosis asociada a la COVID-19: posible papel del grupo sanguíneo ABO. Med Clin (Barc). 2020;155:340–343.
