



Emotional distress is common in Colombian armed conflict victims. Multiple-victimisation is associated with an increase in emotional distress than victimisation due a single event. However, the association between poly-victimisation and emotional distress among victims of the armed conflict in Colombia has not been documented.
ObjectiveTo study the association between multiple-victimisation and emotional distress in victims of armed conflict in the State of Magdalena, Colombia.
MethodsA cross-sectional study was designed, with a secondary analysis of registration of the Psychosocial Care Program and Victim Integral Health (PAPSIVI) in the State of Magdalena, from 2013 to 2014. The profile formula grouped demographic variables, victimising events, and a set of symptoms of emotional distress (perceived discrimination, depressive and anxiety-stress). Odds ratio (OR, 95%CI) were established as measures of association.
ResultsA total of 943 people were included, with 67.4% women, and ages between 18 and 94 years (mean 47.9±14.2). A total of 109 (11.7%) suffered from multiple victimisation. Multiple victimisation events were associated with more emotional distress, depressive symptoms (OR=1.5; 95%CI, 1.3–1.8), perceived stigma (OR=1.3; 95%CI, 1.1–1.5), and anxiety-stress (OR=1.2; 95%CI 1.0–1.4) than a single event.
ConclusionsThere are more emotional distress in multiple victimisations than in a single victimisation event during armed conflict in this region of Colombia. Further studies are required on this topic.
El sufrimiento emocional es frecuente en víctimas del conflicto armado colombiano. La polivictimización se asocia a mayor número de sufrimientos emocionales que la victimización debida un único evento. Sin embargo, hasta la fecha no se ha documentado la asociación entre polivictimización y sufrimiento emocional en víctimas del conflicto armado en Colombia.
ObjetivoEstudiar la asociación entre polivictimización y sufrimiento emocional en víctimas del conflicto armado del Departamento del Magdalena, Colombia.
MétodosSe diseñó un estudio transversal, un análisis secundario del registro del Programa de Atención Psicosocial y Salud Integral a Víctimas (PAPSIVI) del Departamento del Magdalena, 2013-2014. El formulario de caracterización agrupó variables demográficas, eventos victimizantes y un conjunto de manifestaciones de sufrimiento emocional (discriminación percibida, depresión y ansiedad). Se establecieron razones de disparidades como medidas de asociación.
ResultadosSe incluyó a 943 personas, el 67,4% mujeres, con edad de 18-94 años (media, 47,9±14,2). Un total de 109 (11,7%) presentaron polivictimización. La polivictimización se asoció a mayor sufrimiento emocional que la victimización por un único evento, síntomas depresivos (odds ratio=1,5; intervalo de confianza del 95%, 1,3-1,8), estigmatización percibida (odds ratio=1,3; intervalo de confianza del 95%, 1,1-1,5) y ansiedad-estrés (odds ratio=1,2; intervalo de confianza del 95%, 1,0-1,4).
ConclusionesLa polivictimización incrementa el sufrimiento emocional más que la victimización por un único evento en personas víctimas del conflicto armado en esta región colombiana. Es necesario investigar más en esta área.
Poly-victimisation is defined as the simultaneous occurrence or presentation of multiple forms of interpersonal violence.1,2 Undoubtedly, these negative events play a fundamental role in the pathogenesis of symptoms related to mental disorders.3,4
Victims of a single event, whether natural or the result of violent human actions, frequently relate emotional distress following the events.5,6 Likewise, it is observed that people who report poly-victimisation relate greater emotional suffering than those who report a single event in a given period.7–11 Consequently, in people who present poly-victimisation, the frequency of emotional problems is higher, as is the probability of meeting the criteria for a mental disorder as a result.12–15
Poly-victimisation is not a one-dimensional phenomenon, but a diverse set of painful or traumatic experiences with unique implications for each group of victims of the internal armed conflict due to material and immaterial losses, lifestyle changes and coping with new challenges or risks.16,17 The internal armed conflict in Colombia is a significant cause of poly-victimisation; in addition to forced displacement, there are other forms of violence such as direct death threats, disappearances of relatives and acquaintances, murders, kidnappings, torture and sexual assaults, thus increasing the sources of suffering.18
Emotional symptoms and potential mental disorder cases are highly frequent among victims of the internal armed conflict in Colombia. In Colombian adults who have fallen victim to the internal armed conflict and been displaced, the prevalence of potential mental disorder cases exceeds 20%.19 However, in the general population, potential cases of mental disorders, anxiety and depression are observed less frequently, reaching 10% when quantified with the Self-Reporting Questionnaire (SRQ).20
Poly-victimisation has been studied in other countries, particularly in children and adolescents7–11 and, most recently, among adult men and women in other situations besides those occurring in the context of the Colombian armed conflict.12–15 Poly-victimisation is a more stressful eventuality than re-victimisation, i.e., the repetition of the same situation of victimisation7; however, to date, the association between poly-victimisation and emotional suffering among victims of the Colombian armed conflict has not been quantified. A greater frequency and, consequently, a disproportionate number of cases of emotional suffering can be expected among those who report poly-victimisation than those who only present a single victimisation event in the context of the armed conflict.1
In order to meet the needs of the people who have been directly affected by the armed conflict, the Programme for Psychosocial and Integrated Health Care for Victims (PAPSIVI) was created.21 The process began with the registration of the conflict victims, and an instrument was later created to record manifestations of emotional suffering which was consistent with the psychosocial approach protocol for the adoption of comprehensive care, assistance and psychosocial support measures for victims of the armed conflict.22 The naming of potential mental disorders was actively avoided, given the instrument's lack of diagnostic pretensions. Moreover, it is necessary to keep in mind that “diagnosis” is the result of an elaborate analytical process of classifying and explaining a person's emotional suffering, and it can only be performed by professionals with clinical training. Likewise, this approach helps to minimise the possibility of adding another victimisation event, secondary to the stigma, leading to the formal diagnosis of a mental disorder.13
In some situations, the stigmatisation of the victim increases the likelihood of them reporting symptoms of distress that are traditionally related to post-traumatic stress disorder13 and, in the context of the Colombian armed conflict, the displacement situation per se has been stigmatised by various mechanisms or reasons.23 This study quantified the association between poly-victimisation and emotional suffering in the Department of Magdalena to go beyond the simple deduction that “more is worse”,1 since interpersonal victimisation presents a different dynamic to victimisation or poly-victimisation due to accidental events or natural disasters.2
The growing implementation of differential care within the Colombian General System of Social Security in Health renders it necessary to have information that allows for prioritisation or special actions with regard to people in a situation of poly-victimisation, as required by the Colombian law for victims of the internal armed conflict.24
The objective of this research is to study the association between poly-victimisation and emotional suffering among victims of the armed conflict in 15 priority municipalities within the Department of Magdalena in the 2013–2014 period.
MethodsA quantitative, analytical, observational and cross-sectional study was designed, for which information was collected from victims of the armed conflict in the Department of Magdalena. For the research, we had permission to review and analyse the information, though this type of research does not pose any risk to the participants, since no interviews are conducted and only digitised materials are reviewed. Furthermore, for the analysis, the names of the participants were omitted and replaced with a code in order to respect confidentiality, as per Ministry of Health Resolution 8430 of 1993.25
Adults over 18 years of age who participated in the victim characterisation process of the priority municipality in the Department of Magdalena were included in this analysis. Cases where interviewers did not record victimising events, did not complete demographic information or did not complete all manifestations of emotional suffering were excluded. Likewise, characterisation sheets that presented errors in the digitisation process which limited their legibility were excluded from the analysis. In the Department of Magdalena, between 2013 and 2014, 5220 victims were officially registered, distributed across the 30 municipalities in the department; however, the greatest concentration was found in half of them. For this analysis, there was a non-probability sample, for convenience, of victims of the armed conflict in 15 municipalities in the Department of Magdalena.
The PAPSIVI characterisation form consolidates demographic information, family characteristics and a set of manifestations of the condition suffered due to victimising events, including emotional suffering.
A group of 15 of the most common manifestations of emotional suffering reported in the studies conducted on victims of victimising events was evaluated. A team of psychologists constructed a characterisation guide, including 31 emotional manifestations that in this clinical context may be interpreted as symptoms of anxiety, depression or post-traumatic stress, among others. For this analysis, those that are closely related in theory and appearance to perceived stigma (degradation, helplessness, humiliation, inferiority, feelings of insecurity and shame), the anxiety-stress symptoms listed in the international classifications (aggressiveness, anxiety, fear or permanent state of alert, apathy or disinterest, despair and feeling of vulnerability) and depressive symptoms (cycles of anger and sadness, frequent crying, feeling of loneliness and sadness) were taken into account. This selection was carried out after an exploratory factorial analysis process to extract the items that performed best in the abovementioned three dimensions. Each emotional manifestation was evaluated dichotomously, whether present or absent, at the time of the interview.22
The list of victimising events included death threats, disappearances, forced displacement, murders, kidnappings, torture and various forms of sexual violence. The presence of two or more victimising events perceived by the same person related to the internal armed conflict was considered poly-victimisation.
A univariate descriptive analysis was performed on each of the variables. Frequencies and percentages of the nominal data and mean±standard deviation of the quantitative data were observed. To explore the association between poly-victimisation (taken as an independent variable) and manifestations of emotional suffering (conceived as dependent variables), odds ratios (ORs) were estimated with their 95% confidence intervals (95% CI). The associations between poly-victimisation and psychosocial manifestations were adjusted by logistic regression, and demographic variables were taken as covariates or confounding variables. We also performed a factorial analysis using the principal component method to transform and reduce the three groups of manifestations of emotional suffering to a single variable for each one.26 This process was performed because the set of symptoms was not taken as constructs (perceived stigma, anxiety-stress and depressive symptoms) in the initial construction of the measuring instrument, in which case the calculation of Cronbach's alpha would have been sufficient.27
The calculations were performed with the IBM-SPSS Statistics package.28 Adjusted associations that did not include the unit (1.0) in the confidence interval were accepted as significant.29 Goodness-of-fit was determined using the Hosmer–Lemeshow test.30
ResultsOf the 5220 victims registered in total, 1388 people were interviewed. However, 443 interviews (31.9%) were excluded due to data omission or illegibility following a poor digitisation process. Finally, for this analysis, there was a group of 943 participants that presented complete information.
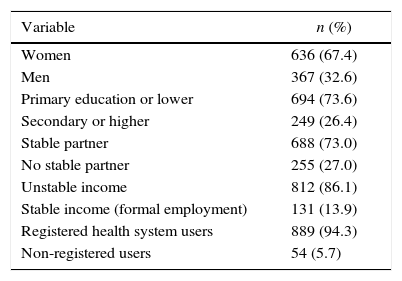
The participants were between 18 and 94 years old (mean, 47.9±14.2); 881 people (86.0%) were aged between 18 and 64 years and 132 (14.0%) were 65 or older. Other characteristics are shown in Table 1.
Demographic characterisation.
| Variable | n (%) |
|---|---|
| Women | 636 (67.4) |
| Men | 367 (32.6) |
| Primary education or lower | 694 (73.6) |
| Secondary or higher | 249 (26.4) |
| Stable partner | 688 (73.0) |
| No stable partner | 255 (27.0) |
| Unstable income | 812 (86.1) |
| Stable income (formal employment) | 131 (13.9) |
| Registered health system users | 889 (94.3) |
| Non-registered users | 54 (5.7) |
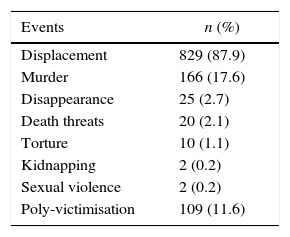
As regards the victimising events, rates of 0.2% were observed for kidnapping and sexual violence, with forced displacement reaching 87.9% (Table 2).
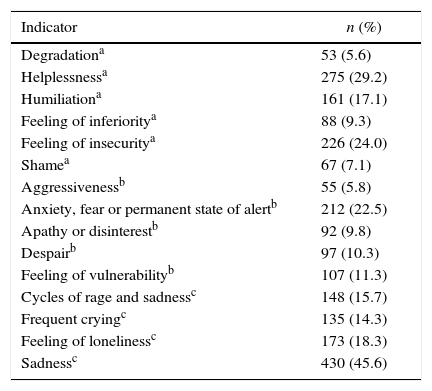
The indicators of emotional suffering ranged from 5.6% feeling degradation to 45.6% sadness (Table 3).
Indicators of emotional distress.
| Indicator | n (%) |
|---|---|
| Degradationa | 53 (5.6) |
| Helplessnessa | 275 (29.2) |
| Humiliationa | 161 (17.1) |
| Feeling of inferioritya | 88 (9.3) |
| Feeling of insecuritya | 226 (24.0) |
| Shamea | 67 (7.1) |
| Aggressivenessb | 55 (5.8) |
| Anxiety, fear or permanent state of alertb | 212 (22.5) |
| Apathy or disinterestb | 92 (9.8) |
| Despairb | 97 (10.3) |
| Feeling of vulnerabilityb | 107 (11.3) |
| Cycles of rage and sadnessc | 148 (15.7) |
| Frequent cryingc | 135 (14.3) |
| Feeling of lonelinessc | 173 (18.3) |
| Sadnessc | 430 (45.6) |
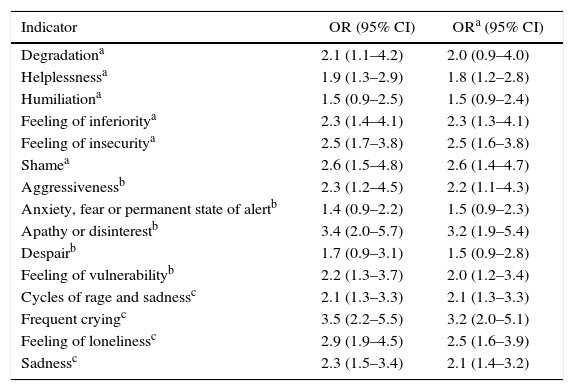
The gross and adjusted associations of poly-victimisation and the indicators studied are shown in Table 4. All adjustments showed adequate Hosmer–Lemeshow goodness-of-fit.
Association between poly-victimisation and emotional distress (gross and adjusted).
| Indicator | OR (95% CI) | ORa (95% CI) |
|---|---|---|
| Degradationa | 2.1 (1.1–4.2) | 2.0 (0.9–4.0) |
| Helplessnessa | 1.9 (1.3–2.9) | 1.8 (1.2–2.8) |
| Humiliationa | 1.5 (0.9–2.5) | 1.5 (0.9–2.4) |
| Feeling of inferioritya | 2.3 (1.4–4.1) | 2.3 (1.3–4.1) |
| Feeling of insecuritya | 2.5 (1.7–3.8) | 2.5 (1.6–3.8) |
| Shamea | 2.6 (1.5–4.8) | 2.6 (1.4–4.7) |
| Aggressivenessb | 2.3 (1.2–4.5) | 2.2 (1.1–4.3) |
| Anxiety, fear or permanent state of alertb | 1.4 (0.9–2.2) | 1.5 (0.9–2.3) |
| Apathy or disinterestb | 3.4 (2.0–5.7) | 3.2 (1.9–5.4) |
| Despairb | 1.7 (0.9–3.1) | 1.5 (0.9–2.8) |
| Feeling of vulnerabilityb | 2.2 (1.3–3.7) | 2.0 (1.2–3.4) |
| Cycles of rage and sadnessc | 2.1 (1.3–3.3) | 2.1 (1.3–3.3) |
| Frequent cryingc | 3.5 (2.2–5.5) | 3.2 (2.0–5.1) |
| Feeling of lonelinessc | 2.9 (1.9–4.5) | 2.5 (1.6–3.9) |
| Sadnessc | 2.3 (1.5–3.4) | 2.1 (1.4–3.2) |
95% CI: 95% confidence interval; OR: odds ratio; ORa: odds ratio adjusted for age, sex, education, stable partner, employment and registration with the health system.
Similarly, in the process of reducing the manifestations of emotional suffering by means of factor analysis, poly-victimisation showed a statistically significant association with manifestations of perceived discrimination (OR=1.3, 95% CI, 1.1–1.5), anxiety-stress (OR=1.3, 95% CI, 1.1–1.5) and depressive symptoms (OR=1.6, 95% CI, 1.3–1.9).
DiscussionThis study shows that 11.6% of the victims of the internal armed conflict in the Department of Magdalena, Colombia, report poly-victimisation. Poly-victimisation was statistically associated with greater emotional suffering (perceived discrimination, depression and anxiety) than victimisation due to a single event.
In this research we found that poly-victimisation was positively associated with manifestations of emotional suffering, reported as symptoms related to depression and anxiety-stress. These findings are entirely consistent with previous studies conducted in other contexts, which indicated that people with poly-victimisation presented more distress or emotional symptoms on the spectrum of anxiety, depression and stress than those who reported victimisation due to a single event.10–15,31–34 For example, Cuevas et al. observed in a group of 870 women that experiencing poly-victimisation significantly increased the proportion of clinically significant symptoms more than any specific form of violence or a single incident of victimisation.35 Moreover, Hunt et al. showed, in a group of 66 refugees who requested mental health services, that those who reported several traumatic events presented symptoms of anxiety, depression and post-traumatic stress more frequently than the group that reported a single event of victimisation.36
In this study, it was also observed that poly-victimisation is associated with greater perceived discrimination than victimisation due to a single event. There are no previous studies reporting this association. Nonetheless, it should be taken into account that the victims of the Colombian armed conflict experienced a process of discrediting, the so-called stigma-discrimination complex, generally secondary to the displacement situation.23,37,38 The stigma-discrimination complex in itself not only represents a further stressor for the victims of the armed conflict,23 but also multiplies the chances of them presenting symptoms related to post-traumatic stress disorder subsequent to an additional victimising event.13 It should also be borne in mind that the stigma-discrimination complex, for any condition, trait or situation, represents an access barrier to health services even when the need for services is completely manifest.39
Given that Colombia is moving towards a post-conflict period, comprehensive psychosocial care is needed for all victims of the internal armed conflict, not only with the objective of responding to emotional suffering, but also to break the cycles of violence that culminate in poly-victimisation.40,41 It is also essential to stop the spiral that leads to the poverty and re-victimisation of these groups42–44 and to thus promote individual, family and collective wellbeing, based mainly on community actions.40,45,46 Undoubtedly, caring for victims of an armed conflict is a major challenge for any health system, given the complexity resulting from the intertwining of complex humanitarian and social phenomena that require integrated cross-sector actions.47,48 PAPSIVI must incorporate one additional element to the differential treatment of people in a situation of poly-victimisation.21,24 This is even more true when a significant number of the internal armed conflict victims belong to ethnic, Afro-Colombian and indigenous communities, who face inequalities when it comes to exercising their rights as citizens.49
This research has the strength of qualitatively presenting the association between poly-victimisation and emotional suffering in victims of the internal armed conflict in Colombia. In addition, an advanced statistical analysis was carried out to quantify the associations, which is very rare or exceptional in the reports published by state organisations. However, this analysis has a limitation that is typical of studies that do not employ probability sampling to apply the observations to populations with similar or comparable characteristics.50 The research presents another disadvantage, characteristic of cross-sectional analyses that do not reveal an unambiguous line of causality, of a cause and effect relationship.51 Moreover, for the analysis it was necessary to exclude a significant percentage of the interviewees; however, given that there was a large sample of around 1000 participants, it is possible to minimise several probable biases or errors that could occur due to this loss of information.52
It is concluded that poly-victimisation is a phenomenon experienced by approximately 1 in 10 victims of the internal armed conflict in the Department of Magdalena. Poly-victimisation is associated with greater emotional suffering than victimisation due to a single event. Poly-victimisation should be considered in the comprehensive psychosocial and health care of the victims. Further research is needed in this area during the post-conflict period.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflicts of interestThe authors have no conflicts of interest to declare.
To Dr Patricia Serrano, Victims Coordinator, PAPSIVI Magdalena, for kindly obtaining information on the victims.
Please cite this article as: Campo-Arias A, Sanabria AR, Ospino A, Guerra VM, Caamaño BH. Polivictimización por el conflicto armado y sufrimiento emocional en el Departamento del Magdalena, Colombia. Rev Colomb Psiquiat. 2017;46:147–153.
