



Cerebral hemiatrophy or Dyke-Davidoff-Masson syndrome is a rare condition first described in 1933, with characteristic clinical and radiological features such as facial asymmetry, hemiplegia, seizures, mental retardation, cerebral hemiatrophy, and skull and frontal sinus abnormalities. We describe the clinical features, brain imaging and clinical course of a 13 year-old patient with this syndrome.
Introduction
Cerebral hemiatrophy or Dyke-Davidoff-Masson syndrome (DDMS) is a rare condition, which may be congenital or develop in early childhood. In 1933, Dyke, Davidoff and Masson first described the syndrome in a series of 9 patients with hemiplegia and cranial asymmetry in plain cranial X-rays. However, since then there have been few pediatric cases reported.1-3 The syndrome is characterized by facial asymmetry, seizures, hemiplegia or contralateral hemiparesis, and mental retardation of variable severity.1,3,4 it occurs in both genders, with a predominance in males (73.5%).5 A diagnosis is usually made during late childhood, adolescence or adulthood.6 The etiology can be congenital or acquired as a result of an alteration in the cerebral perfusion during prenatal, perinatal or early childhood periods.1,4,5,7,8 The brain scan (CT) or magnetic resonance imaging (MRI) is utilized to perform a diagnosis and specific findings include unilateral brain volume loss and compensatory bone alteration resulting in cerebral hemiatrophy, usually on the left hemisphere (69%). In addition, ipsilateral cranial hypertrophy, overdevelopment of the orbital roof and hyperpneumatisation of frontal sinuses may occur.4,5,7,9,10
Case presentation
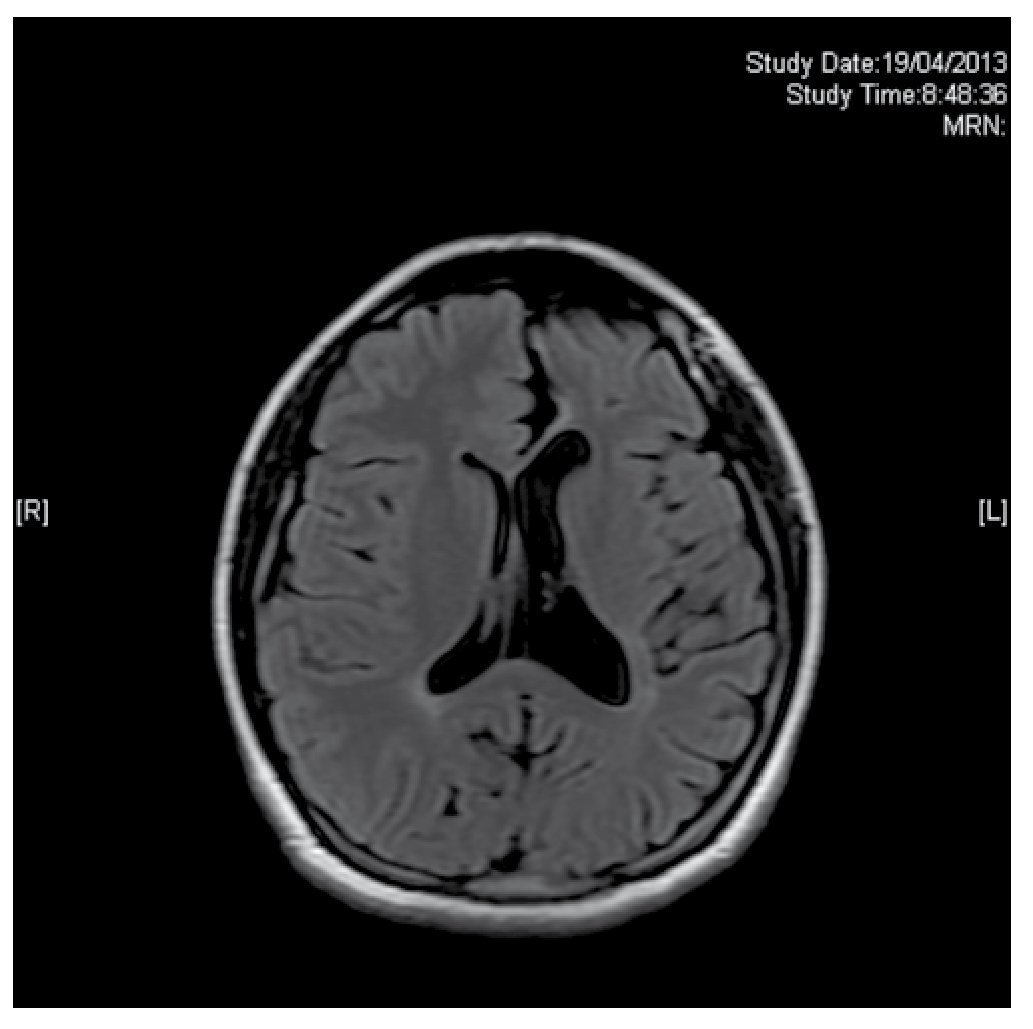
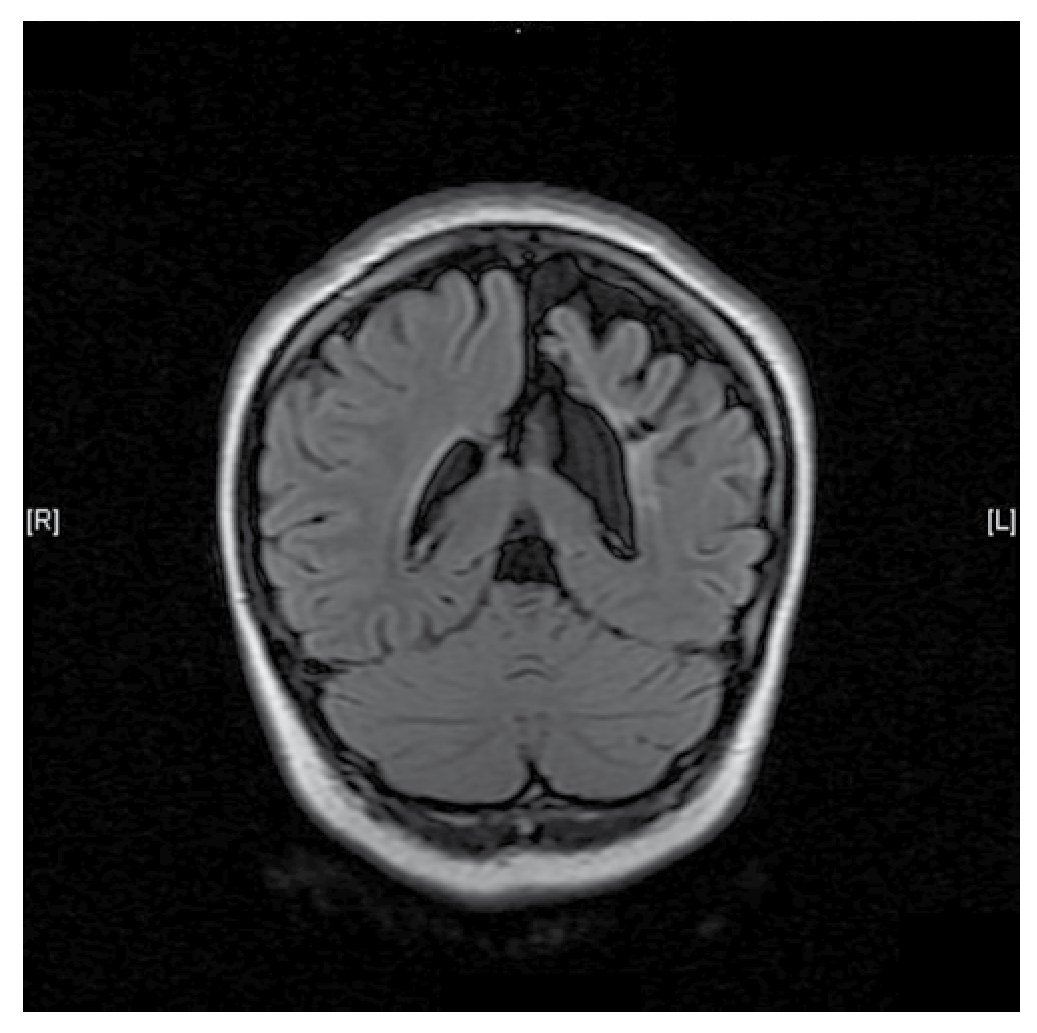
A 13-year-old female, product of a fourth pregnancy, with a history of a monozygotic twin pregnancy, full term with adequate weight and no contingencies, normal psychomotor development up to the first year of age, when a gait alteration with right hemibody weakness was noticed. She was admitted to the Pediatric Neurology Service at "Dr. José Eleuterio González" University Hospital after presenting simple partial seizure with motor symptoms at age 7. An electroencephalogram (EEG) was performed with normal results, and the patient was controlled with 400 mg/day of oral carbamazepine. During the physical exam the patient displayed hemifacial atrophy of the right side causing asymmetry (Fig. 1), right spastic hemiparesis with atrophy, hyperreflexia, ipsilateral extensor plantar response and a hemiplegic gait. We are able to observe in the brain MRI a reduction of ridges and grooves in the left frontoparietal region, associated with ectasia of the ipsilateral ventricle, which is compatible with cerebral hemiatrophy of the left frontoparietal lobe (Figs. 2 and 3). The patient is currently stable with proper control of seizure crisis and an adequate level of antiepileptic medication (9.0 µg/dl). She is attending our integral follow-up service and rehabilitation.

Figure 1 A 13-year-old female in whom facial asymmetry is observed.
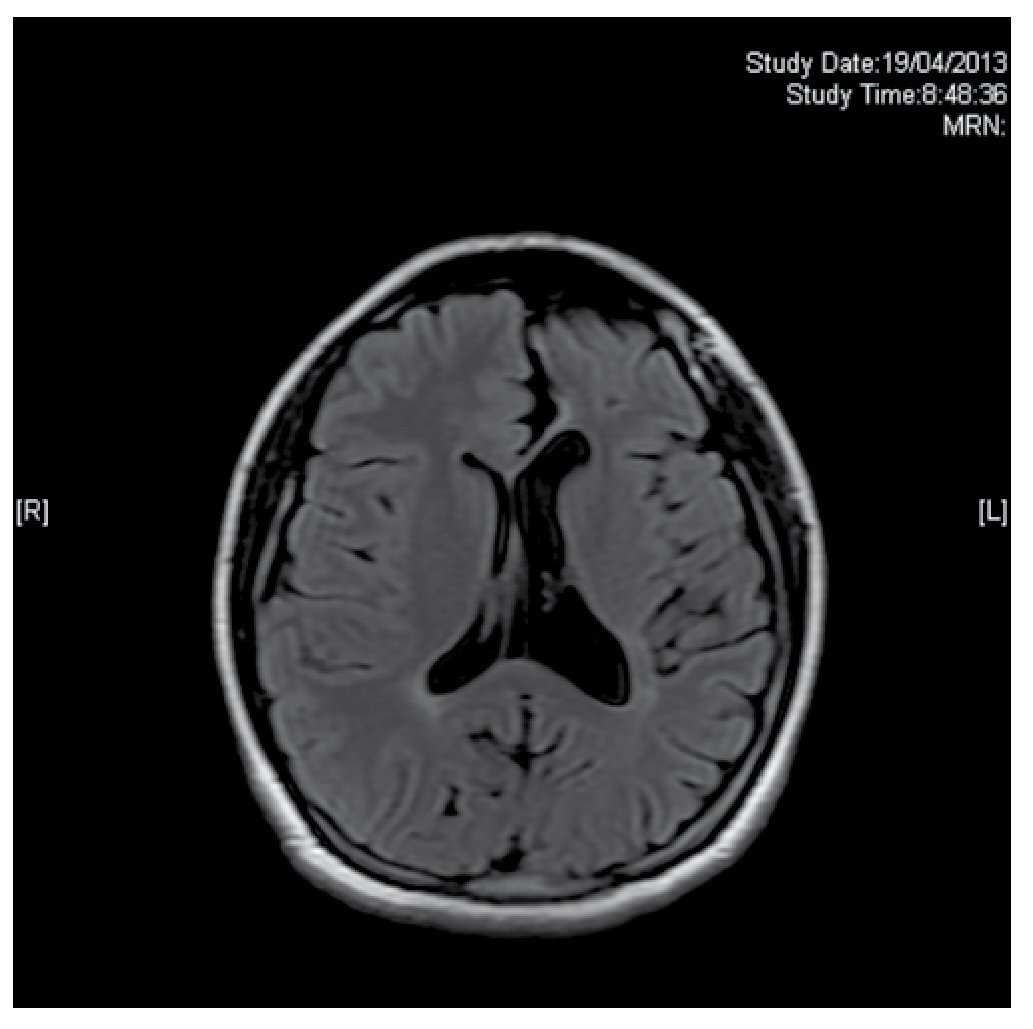
Figure 2 Axial magnetic resonance imaging (MRI), T2 FLAIR sequence which shows left frontoparietal atrophy with ipsilateral ventriculomegaly.
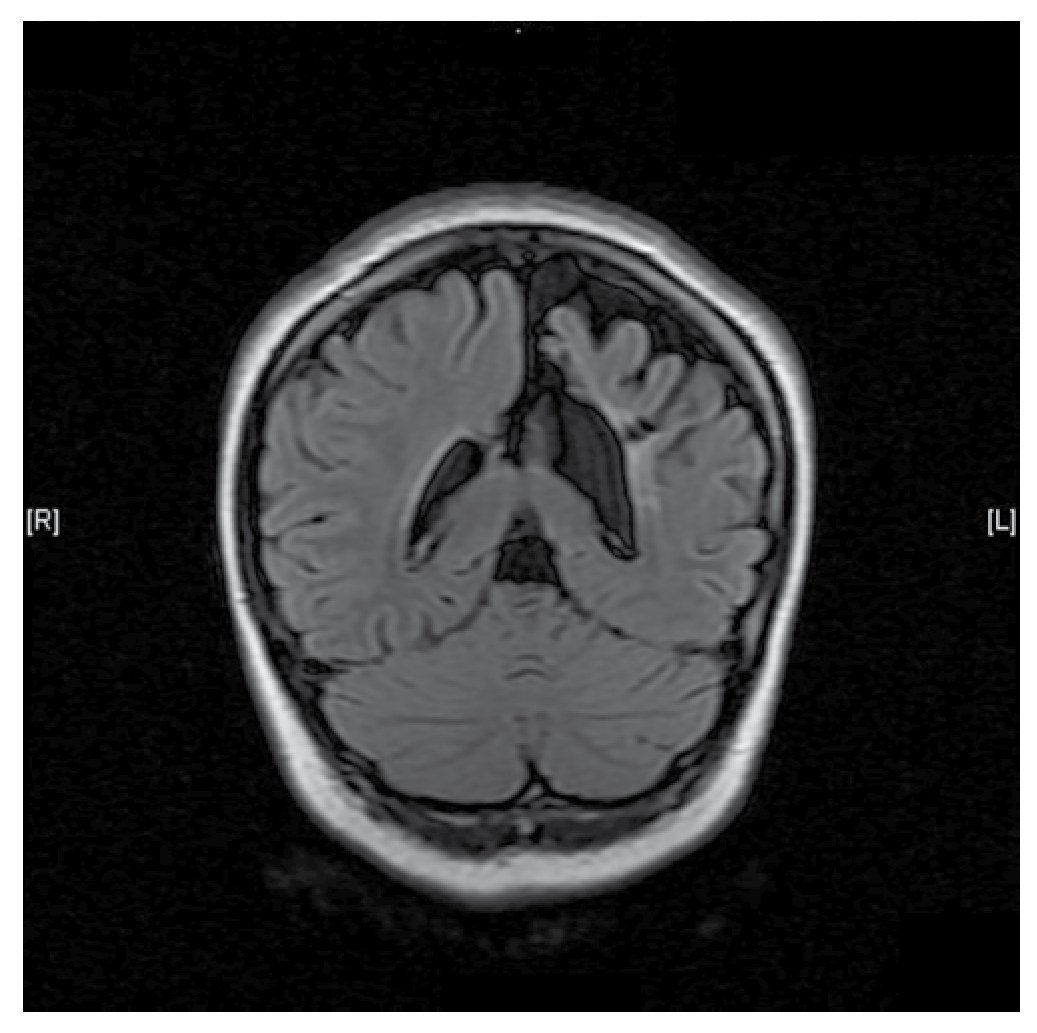
Figure 3 Coronal magnetic resonance imaging (MRI), T2 FLAIR sequence which shows interhemispheric asymmetry with atrophy and left ventricular ectasia.
Discussion
Cerebral hemiatrophy or DDMS is an entity characterized by seizures, hemiplegia or hemiparesis and mental retardation.1,4,5,9 The condition may be congenital or acquired. In the congenital form, there are usually no evident etiological factors and symptoms present at birth or shortly after. Cerebral damage is likely due to an intrauterine vascular occlusion during the prenatal period. In the acquired form, symptoms are related to a damage of the central nervous system occurring around or after the perinatal period. Some of the etiological factors include trauma, infection, vascular anomalies, hemorrhagic and ischemic conditions, amniotic bands, and an intraventricular and subependymal germinal matrix.5,8,10 The mechanism of cerebral atrophy remains unknown.1 Our patient displayed symptoms during an early stage of her development; moreover, because of the history of being a product of a twin pregnancy, a high risk state during pregnancy and the lack of evidence of injury during postpartum, most likely the damage occurred during the prenatal stage. Seizures do not always appear during early childhood and often begin months or years after the hemiparesis onset.3,4 Sometimes patients display refractory epilepsy, and the treatment must focus on seizure control with anticolvulsant medication being either mono or polytherapy.5 Children with refractory epilepsy and hemiplegia are potential candidates for hemispherectomy, with a success rate of 85%. Vagal stimulation is another alternative. There is evidence that 30%-50% of patients with partial epilepsy may experience a decrease in convulsions in over 50% of the cases.3 The prognosis is better if the hemiparesis appears after the first 2 years of age and in absence of recurrent and prolonged epilepsy. This syndrome is a rare condition, with few cases described in medical literature and limited experience in pediatric patients. It is important to keep it in mind when dealing with a patient with facial asymmetry associated with neurologic hemiplegia data, seizures, and mental retardation, in order to perform a correct diagnosis and proper care. Even though an established protocol for management is lacking, there is the indication for therapy including anticonvulsants and surgery in specific cases. In addition, physical therapy, occupational therapy and language therapy play significant roles in the long term management of the patients.5
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
No financial support was provided.
Received: July 2013;
Accepted: January 2014
* Corresponding author:
Service of Pediatric Neurology, Department of Neurology,
"Dr. José Eleuterio González" University Hospital, Faculty of Medicine,
Universidad Autónoma de Nuevo León, Monterrey, N. L., Mexico.
Telephone: (044) 818 016 9944.
E-mail address: kazaamba@hotmail.com (M. A. Duncan).