



A 70-year-old man, non-smoker, referred to pulmonary consultation with 1-year evolution of exertion dyspnea, cough with sputum and wheezing. He worked on stone extraction in a quarry for 7 years and had history of pulmonary tuberculosis, 12 years ago. On physical examination, no relevant alterations. Chest computed tomography scan revealed extensive consolidation in right upper lobe (RUL), in relation to sequels of tuberculosis, and micronodular pattern bilaterally, compatible with silicosis (Fig. 1A). Flexible bronchofibroscopy demonstrated mucosa dark pigmentation in all segmental bronchi (Fig. 1B–D), mostly marked in RUL bronchus and right lower lobe bronchus (Fig. 1B and C), with bronchial distortion. Bronchial biopsy by forceps revealed respiratory epithelium with fibrosis and lymphohistiocytic inflammatory infiltrate with deposition of anthracotic pigment.
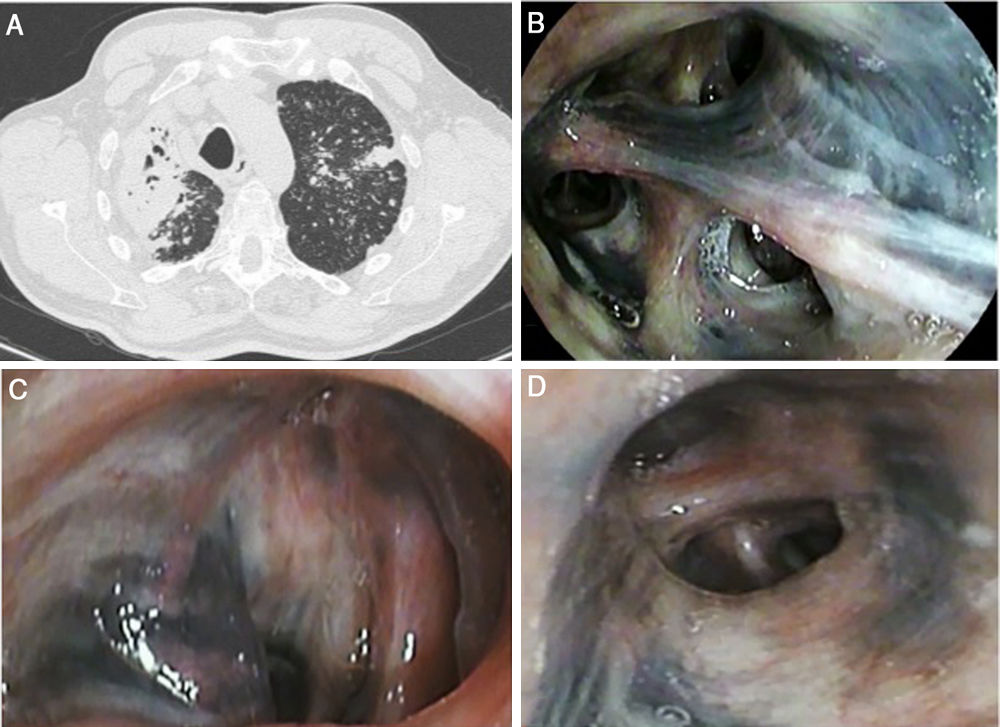
 Axial cut of chest computed tomography scan showed extensive consolidation in right upper lobe, with bronchial distortion; bilateral micronodular pattern, especially in upper lobes. (B–D) Flexible bronchoscopy showed bilateral anthracosis, mostly marked in right upper lobe bronchus (B) and right lower lobe bronchus (C), with endobronchial distortion, and left upper lobe bronchus (D).")
(A) Axial cut of chest computed tomography scan showed extensive consolidation in right upper lobe, with bronchial distortion; bilateral micronodular pattern, especially in upper lobes. (B–D) Flexible bronchoscopy showed bilateral anthracosis, mostly marked in right upper lobe bronchus (B) and right lower lobe bronchus (C), with endobronchial distortion, and left upper lobe bronchus (D).
Anthracosis is characterized by black pigmentation in bronchial mucosa caused by deposit of carbon, silica and quartz particles, characteristically related to pneumoconiosis. Bronchial anthracofibrosis occurs when it causes luminal narrowing or distortion.1,2 Tuberculosis is a frequently associated condition. Anthracofibrosis is established by bronchoscopic visualization with luminal distortion and histological confirmation.1 Radiologic features include multifocal bronchial narrowing, usually involving RUL bronchi, peribronchial cuffing, collapse and consolidation. Given endobronchial and radiological similarities with lung cancer, differential diagnosis can be difficult. Preventive exposure approach remains the only measure.2
Declaration of interest statementThe authors have not declared any competing interests.
The authors acknowledge all the members of Pulmonology Department that contributed to development of this clinical case.
