




Sternal fractures are considered uncommon in paediatric patients. Classically, they have been described as fractures secondary to high-energy trauma that have a risk of associated lesions.
ObjectiveTo describe the clinical and imaging features of sternal fractures in patients less than 18 years of age.
Material and methodsWe retrospectively reviewed 79 paediatric patients diagnosed with sternal fractures after trauma.
ResultsWe found that 92.4% of the fractures were caused by low-energy trauma and that associated lesions were present in only 3 (4%) patients.
ConclusionOur results suggest that sternal fractures in children are often due to lesser trauma and that associated lesions are rare.
Las fracturas esternales se consideran infrecuentes en la edad pediátrica. Clásicamente se han descrito como fracturas secundarias a traumatismos de alta energía y con riesgo de lesiones asociadas.
ObjetivoDescribir los aspectos clínicos y de imagen de las fracturas esternales en niños menores de 18 años.
Material y métodosSe realiza una revisión retrospectiva de 79 pacientes pediátricos con diagnóstico de fractura esternal tras traumatismo.
ResultadoDemostramos que en el 92,4% de los casos, las fracturas son causadas por mecanismos de baja energía y que únicamente en 3 (4%) pacientes se presentan lesiones asociadas.
ConclusiónNuestros resultados sugieren que las fracturas esternales en niños son frecuentemente causadas por traumatismo menor, con escasa incidencia de lesiones asociadas.
Sternal fractures have always been considered uncommon in children, with only short series reported in the specialised literature1 and an estimated total incidence of 0.5–3%.2
In adults, 90% of sternal fractures are the result of high-energy trauma3 and, although not common, the aetiology is usually similar in children. However, there are isolated reports of a different aetiological spectrum in children, showing low-energy trauma fractures without other associated injuries.4 The fracture mechanisms in children include direct impact on the anterior chest wall, hyperflexion associated with compression of the spine, thoracic hyperextension with muscle traction and stress fracture.5
In adults, there is a high incidence of associated injuries, with 77% of cases also having rib or thoracic or lumbar spine fractures, lung contusion, haemopneumothorax, contusions or blunt cardiac injury.3,6–8 Both in children and adults, the risk of associated injuries is greater when high-energy mechanisms are involved.6
Lateral chest and sternum X-rays are usually the initial examination in cases involving low-energy trauma. Ultrasound (US) is very useful for detecting disruption or angulation of the cortex. Computed tomography (CT) is the examination of choice in high-energy-mechanism fractures.9
The aim of this study was to describe the important clinical and imaging findings in children with sternum fractures, based on a larger number of cases than have previously been described in the specialised literature.
Material and methodWe conducted a retrospective, cross-sectional, analytical study in the accident and emergency department of our hospital from June 2004 to May 2016 which included all patients under the age of 18 with a diagnosis of fracture of the sternum in the RIS/PACS system database. We excluded patients who had anatomical variations, including sternal foramen, xiphisternal pseudo foramen or cleft sternum.
The images were analysed by two paediatric radiologists with over 10 years of experience. We included the cases where both radiologists agreed on the diagnosis of sternal fracture from at least one imaging technique. We recorded the characteristics of each fracture, including type, location, angulation, displacement and presence of associated injuries.
The imaging study modalities used were chest X-ray (anteroposterior and lateral), sternum X-ray (anterior oblique and true lateral), US and low-dose chest CT. The ultrasound scans were performed by radiologists, using high resolution transducers.
We reviewed the medical records, recording age, gender, injury mechanism, symptoms, time from injury to first consultation, associated injuries and date of discharge.
The injury mechanisms were classified according to the American College of Surgeons Advanced Trauma Life Support (ATLS) criteria,10 which classifies as high energy: falls from heights of more than three metres or two to three times the height of the child; high-risk road traffic accidents; and impacts by vehicles travelling at over 32km/h. The remaining mechanisms were considered low-energy.
Statistical analysis was performed using the SPSS software (version 17.0, SSPS). A p value <0.05 was considered statistically significant. Central tendency and variability measures were used to describe the relevant data. The ANOVA test was used to analyse the association between fracture mechanism and location.
This study had ethics committee approval.
ResultsWe identified 79 patients diagnosed by imaging with fracture of the sternum; they had a mean of ten years of age, with a range from three to 18, and 63% were male. All the patients had a history of trauma. In 94.9% (75 of 79) of the cases, the fractures were caused by low-energy mechanisms, and only in 5.1% (4 of 79) was the mechanism high-energy (two high-risk road traffic accidents, one high-speed skiing collision and one forced landing in a light aircraft).
In 58.2% (46 of 79) of the cases, the injury mechanism was indirect, including trampoline and chest compression-related injuries, while 37.9% (30 of 79) received direct trauma to the anterior chest wall. In 3.8% (3 of 79) of the cases it was not possible to determine the injury mechanism, so they were classified as “undetermined” (ski collision, tree fall and forced landing in small plane).
In 43% (34 of 79) of the cases, they did not consult the accident and emergency department on the day of the trauma; the mean delay after injury was two days, with a range of zero to 21 days.
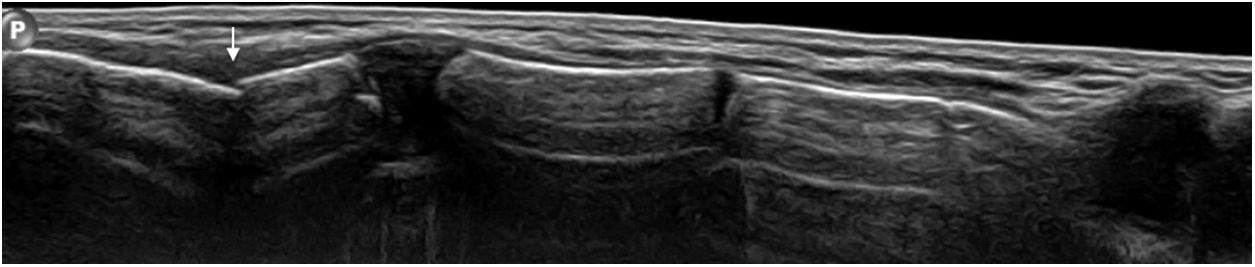
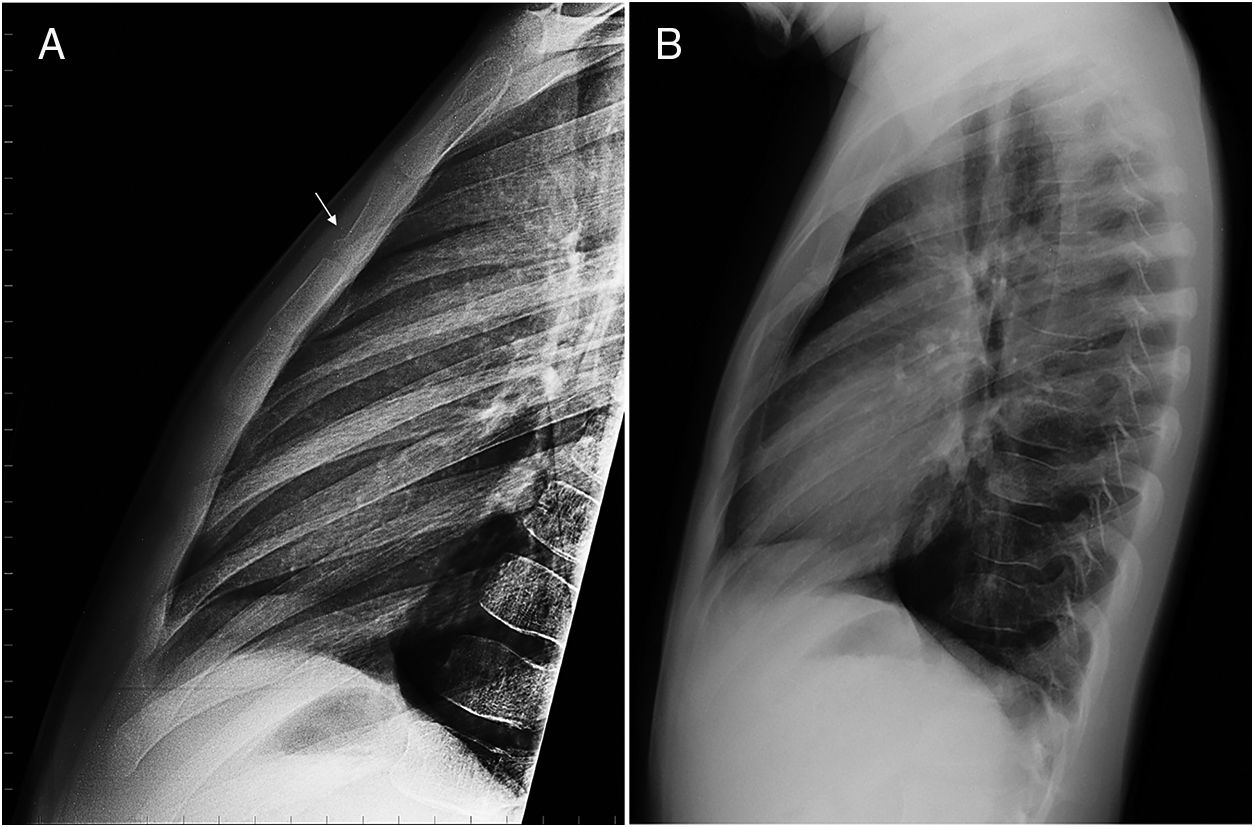
US scan was the test most used for diagnosis (Fig. 1). In 27% (21 of 79) of the cases the chest X-ray showed no signs of sternal fracture and the fractures were identified by a different imaging method (Fig. 2).
 due to a fracture in the manubrium sterni.")
 Lateral X-ray of the sternum: image of a fracture of the anterior cortex of the upper third of the body of the sternum (arrow). (B) Lateral chest X-ray of the same patient, where no fracture line can be seen.")
When X-ray of the sternum was used, all fractures of the anterior cortex were visible in the lateral view, but not in the anterior-oblique views.
The fracture was in the body of the sternum in 78.5% (62 of 79) of the cases, with the upper third being the most common location (66%; 41 of 62); 14.5% (9 of 62) were located in the middle third and 19.3% (12 of 62) in the lower third. The manubrium sterni was affected in 21.5% (17 of 79) of the cases. No xiphoid process fractures or dislocations of the manubriosternal synchondrosis were identified. No significant association was found between the fracture location and the injury mechanism (direct vs indirect) (p=0.095).
The most common finding, in 91.1% of cases (72 of 79), was incomplete, non-displaced fracture of the anterior cortex; 86.1% (62 of 72) had disruption or angulation of the cortex and 13.9% (10 of 72), cortical depression. Of these fractures exclusively involving the anterior cortex, 55.5% (40 of 72) were located in the upper third of the sternal body, 11.1% in the middle third (8 of 72), 15.2% in the lower third (11 of 72), and the remaining 18% (13 of 72) in the manubrium.
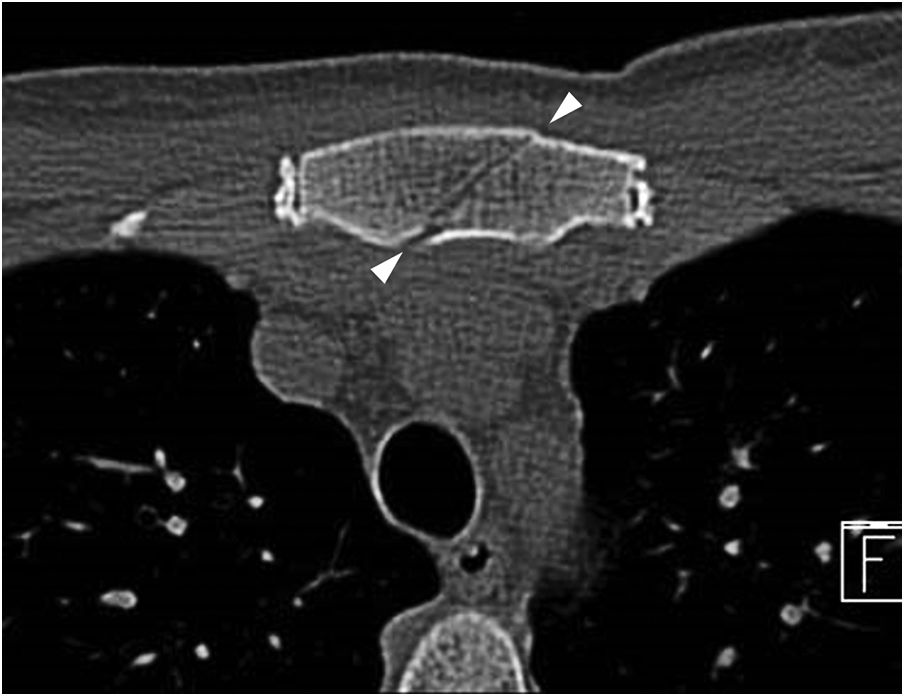
Only 8.9% (7 of 79) of the total were complete fractures (Fig. 3): two indirect-mechanism, high-energy traumas; two indirect-mechanism, low-energy traumas (cervical hyperflexion jumping on a trampoline); and three direct, low-energy sternal contusions. Of the complete fractures, 57% were of the manubrium sterni.
.")
Three patients (3.8%) had associated injuries: two suffered multiple trauma secondary to high-energy mechanisms (thoracic vertebral compression fractures (Fig. 4) and lung contusion associated with multiple fractures); the third patient received direct sternal impact with associated laminar pneumothorax.
, associated with sternal fracture.")
Of the 72 patients who suffered isolated fractures of the anterior cortex, 95% (69) were discharged the same day they consulted; none returned to Accident and Emergency or required additional investigations. The remaining 5% (3 of 72) were admitted to hospital for observation, but were fully discharged within the next 24hours. Of the seven patients who suffered complete fractures, 86% (6) were admitted; one patient for three days due to multiple fractures, and five for 24hours, for observation and pain management.
DiscussionOur study, conducted in an accident and emergency department which receives about 37,000 patients under the age of 18 each year, shows that in children, sternal fractures are frequently secondary to low-energy mechanisms (94.9%). Our findings are consistent with those of several previous small series.4,11,12 In our series, patients consulted on average two days after the injury, suggesting the low intensity of the trauma.
Although the specialised literature has classically described a high incidence of other injuries associated with sternal fractures,6 our series had a low rate of associated injuries (3.8%). In 1993, Heyes et al. published similar results with a retrospective study of 65 adults with sternal fractures, 45 of whom did not have associated injuries.13
It is mentioned that sternal fracture is one of the injuries considered to have the highest specificity in terms of diagnosing suspected child maltreatment or non-accidental trauma in children under two years of age, although there are no pathognomonic fractures. In our series, the youngest child was three years old and there were no suspicions of abuse in any patients.
Analysis of the morphology of the fracture helps determine the injury mechanism.14 In our series, we found that anterior cortex fractures, especially those located in the upper third of the body of the sternum, often involved low-energy mechanisms. However, 50% of fractures secondary to high-energy mechanisms and 57% of complete fractures were located in the manubrium.
Because in our series a large number of cases were non-displaced fractures of the anterior cortex, the anterior X-ray views were not of use for the diagnosis. Lateral X-ray of the sternum, however, is technically easy to obtain and uses bone radiography technical parameters. This gives better definition to the image, so small angulations or interruptions in the continuity of the anterior cortex can be seen clearly, as demonstrated in our series.15,16
The use of ultrasound scans to detect sternum fractures is simple for radiologists trained in the technique and simply requires high resolution linear transducers, which are generally available in all healthcare centres. You et al. recently reported 100% sensitivity and specificity for US in adults with sternum fractures, compared to 70.8% sensitivity and 75% specificity for X-rays.17 The high performance of US in the diagnosis of small anterior cortex fractures, described in the literature and confirmed in our study, supports its use for the diagnosis of this type of fracture.18,19
Analysing the use of imaging in our series of patients, we were able to surmise that the choice of study method depended on the mechanism involved and the patient's clinical condition. If a sternal fracture is clinically suspected in a well child whose traumatic event did not involve a high-energy mechanism, US may be used as the initial examination. If there is a history of low-energy chest trauma with non-specific location, anterior and lateral chest X-rays are recommended. These X-rays will also assess the lungs and the pleural cavity; if the radiological findings are not definitive, US may be useful as a complementary test to detect the presence of a fracture. In the case of high-energy trauma, especially in patients with cardiac or respiratory symptoms, CT assessment of the patient needs to be considered in order to investigate fractures and associated injuries.9,20
The limitations of this study include bias resulting from the retrospective data collection; lack of standardisation in the choice of diagnostic tests used in the accident and emergency department; and possible underestimation of the number of complete fractures in children who were studied exclusively with US, due to method limitation.
ConclusionsOur series shows that sternal fractures in children frequently present as isolated injuries caused by indirect low-energy mechanisms and do not generally require in-hospital management. Being aware of this can help us avoid unnecessary examinations in search of non-existent associated injuries.
The most common imaging findings are of anterior cortex fractures in the superior aspect of the body of the sternum, which do not show up on anterior X-rays.
US is an excellent tool for diagnosing isolated sternal fractures, when a low-energy mechanism was involved.
Authorship1. Responsible for the study as a whole: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
2. Study conception: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
3. Study design: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
4. Data acquisition: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
5. Analysis and interpretation of the data: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
6. Statistical processing: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
7. Literature search: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
8. Drafting of the manuscript: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
9. Critical review of the manuscript with relevant intellectual contributions: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
10. Approval of the final version: KMB, DAC, XOF, CPS, JEJ, MPM and JGL.
Conflict of interestThe authors declare that they have no conflicts of interest.
Please cite this article as: Moënne Bühlmann K, Araneda Castiglioni D, Ortega Flores X, Pérez Sánchez C, Escaffi Johnson J, Pérez Matta M, et al. Estudio clínico radiológico de las fracturas esternales en edad pediátrica. Radiología. 2019;61:234–238.

