





External ophthalmomyiasis is an infestation of conjunctiva with larvae or maggots of certain flies. Oestrus ovis is the most common cause of human ophthalmomyiasis. The case of a 16-year-old female is described, who presented with foreign body sensation, pain, and redness in the left eye. Slit-lamp biomicroscopy revealed 32 tiny larvae crawling around the conjunctival sac. The larvae were mechanically removed under topical anesthesia, and identified under a light microscope as first-stage larvae of O. ovis causing external ophthalmomyiasis. She was successfully treated with topical tobacco juice.
Follow-up examination of these cases is recommended to avoid possible complications.
Introduction
Infestation with larvae (maggots) on human and animal tissues and organs is known as myiasis. The most common site of infection is damaged skin, however; there are other less common places like the throat, nose, nostrils, eyes and urogenital tract. The infection of the eye caused by larvae is known as ophthalmomyiasis.1 We present an external ophthalmomyiasis case by Oestrus ovis diagnosed and treated in a hospital in Monterrey, Mexico.
Clinical case
Female patient, 16 years old, without any significant medical or ophthalmological history. The patient went to the ophthalmology department in a private hospital in Monterrey, Mexico, 3 h after suffering an impact in the left eye caused by a flying insect. The patient was at school at the time of the accident and presented a sensation of a foreign body, redness, epiphora and burning in her left eye. Upon examination, the eyelids were found to be normal, the conjunctive was congested and the patient retained eye movement. In the biomicroscopy we observed transparent larvae moving over the bulbar conjunctive from the inferior towards the superior formix, as well as on the cornea. The larvae displayed a photophobic behavior since they moved away from the light from the slit lamp, thus impeding photography (figure 1). We applied an anesthetic chloridium (tetracaine) in order to perform their extraction with a swab, but it was difficult since they were strongly attached. We used tweezers to remove the 32 larvae; they were submitted to the microbiology department. We prescribed antibiotic therapy and anti-inflammatory medication (systemic and topical), and hospitalization. In addition, we prepared a tobacco solution made from 10 cigarettes diluted in 100 mL of distilled water mixed with eyewash lubricant and prescribed 2 drops every hour. There was no evidence of intraocular inflammation or inflammation of other organs in the eye. The right eye was normal. The patient remained hospitalized and was discharged on the third day given the fact she was no longer displaying symptoms. In her follow-up appointments 3 and 6 weeks after the event, she did not report any symptoms nor were abnormal signs found in the biomicroscopy.
Figure 1 Biomicroscopic photograph in which a non-pathognomonic conjunctival injection can be observed in the injury caused by the larvae, which presented photophobic behavior, which was why they could not be photographed.
The maggots (larvae) were studied with Lugol stain; they were 1 mm long, with a white-yellowish color, and presented two dark horn-shaped buccal hooks attached to a cephalopharyngeal skeleton. The body had 11 abdominal segments separated by another spiculed ventral. The caudal pole presented a bulging with two terminal lobes and several hooks, data compatible with first-stage O. ovis larvae (figures 2 and 3).

Figure 2 Photograph from an optical microscope (×100) showing an Oestrus ovis larva.
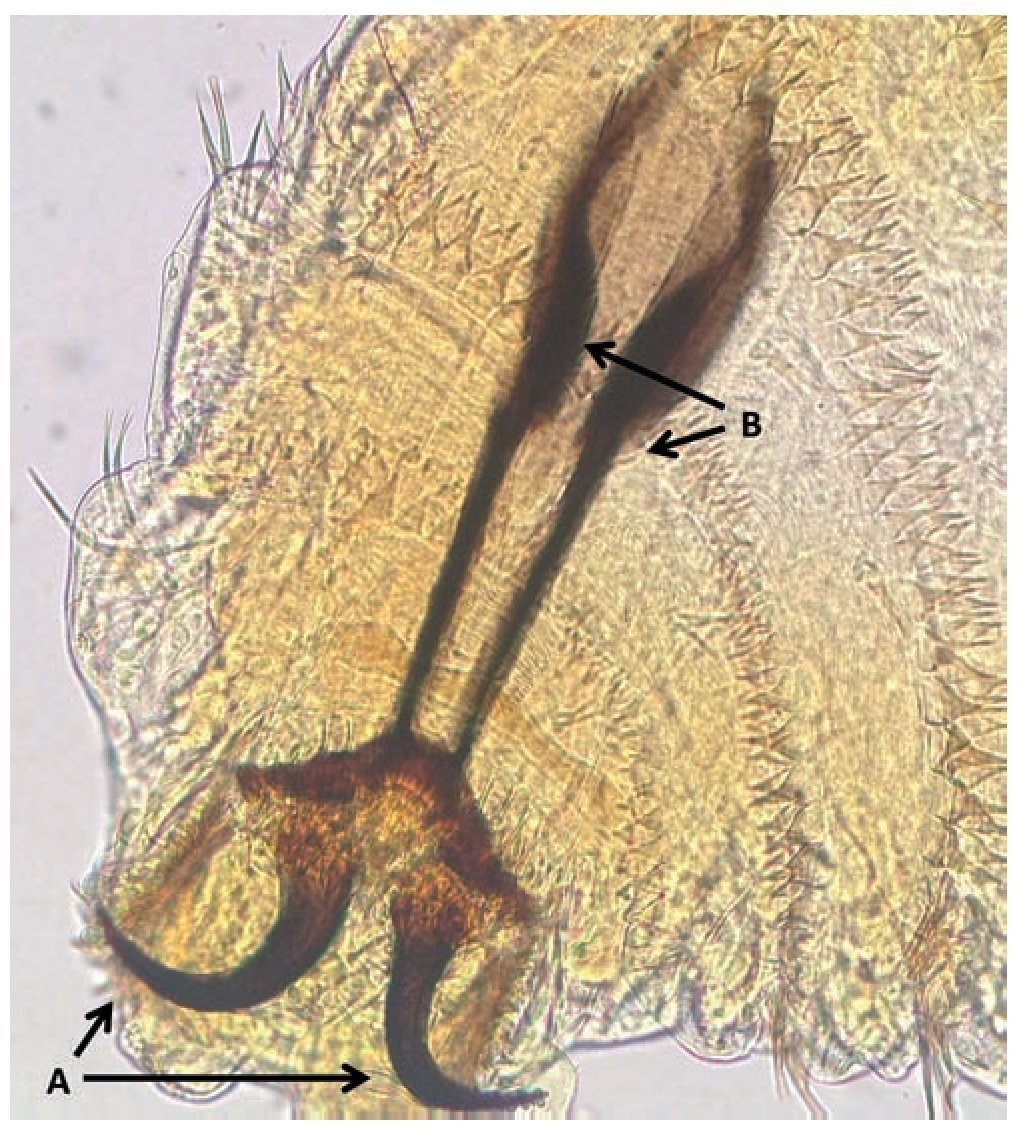
Figure 3 Amplification of a photograph from an optical microscope (×400) of the upper or buccal pole of Oestrus ovis. Two horn-shaped buccal hooks (A) attached to a cephalopharyngeal skeleton (B) can be observed.
Discussion
Ophthalmomyiasis caused mainly by O. ovis is a benign disease.2,3 It has a prevalence of <5% as a cause of myiasis in humans and it is classified as external or conjunctival if the larvae is on the conjunctiva, and internal if it has penetrated the ocular eyeball. External is the most common.4
Parasites from the Cuteribridae(Dermatobia hominis) and Oestridae (Oestrus ovis) families inhabit the nasal cavities of goats and sheep and are the most common cause of ophthalmomyiasis in humans. O. ovis’s females are larviparous and capable of projecting fertilized eggs mid-flight, which makes ovoposition easier.
Patients with this condition present similar symptoms to those of viral or bacterial conjunctivitis, thus causing inaccurate diagnoses.5 A study published by the United Kingdom documented a patient with external ophthalmomyiasis who developed nasal complications, requiring nasal, ear and throat endoscopic inspection.2 On the other hand, our patient did not present any complications.
Jenzeri et al reported a case of keratouveitis secondary to external ophthalmomyiasis in a 77-year-old adult, thus recommended considering ophthalmomyiasis in the differential diagnosis of this disease.6 Sreejith et al reported that O. ovis larvae are incapable of secreting proteolytic enzimes,7 therefore most of them refrain from invading other than the ocular surface. However, small hemorrhages may appear in the conjunctiva where the larvae attach themselves to the eye surface. Our patient certainly presented tiny conjunctival hemorrhages which disappeared shortly after treatment was initiated.
Tropical zones with warm weather, like Central America, the southern United States, Africa and southern Asia, are the most common places to acquire this disease.8 People exposed to animals, or with a degree of immobility are at higher risk.9 Diverse reports have proposed a treatment based on tobacco paste, ether, potassium permanganate, chloroform, pig’s fat, basil, chewing gum and ivermectin. In our clinical case we successfully used a tobacco dilution.
Concerning the pharmacodynamics of tobacco plant leaves (Nicotiana tabacum), authors like Murillo10 have proved that nicotine mimicks the acetylcholine neurotrans-mission action, joins the receptor of the neuromuscular union postsynaptic membrane and stimulates the generation of nervous impulses which can cause the insects’ death. The union of the alkaloid works through two ways: contact with and ingestion of the larvae. This larvacide effect has been exploited for a new generation of insecticides,11 thus preventing new cases, especially in emerging countries.12
Conclusions
External ophthalmomyiasis is an infrequent disease and generally benign. Because O. ovis larvae is deposited on the ocular surface without going through the egg stage, all flies which impact the eye can deposit larvae directly, accelerating conjunctival irritation. The authors consider that one should act carefully in the diagnosis and management of this pathology due to all the possible complications which may be present, such as internal ophthalmomyiasis with possible visual sequels.
Received: November 2013;
Accepted: June 2014
*Corresponding author:
Doctors Hospital Despacho 919,
Ecuador 2331, Colonia Balcones de Galerías,
Monterrey, 64620 Nuevo León, México.
E-mail address: drjuanluisgonzalez@prodigy.net.mx (J.L. González-Treviño).