



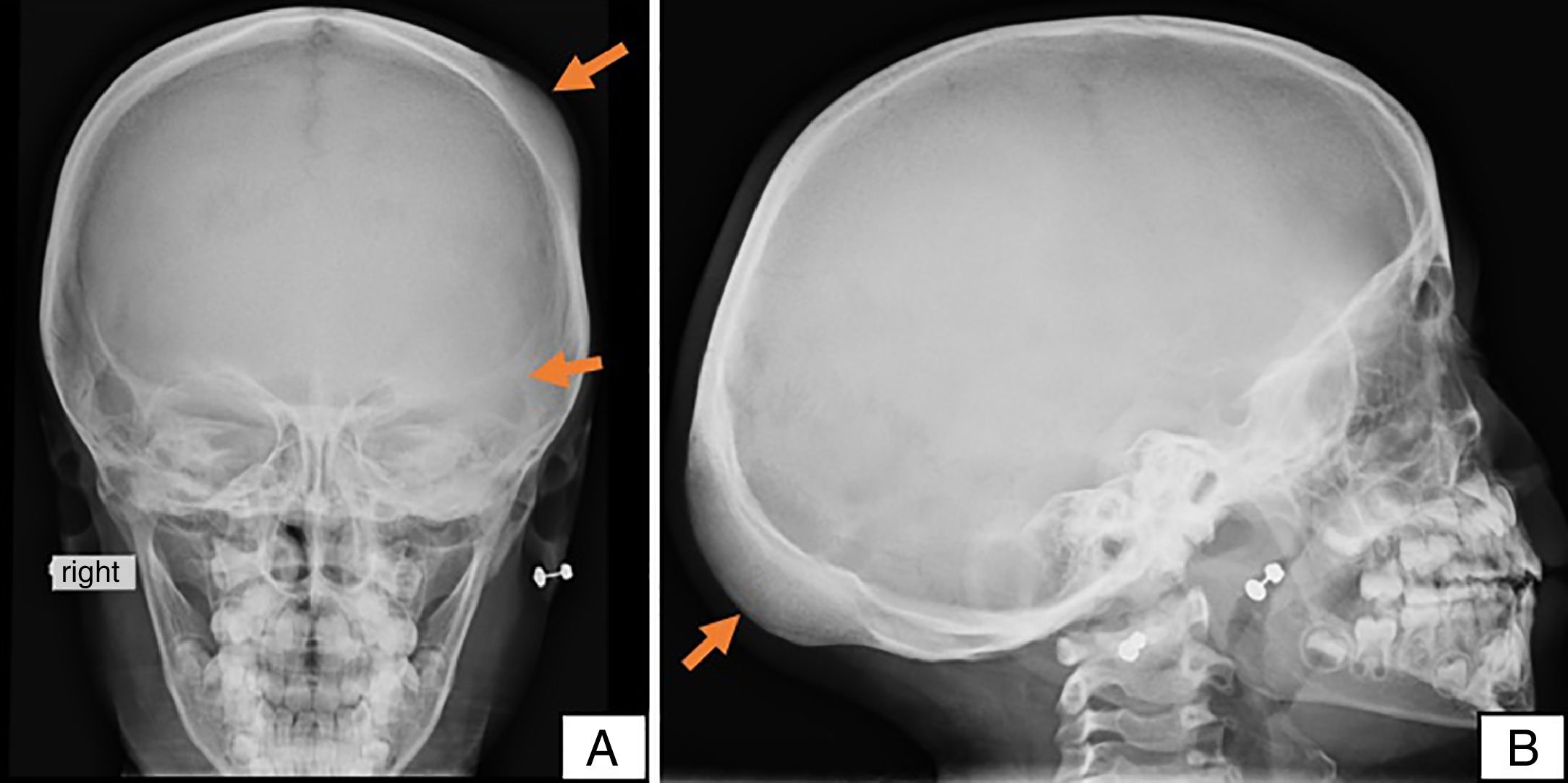
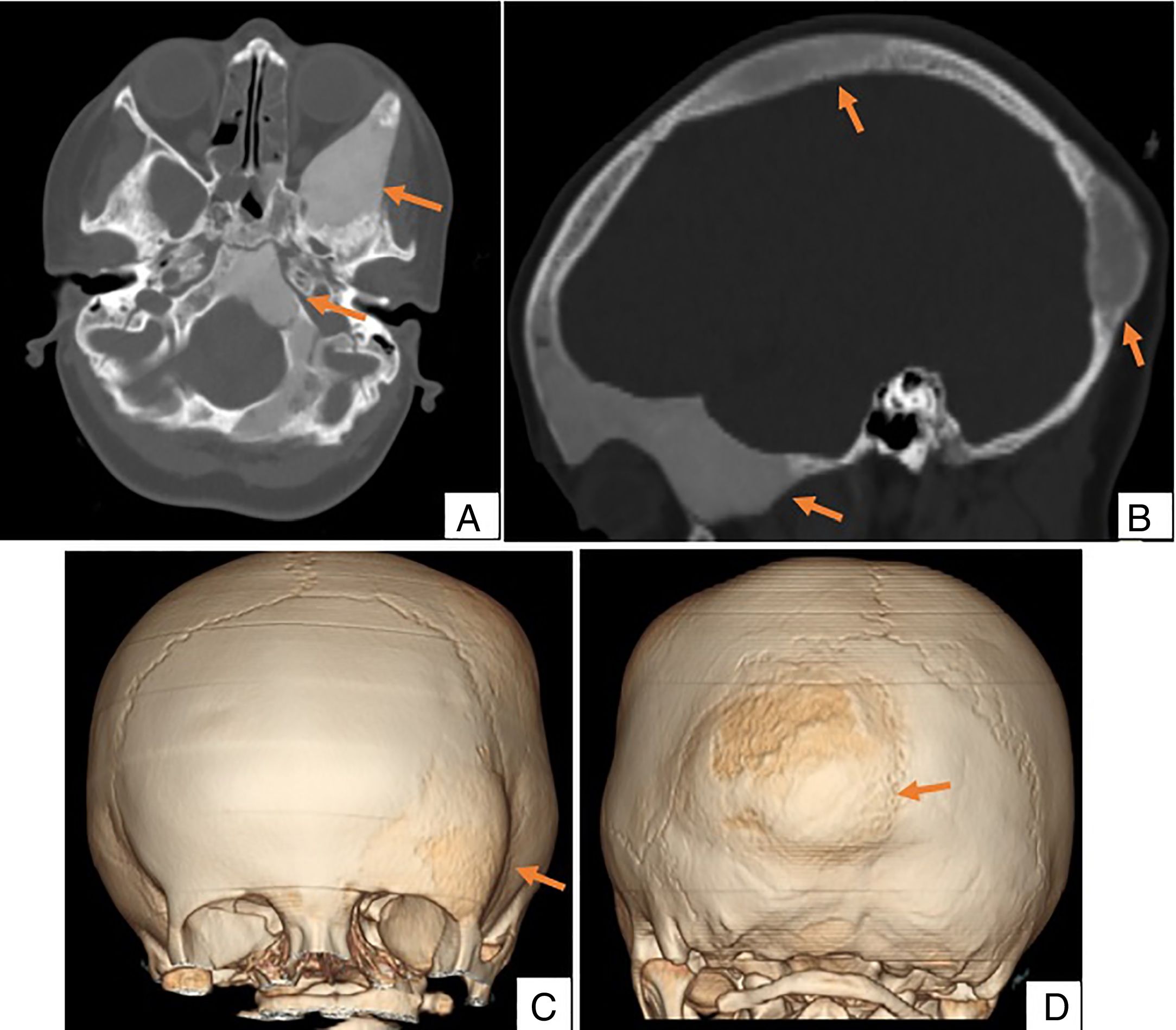
We present the case of a 4-year-old girl with no history of trauma who was brought to the clinic due to a tumour and deformity in the left supraorbital ridge. Anteroposterior and lateral X-rays of the skull (Fig. 1) showed areas of thickening and decreased bone density in the left frontoparietal and occipital regions. The study was completed with a craniofacial computed tomography (CT) scan (Fig. 2) that confirmed these findings. Several enlarged “ground-glass” lesions of homogeneous density were observed in the left frontal, occipital and sphenoid bones.
 and lateral (B) X-rays of the skull. Note the areas of bone thickening and decreased density in the frontal and occipital bones (arrows).")
, sagittal (B), and 3D reconstruction (C and D) confirming and delimiting the ground-glass lesions of homogeneous density in the left frontal, occipital and sphenoid bones, characteristic of polyostotic fibrous dysplasia.")
Fibrous dysplasia is a rare, benign, hamartomatous disease characterised by replacement of normal bone matrix by fibrous connective tissue that shows various degrees of metaplasia on histology study.1 The aetiology is genetic, and the condition is caused by a sporadic post-zygotic mutation in the GNAS 1 gene (chromosome 20q13).1,2
It can affect a single bone (monostotic), which is the most frequent form (70–80%), or several bones (polyostotic).2 Craniofacial polyostotic fibrous dysplasia is a type of fibrous dysplasia characterised by involvement of the skull and facial bones, including the mandible and maxilla.1
The most common clinical presentations are aesthetic deformities, neurosensory abnormalities, visual impairment, proptosis and nasal malformation.2
The diagnosis of polyostotic fibrous dysplasia is based on clinical symptoms and radiological findings.1 The main radiological feature is the appearance of asymmetric “ground-glass” densities that blend into normal bone, thin cortices and bone expansion.3
The radiological protocol for diagnosing polyostotic fibrous dysplasia consists of scintigraphy followed by a simple X-ray of the areas that show increased radioisotope uptake. This study can be complemented by CT, which is useful in confirming diagnosis and establishing the extension of involvement.1
In patients presenting neuropathy, contrast-enhanced CT or magnetic resonance imaging should be performed in the early stages of diagnosis to determine the degree of nerve compression.4
Four differential radiological diagnoses should be considered: skull base meningioma, cranial osteoma, ossifying fibroma of the maxilla and Paget's disease.
The aim of treatment is to prevent the onset of pathological fractures, control pain and reduce bone deformities. The first choice in asymptomatic patients is radiological follow-up. Surgical treatment is reserved for symptomatic cases.2
The risk of recurrence is greater in the growing period, and increases in cases of conservative surgery in which complete resection of the lesion is not feasible. Malignant transformation has only been reported in a few cases. One of the main causes of this is radiotherapy. Patients with the polyostotic form are more at risk than those with monostotic fibrous dysplasia.2
Fibrous dysplasia is an uncommon disease characterised by dystrophy and secondary metaplasia of the bone. It occurs mainly in children and is characterised by slow development until puberty. Diagnosis is based on clinical findings and radiological tests, and for this reason it is important to be familiar with the typical radiological signs of this entity in order to choose the right treatment.
Please cite this article as: Moya Sánchez E, Ruiz de Arévalo García Á. Displasia fibrosa poliostótica craneofacial: hallazgos por imagen. Radiología. 2019;61:177–178.

