


Chronic shoulder pain is one of the most frequent causes of consultation for musculoskeletal pain. Physical and drug therapy usually result in little improvement and surgical intervention commonly fails. Tricompartmental blockade of the shoulder is an option when baseline therapy fails and ultrasonography is a tool that facilitates the approach, improves the efficacy and reduces the complications.
ObjectiveTo determine the efficacy and safety of ultrasound-guided tricompartmental blockade of the shoulder in chronic pain patients.
Methods and materialsA descriptive, prospective, follow-up study was made of a cohort of 19 patients with chronic shoulder pain receiving ultrasound-guided tricompartmental blockade of the shoulder. Data were collected prior to the procedure with four, eight and sixteen week controls. Pain intensity was measured with the visual analog scale.
ResultsAverage age was 58.89 years, 73.7% were females. All patients referred severe pain prior to the block. The percentage of patients with reduced pain in the four follow-up periods was 78.3%.
ConclusionsChronic shoulder pain considerably affects the quality of life. Tricompartmental blockade of the shoulder is an alternative when drug therapy fails, with good outcomes, although the scientific evidence is very scarce. In our study the ultrasound-guided tricompartmental blockade of the shoulder is an effective and safe technique.
El dolor crónico de hombro es una de las causas más comunes en la consulta de dolor osteomuscular. Es frecuente encontrar poca mejoría con la terapia física y farmacológica y fallo en la intervención quirúrgica. El bloqueo tricompartimental de hombro es una alternativa cuando la terapia de base no funciona, y la ultrasonografía es una herramienta que facilita el abordaje, aumenta la eficacia y disminuye las complicaciones.
ObjetivoDeterminar la eficacia y la seguridad del bloqueo tricompartimental de hombro guiado por ultrasonografía en pacientes con dolor crónico.
Métodos y materialesSe realizó un estudio de tipo descriptivo, prospectivo, de seguimiento a una cohorte de 19 pacientes con dolor crónico de hombro que recibieron un bloqueo tricompartimental de hombro guiado por ultrasonografía. Se obtuvieron datos antes del procedimiento, y seguimientos a las 4, 8, 12 y 16 semanas. La intensidad del dolor se midió con la escala visual analógica.
ResultadosEl promedio de edad fue de 58-89 años, con una proporción de mujeres del 73,7%. Todos los pacientes refirieron dolor severo antes del bloqueo. La proporción de pacientes con disminución del dolor en los 4 períodos de seguimiento fue del 78,3%.
ConclusionesEl dolor crónico de hombro afecta de manera importante a la calidad de vida. El bloqueo tricompartimental de hombro es una alternativa cuando fracasa la terapia farmacológica, con buenos resultados, aunque la evidencia científica aún es muy baja. En nuestro estudio el bloqueo tricompartimental de hombro guiado por ultrasonografía es una técnica eficaz y segura.
Chronic shoulder pain is one of the most frequent reasons for musculoskeletal pain consultation. It causes considerable functional limitation and affects the quality of life. In the United States, shoulder pain is the third cause of musculoskeletal disability.
Pain may originate in areas other than the shoulder. When the cause of pain is intrinsic to the joint, it may originate at various structures: muscles, ligaments, bones or nerves, all of them with symptoms and similar clinical evaluation, making the etiological diagnosis difficult and misleading.
The initial treatment of most causes of pain is conservative, based on drug therapy and physical rehabilitation; however, it is usual to find patients who fail to show any improvement in their pain intensity and mobility with conservative therapy and surgical intervention.
Tricompartmental blockade of the shoulder (TBS) is a technique used in patients with shoulder pain refractory to conventional therapies.1 The drugs most commonly used for this blockade are corticosteroids with varying grades of effectiveness, depending on the study and the cause of pain, but most report improved mobility and pain relief after 12–16 weeks.2
In the past, this technique was performed blindly with adverse events and frequent blockade failure due to injection in the wrong site. Hence, an image-guided technique shall provide higher precision and efficacy.3
Despite ultrasound-guidance has been rarely studied in TBS, it could improve both the intervention and the outcomes,4 resulting in multiple advantages over the blind technique,5 including better precision for anatomical localization and fewer complications.
Fluoroscopy has been the most frequently studied image-guided technique for TBS and the first to be described. There is very little research describing the advantages of other imaging techniques, such as MRI and ultrasonography that is the topic of this paper.6
Consequently, the purpose of this paper is to determine the efficacy and safety of ultrasound-guided TSB in patients with chronic benign pain.
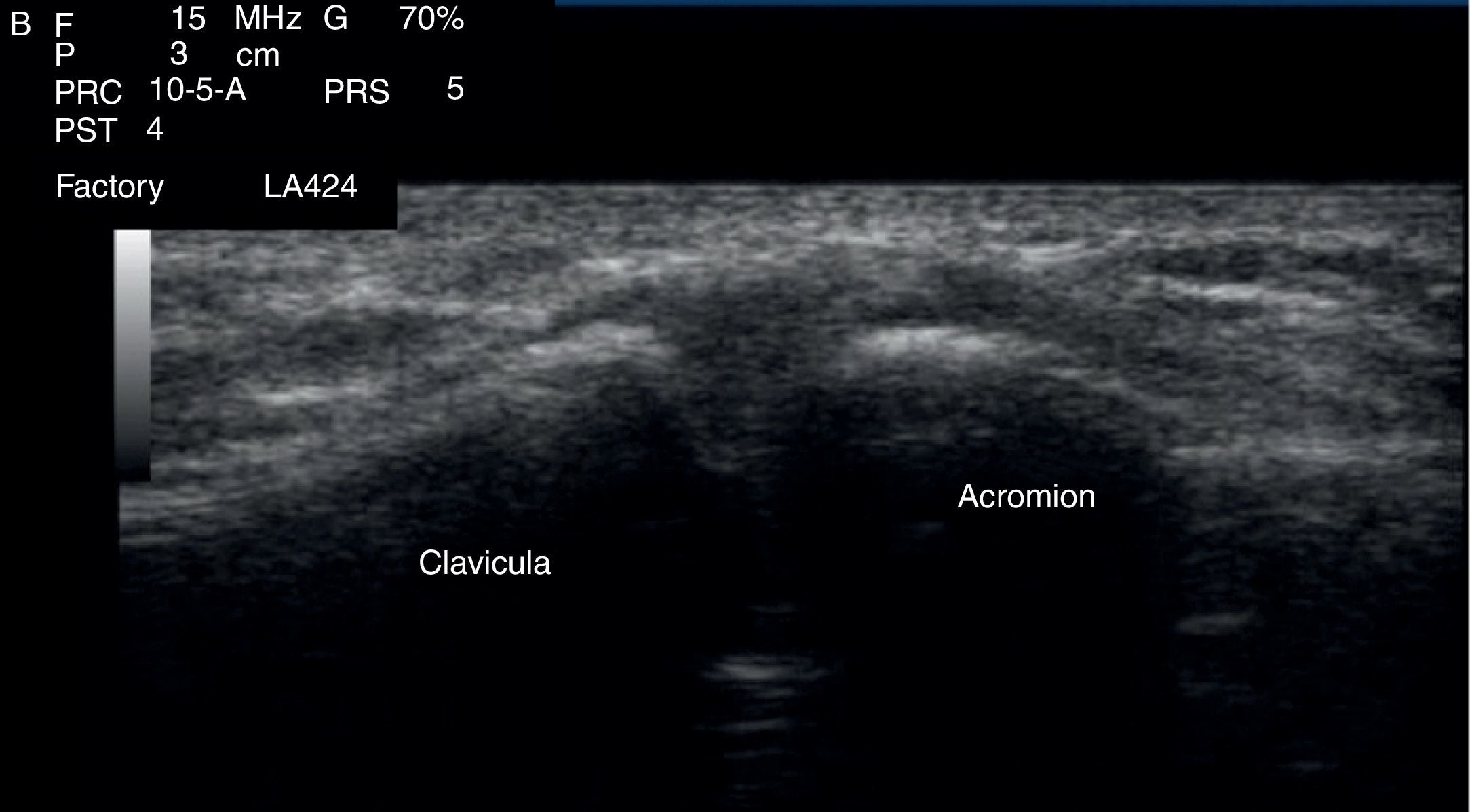
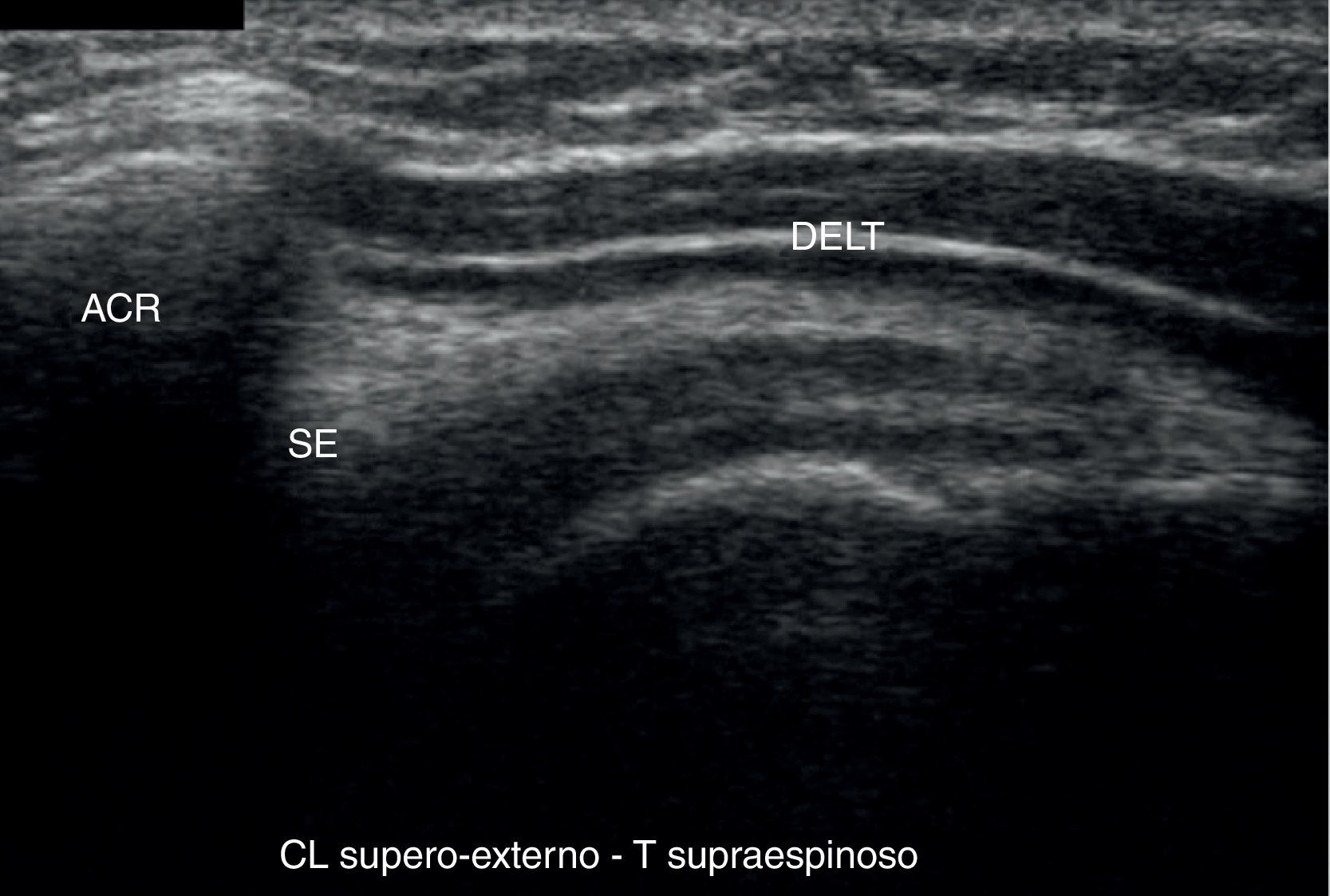
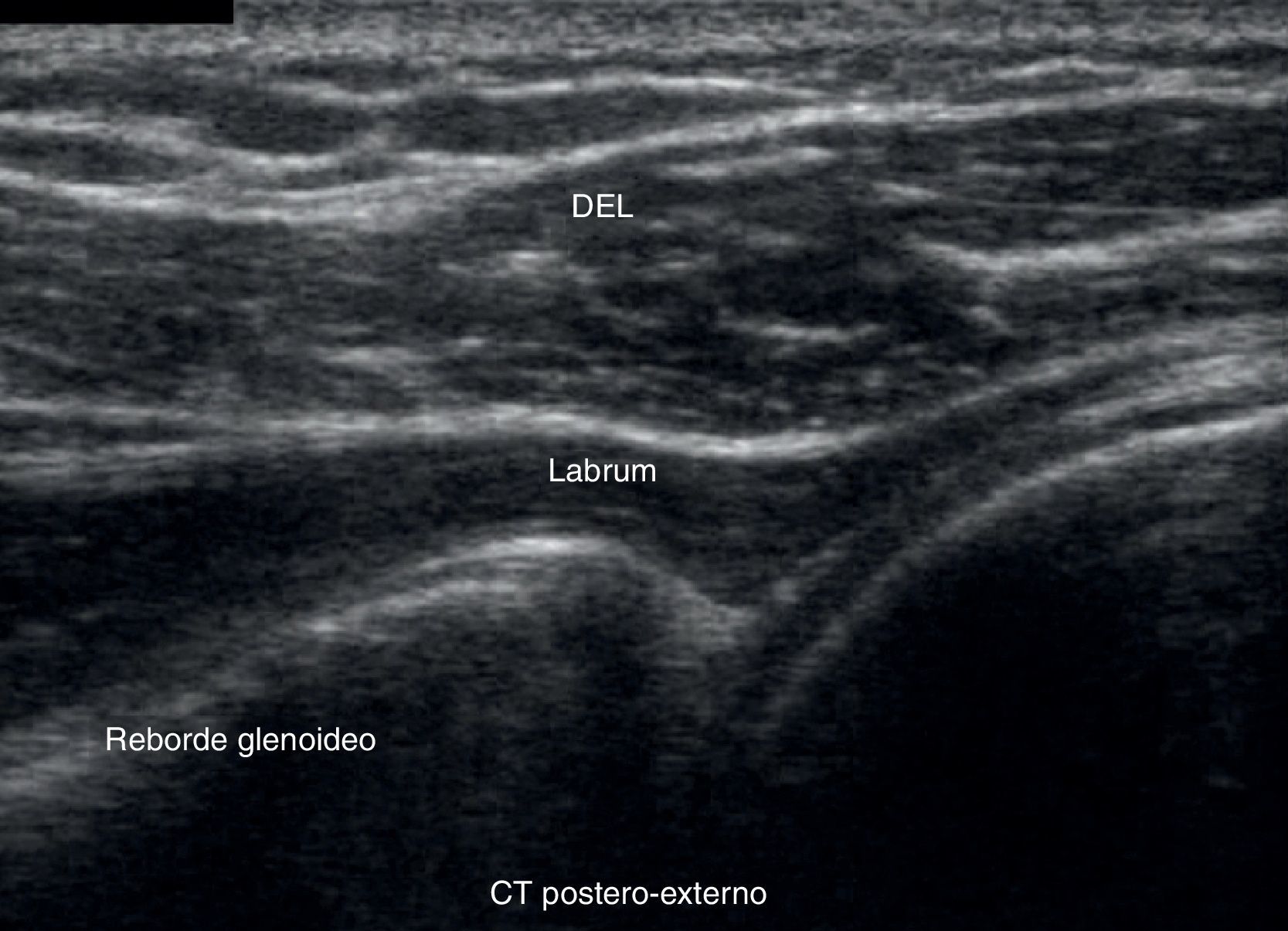
Materials and methodsFollowing the approval of the institutional ethics committee, an observational, descriptive, prospective follow-up trial was completed in a cohort of patients with chronic shoulder pain pathology undergoing ultrasound-guided interventional therapy with TBS using 9mL combination of 0.5% bupivacaine (without epinephrine) plus 50mg of triamcinolone. A portable ultrasound machine with lineal transducer (7–12MHz) was used. The blockades were performed in the minor procedures room using aseptic techniques. The infiltrations were done using a 22 gauge spinal needle and 10mL syringe. Patients were placed in a sitting position, disinfected with chlorhexidine and 2mL were infiltrated in the acromioclavicular joint (Fig. 1), 4mL in the subdeltoid bursa (Fig. 2) and 3mL in the glenohumeral joint (Fig. 3). All patients were evaluated prior to the procedure and followed at four, eight, twelve and sixteen weeks. Age, gender, diagnosis, pain intensity using the visual analog scale (VAS) and the presence of blockade-related complications were evaluated. Pain relief was defined as at least 50% VAS improvement. The sample was taken from patients who came to the pain clinic at the Colombian Pain Institute in Medellin between June 2011 and March 2012 and who met the inclusion and exclusion criteria. The data were collected from revision consultations.



The following were the inclusion criteria: (1) diagnosis of chronic shoulder pain (over 3 months of evolution), (2) undergoing shoulder TBS and (3) use of ultrasound guidance for doing the blockade.
The following were the exclusion criteria: (1) indication for interventionist management with multiple simultaneous blockades, (2) prolotherapy or radiofrequency pain management of the suprascapular nerve in the last two years, (3) insertion of the perineural continuous infusion catheter and (4) unable to quantify pain intensity.
The database was stored in an Electronic Spreadsheet Program and the software used for the analysis of the data was SPSS 18 (under a license from CES University). A descriptive analysis for all the variables studied was done, supported by the calculation of percentages and descriptive measurements. A paired analysis was used to establish the difference between pain intensity before and after the procedure using Wilcoxon's test, with a 5% level of statistical significance and 95% confidence interval.
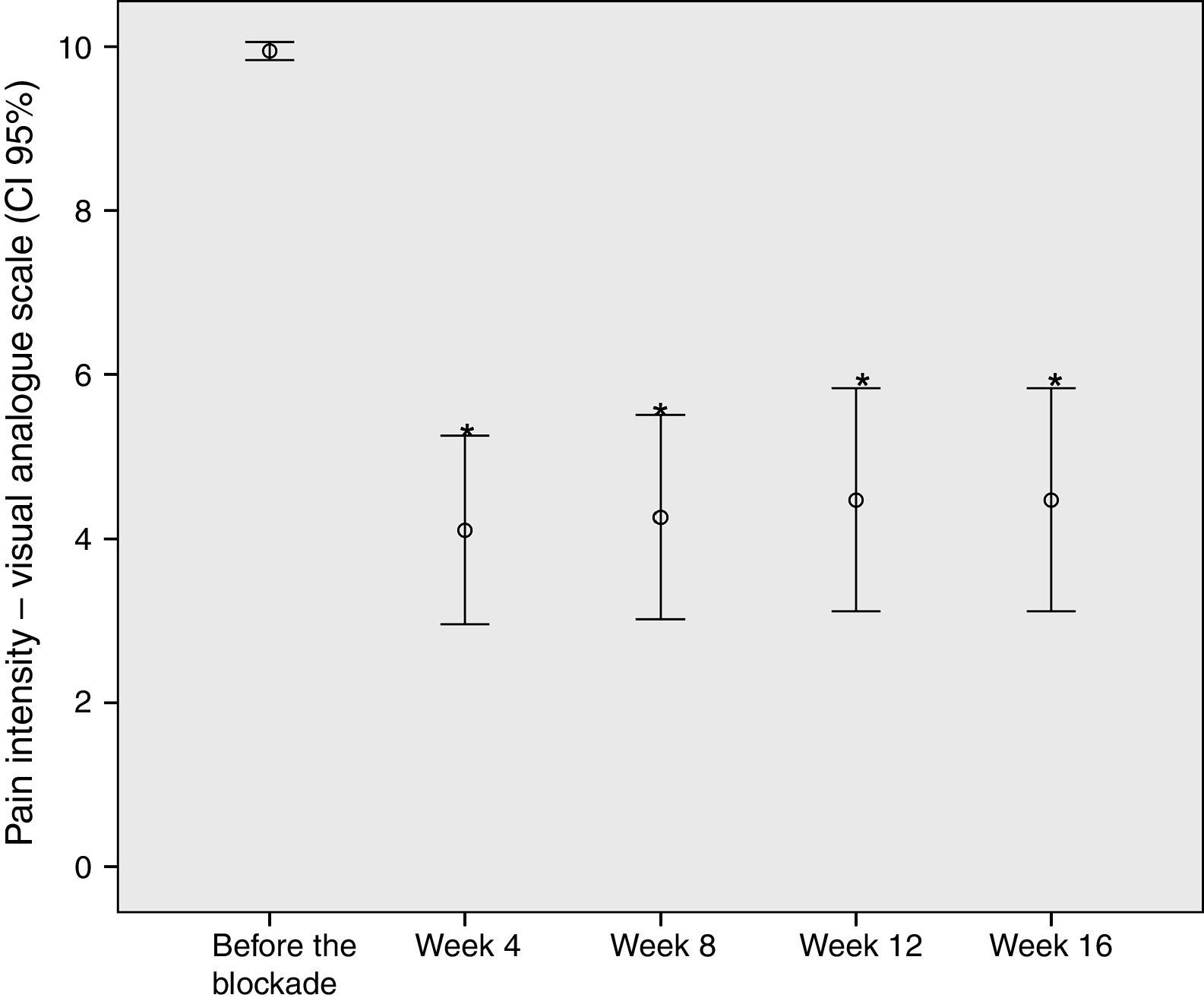
ResultsA total of 19 ultrasound-guided TBS treated patients were analyzed. The average age was 58.89 years (SD±15.3), 73.7% women. All patients referred severe pain prior to the blockade (Table 1). The most frequent diagnosis was rotator cuff syndrome (8 patients), followed by supraspinatus tendonitis (4 patients), osteoarthrosis (4 patients) y subdeltoid bursitis (3 patients).
The proportion of patients with improved pain in the four follow-up periods of time was the same at 78.3%.
The difference between the initial VAS means and the following evaluations was 5 points with statistical significance (p<0.0001) (Fig. 4).
 at various times during observation.")
Analyzing the subgroup of patients who did not improve, 75% of them had a diagnosis of arthrosis of the shoulder. There were no gender differences and no complications were reported.
DiscussionAs previously discussed, TBS is a relatively non-invasive option for the treatment of chronic pain, considering that blind blockade has a high probability of failure and should no longer be used. Imaging guidance improves both efficacy and safety. When blind blockade is done and images are taken to verify the needle localization, proper needle placement has been identified only in 39–66% of the cases.7,8 In contrast, image guided procedures exhibit a 95–100% success rate.9,10
A systematic review reported that a series of three shoulder blockades accomplished a 16-week improvement in pain and mobility and that there is no additional benefit with four or more sessions.11 Similar results were obtained with our research using one session per patient.
It has also been reported that corticosteroid TBS plus physical therapy is ore effective in reducing pain and improving the range of movement when compared against physical therapy alone.12
The most frequently used images for blockade guidance are first fluoroscopy13 and secondly ultrasonography.9 Fluoroscopic guidance is an excellent tool to visualize the bone compartments, in this particular case the glenohumeral and the acromioclavicular; however, the third compartment, the subdeltoid bursa is a space between the muscles and the supraspinatus, structures that are not properly visualized using ultrasound. It is also frequent that shoulder pain be originated in the long segment of the head of the biceps, another structure not visualized fluoroscopically. For these reasons, ultrasound becomes an effective tool for visualizing all of the shoulder structures: muscles, joints and nerves, plus additional advantages against fluoroscopy, such as easy to transport equipment and absence of radiation.14,15
The major difficulty in chronic shoulder pain studies is the multiplicity of pain etiologies in this joint. The shoulder may be labeled as the great simulator joint, since there are multiple extrinsic and intrinsic shoulder pathologies that cause pain in the area and each of them has a different pathophysiology and treatment approach. Only a comprehensive clinical evaluation supported by diagnostic tools will establish whether a patient is a candidate for TBS.
ConclusionsChronic shoulder pain is a pathology that greatly affects quality of life. Drug therapy and physical rehabilitation are the first line of treatment. Less invasive interventionist therapies are currently being used with good results, though the scientific evidence is still limited. In our study, ultrasound-guided TBS was effective and safe for the treatment of pain. Ultrasonography is available in our healthcare environment and hence blind blockade is no longer considered a good practice, in the light of the notable difference between both techniques.
FinancingThis work was done with the author's own resources and the advice of CES University (Medellin – Colombia).
Conflicts of interestThe authors have no conflicts of interest to disclose.
We thank Doctor Juan Felipe Giraldo Cardona for his contribution with ultrasound.
Please cite this article as: Díaz RCR. Bloqueo tricompartimental de hombro guiado por ultrasonografía. Rev Colomb Anestesiol. 2013;41:245–249.