




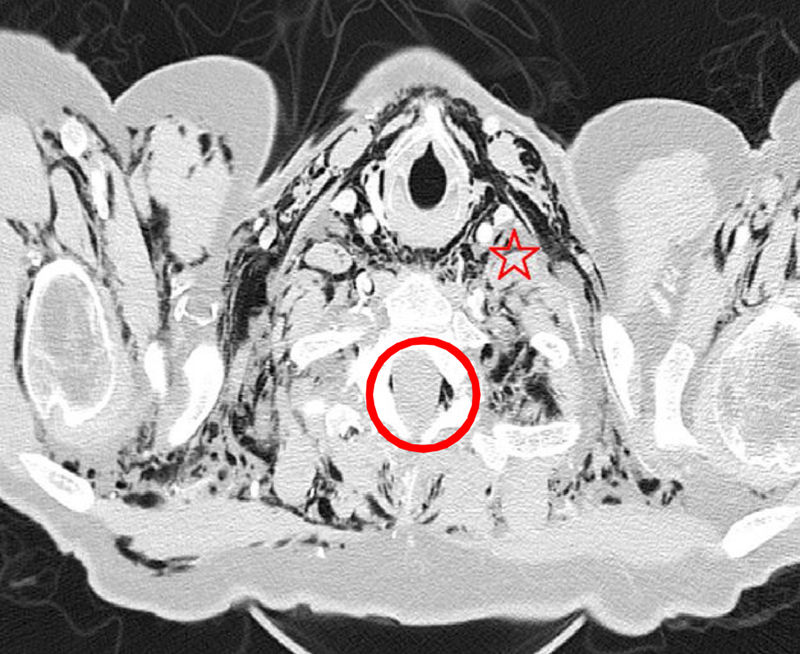
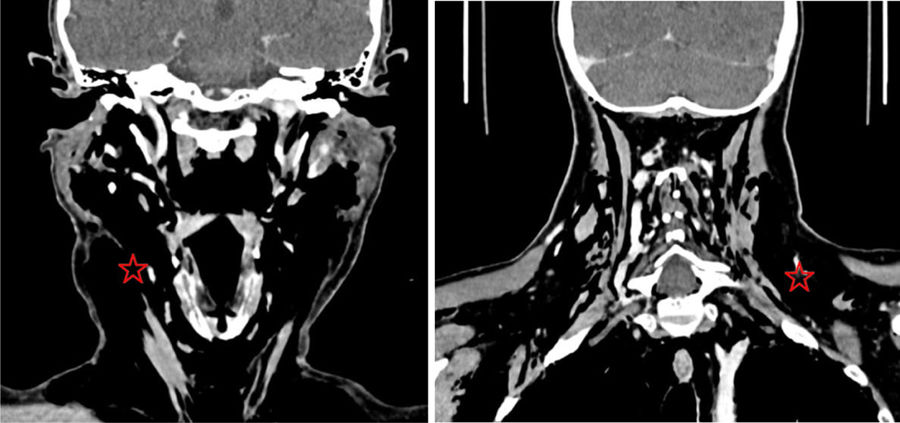
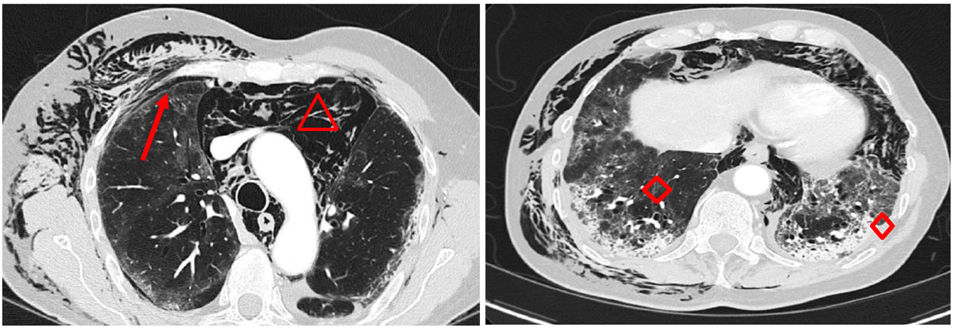
Male, 61, previously admitted to ICU for COVID pneumonia without invasive procedures (intubation or mechanical ventilation), managed with high-flow oxygen therapy and transferred to ward. A few days later, a subcutaneous emphysema was observed without initial clinical impact, but with subsequent progression. A neck soft tissue CT and a chest CT were performed, showing facial-cervical subcutaneous emphysema dissecting muscle planes with air content in the retropharyngeal space, with no decrease in calibre or airway compromise (Fig. 1: Axial CT section and Fig. 2: Coronal CT section, marked with red stars). Significant pneumomediastinum that extended from the cervical region (Fig. 3: Axial CT section, marked with red triangles), causing posterior displacement of the cardiovascular structures and the lung parenchyma, mainly on the left. Presence of right pneumothorax predominantly in the apex (Fig. 3, marked with a red arrow). Subcutaneous emphysema that dissected thoracic and abdominal muscle planes, predominantly on the right side, with air content in the spinal canal (Fig. 1, marked with a red circle). Opacities and ground glass areas with traction bronchiectasis were observed in the lung parenchyma (Fig. 3: Axial CT scan, marked with red diamonds). After a good clinical course with conservative treatment, the patient was discharged from the hospital.



Please cite this article as: Orera Pérez Á, Barber Ansón M, Erice Azparren E. Neumomediastino y enfisema subcutáneo en COVID-19 en ventilación espontánea. Med Clin (Barc). 2022;158:400.
