



Rather than focusing on the extensively studied social perception and recognition impairments in people with schizophrenia, this study focuses on the type of social information considered relevant by people with schizophrenia, and how they use it to arrive at conclusions about social situations.
MethodsParticipants included 50 outpatients with schizophrenia from the Hospital del Salvador at Valparaíso, Chile, and 50 healthy comparators matched by age and gender. Subjects completed the Social Information Preference Test (SIPT), which presents scenes depicting ambiguous social situations with faces, thoughts, and facts about the scene hidden from view. Participants were required to select a limited number of these items and then choose between possible interpretations of the scene (positive, neutral, or negative). Additionally, they are asked to provide a feeling of certainty in their answers, using a 7-point visual analogue scale.
ResultsPeople with schizophrenia, as well as controls had a strong preference for knowing the thoughts of the characters. Both groups were least likely to choose emotional expressions. Patients were significantly less likely to choose object/information than controls. Both groups showed a high certainty in their responses and no tendency to choose negative interpretations. Limitations: compensated clinical status of the patients may have influenced the results.
ConclusionsThe results of this study suggest that, despite difficulties perceiving clues about the mental state of others, people with schizophrenia use this information to make sense of social situations, and apparently, they do not have problems in understanding social interactions.
En lugar de los impedimentos en la percepción social, ampliamente estudiada en personas con esquizofrenia, centramos nuestra investigación en el tipo de información social considerada relevante por las personas con esquizofrenia y cómo la usan para llegar a conclusiones sobre situaciones sociales.
MétodosSe incluyó a 50 pacientes ambulatorios con esquizofrenia del Hospital del Salvador en Valparaíso, Chile, y 50 comparadores sanos, emparejados por edad y sexo. Los sujetos completaron la Prueba de Preferencia de Información Social (SIPT), que presenta escenas con situaciones sociales ambiguas en las que rostros, pensamientos y hechos sobre la escena están ocultos a la vista. Los participantes deben seleccionar un pequeño número de estos elementos y luego elegir entre posibles interpretaciones (positiva, neutral o negativa). Además, se les pide que proporcionen una sensación de certeza en sus respuestas, utilizando una escala analógica visual de 7 puntos.
ResultadosTanto las personas con esquizofrenia como los comparadores mostraron una fuerte preferencia por conocer los pensamientos de los personajes. La opción menos preferida por ambos grupos fue las expresiones emocionales, mientras que los pacientes escogieron menos objeto/información que los controles. Ambos grupos mostraron una alta certeza en sus respuestas y no se observó una tendencia a elegir interpretaciones negativas. Limitaciones: el estado clínico compensado de los pacientes puede haber influido en los resultados.
ConclusionesLos resultados de este estudio indican que, a pesar de las dificultades para percibir pistas sobre el estado mental de los demás, las personas con esquizofrenia usan esta información para dar sentido a las situaciones sociales y, aparentemente, no presentan problemas para comprender las interacciones sociales.
Even after prolonged periods of remission from psychotic symptoms, people with schizophrenia face considerable difficulties in many aspects of everyday life, including employment,1 independent living,2 and community functioning.3 These impairments have profound negative impacts on their overall level of functioning and quality of life.4
Although there is an important degree of overlap with the general cognitive deficit present in schizophrenia,5 the alterations described are usually thought of as consequences of a more specific deficit in social cognition6,7 or to construct representations of the relation between oneself and others and flexibly use these representations to guide social behaviour.8
Social cognition is a set of interrelated but separable skills or domains. Following the definitions of initiatives such as MATRICS9 and CNTRICS,10 the most commonly described social cognitive deficits in schizophrenia are impairments in emotion perception, social perception/knowledge, the theory of mind, and attributional style.
Briefly, emotion perception is being able to identify the emotions of others accurately; social perception/knowledge refers to the ability to perceive, understand, and appraise social roles, rules, and context; theory of mind is the ability to interpret someone's speech or actions in terms of their intentions; and attributional style is the usual mode of explaining events as consequence of internal (personal), external (other person), or situational factors.11
All the above has been extensively studied in schizophrenia. According to published research, patients exhibit impaired recognition of emotions conveyed both through facial expressions and verbal communication.12 They also have problems representing affective but not simpler cognitive mental states, although some individuals, especially those with predominantly paranoid symptoms, may actually overmentalize.13
Attributional style refers to the particular ways in which individuals explain the causation of events. People with schizophrenia, especially those with delusions, exhibit reasoning anomalies such as abnormal data gathering or jumping-to-conclusions, which may lead subjects to arrive at conclusions despite insufficient evidence.14 Impaired attributional biases may lead patients to explain their negative experiences as being caused by others rather than by themselves15 or by few rather than by many factors.16
Besides recognising emotional cues and adequately attributing causation of events, social cognition also requires being aware of the characteristics of the social context in which they occur. Though somewhat less studied than the previously mentioned domains, research has shown that people with schizophrenia are less sensitive to the more abstract cues in social situations;17 they lack information about appropriate conduct18 and have difficulties processing social schemes.19
Focus on impairments of specific components of social cognition is helpful to understand the elements that constitute deficits in social and interpersonal functioning observed in people with schizophrenia. However, some authors claim that this approach cannot clarify whether these deficits are specific or part of a global perceptual and cognitive problem.
Other researchers argue that social cognition cannot be addressed by dividing the gestalt into subcomponents and recommend a more comprehensive method of study. These authors distinguish between basic “molecular” or perceptual deficits and “molar” deficits, including inefficient use of social scripts and schemes to organise the information perceived in social situations as well as difficulties understanding the actions, roles, rules, and goals involved.20
Instead of focusing on the extensively studied emotion perception and recognition impairments,21,22 we centred our research on the type of social information that is considered relevant by people with schizophrenia and how it is used to arrive at conclusions about social situations. Rather than examining separate deficits, we were interested in a more “molar” study addressing the selection and processing of information in a group of well-stabilised outpatients treated at the Hospital del Salvador in Valparaíso, Chile.
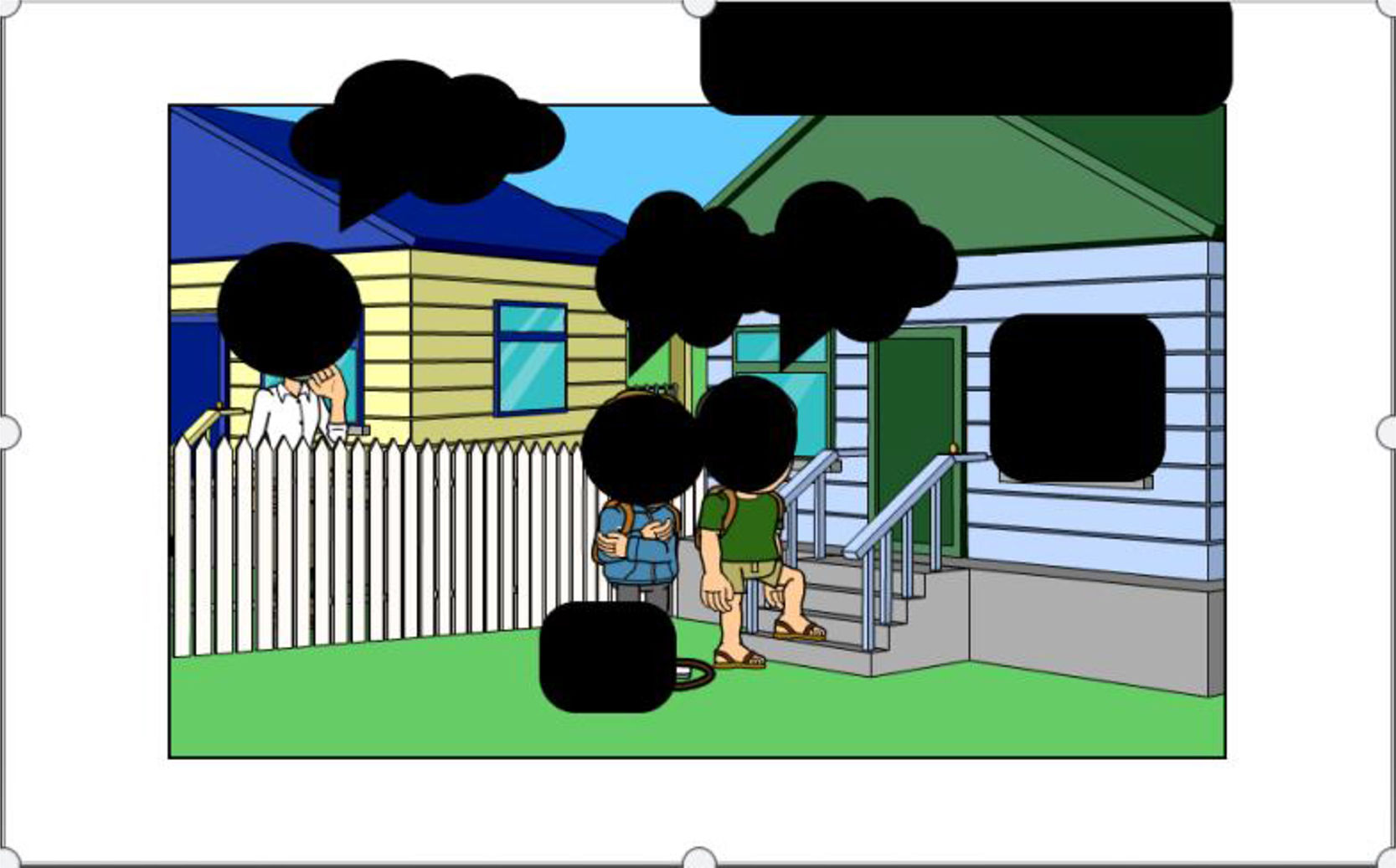
The Social Information Preference Test (SIPT), part of the EMOTICOM battery, presents participants with scenes depicting ambiguous social situations in which faces (feelings), thoughts, and facts about the scene are hidden from view (figure 1). Participants are required to select a limited number of these items and then choose between three possible interpretations of the scene (positive, neutral, or negative), thus allowing evaluation of how a social situation is perceived, the type of information used to resolve its ambiguity, and possible cognitive bias.23 Rather than assessing whether participants have Theory of Mind ability, this newly developed task assesses the extent to which people choose to use this type of information.

Based on the descriptions of difficulties in social perceptions in people with schizophrenia, including reading expressions and minds, we anticipate that patients will choose fewer faces and thoughts items than the comparison group. Also, due to deficits in the ability to appraise complex social schemata and attributional biases, we expect them to differ from the comparison group in their selection of interpretations of the social situations exhibited.
Subjects and MethodsDesign: cross-sectional study.
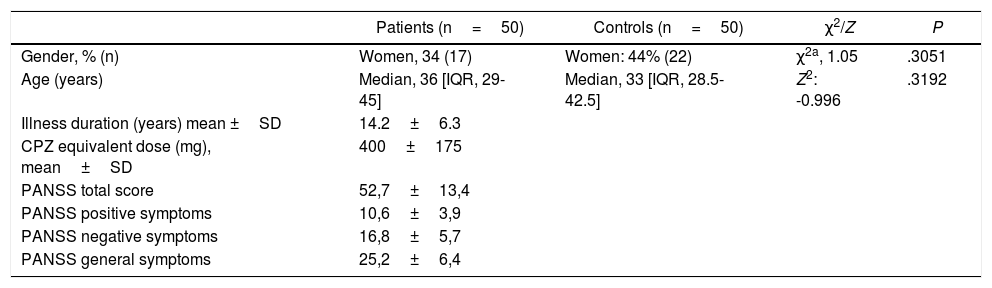
ParticipantsThe patient sample included 50 individuals with schizophrenia recruited from the outpatient clinic of the Hospital del Salvador at Valparaíso, Chile. All patients met DSM-524 criteria for a lifetime diagnosis of schizophrenia and were well stabilised and receiving treatment with psychotropic medication. Exclusion criteria included comorbid organic brain disease, severe medical disease, and lifetime substance abuse disorder (Table 1).
Demographic and clinical data for patients and controls.
| Patients (n=50) | Controls (n=50) | χ2/Z | P | |
|---|---|---|---|---|
| Gender, % (n) | Women, 34 (17) | Women: 44% (22) | χ2a, 1.05 | .3051 |
| Age (years) | Median, 36 [IQR, 29-45] | Median, 33 [IQR, 28.5-42.5] | Z2: -0.996 | .3192 |
| Illness duration (years) mean ±SD | 14.2±6.3 | |||
| CPZ equivalent dose (mg), mean±SD | 400±175 | |||
| PANSS total score | 52,7±13,4 | |||
| PANSS positive symptoms | 10,6±3,9 | |||
| PANSS negative symptoms | 16,8±5,7 | |||
| PANSS general symptoms | 25,2±6,4 |
IQR: interquartile range.
Fifty subjects, matched by age and gender, were recruited through community advertising and acted as a comparison group. Individuals were excluded if they had a history of past or present psychiatric disorder or if any first-degree relatives had been diagnosed with a severe mental disorder.
The study protocol was explained to all participants, and written informed consent was obtained. The study was approved by the Ethics Committee of Valparaíso-San Antonio Public Health Service.
Clinical evaluationA psychiatrist assessed symptom severity with a semi-structured interview using the Spanish version of the PANSS25 on a 7-point scale considering positive and negative subscales and total score.
Experimental taskParticipants completed the Social Information Preference Test programmed in PsychoPy26 on a touchscreen laptop (Dell Inspiron 11, series 300). The task was administered in a quiet testing room over 15-20min.
The Social Information Preference Test (figure 1, sample scene) assesses information sampling in socially ambiguous situations. Participants are shown 18 scenes with three faces, three thoughts, and three facts about the scene hidden from view. Participants must select four out of nine pieces of information to resolve the ambiguity of each scene, choosing between three possible outcomes of the situation (negative, positive, or neutral), thus providing a measure of interpretational bias. All outcomes are equally possible, thus allowing variation of responses. Additionally, participants are asked to provide a feeling of certainty in their answers using a 7-point visual analogue scale. There is no time restriction for the task.
Statistical AnalysisNormality of data distribution was determined using the Shapiro-Wilkinson test and histograms. Results are described with measures of central tendency (mean or median) for parametric and dispersion (standard deviation or interquartile range) for non-parametric variables. The association between qualitative variables was examined with χ2. Associations between quantitative and dichotomous variables were analysed with student T-test for parametric variables and the Mann-Whitney U test for non-parametric. For two quantitative variables, the Pearson test was used for normal variables and the Spearman test for non-parametric. Finally, a multivariate analysis was performed with the dependent variables that had differences between the two groups (object and response time), and the independent variables included in the study (age, gender and group). All data were analyzed using Stata 15 software. Statistical significance was considered with P<.05.
ResultsBoth groups are comparable in terms of age and gender. The group of patients was 34% females, with a median age of 36 years, while the comparison group was 44% females with a median age of 33 years.
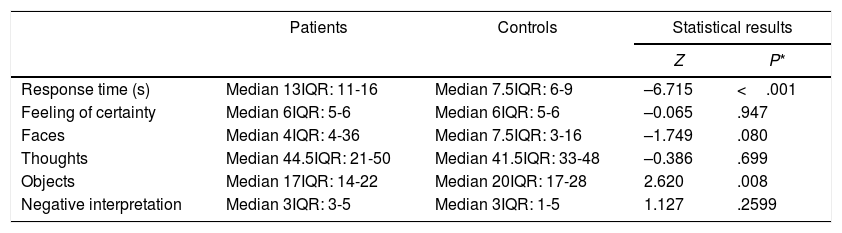
Performance on the Social Information Preference Test did not follow a normal distribution, so differences between patients and controls were analysed with the Mann-Whitney's U test. As expected, the patients took significantly longer to respond than controls, with a median of 13 vs. 7.5 s. However, the feeling of certainty in the answers is equal in both groups, with a median of 6, which is considered high (maximum 7).
When comparing the proportion of the clues thoughts, faces, and objects chosen by the subjects of the patient group and the control, no significant differences were observed in the first two categories (Table 2). A particular category can be selected 54 total times (3 times in each of the 18 scenes); thoughts was chosen most frequently by both controls (41 out of 54 choices) and patients (44 out of 54 choices). The item least chosen by both groups was faces, with medians of 7.5 and 4 for controls and patients, respectively. The only statistically significant difference found between the two groups of participants was the frequency of selection of the item objects. In both groups, it was the second most frequent choice, but the number of selected items was significantly higher in the comparator group, with a median of 20 vs. 17 (P=.008).
Results of the comparison of Social Information Preference Test data between patients and controls.
| Patients | Controls | Statistical results | ||
|---|---|---|---|---|
| Z | P* | |||
| Response time (s) | Median 13IQR: 11-16 | Median 7.5IQR: 6-9 | –6.715 | <.001 |
| Feeling of certainty | Median 6IQR: 5-6 | Median 6IQR: 5-6 | –0.065 | .947 |
| Faces | Median 4IQR: 4-36 | Median 7.5IQR: 3-16 | –1.749 | .080 |
| Thoughts | Median 44.5IQR: 21-50 | Median 41.5IQR: 33-48 | –0.386 | .699 |
| Objects | Median 17IQR: 14-22 | Median 20IQR: 17-28 | 2.620 | .008 |
| Negative interpretation | Median 3IQR: 3-5 | Median 3IQR: 1-5 | 1.127 | .2599 |
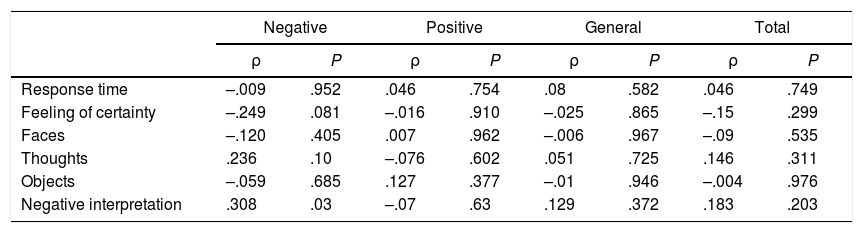
We next considered affective bias in the interpretation of the scene. Contrary to what was expected, patients did not show a preference for the negative options, which were selected by both groups on an identical and low number of occasions (3). Finally, results were mostly unaffected by patients’ symptoms, the only exception being a greater tendency to select negative interpretations in patients with more severe negative symptoms (Table 3).
Correlations between SIPT and PANSS.
| Negative | Positive | General | Total | |||||
|---|---|---|---|---|---|---|---|---|
| ρ | P | ρ | P | ρ | P | ρ | P | |
| Response time | –.009 | .952 | .046 | .754 | .08 | .582 | .046 | .749 |
| Feeling of certainty | –.249 | .081 | –.016 | .910 | –.025 | .865 | –.15 | .299 |
| Faces | –.120 | .405 | .007 | .962 | –.006 | .967 | –.09 | .535 |
| Thoughts | .236 | .10 | –.076 | .602 | .051 | .725 | .146 | .311 |
| Objects | –.059 | .685 | .127 | .377 | –.01 | .946 | –.004 | .976 |
| Negative interpretation | .308 | .03 | –.07 | .63 | .129 | .372 | .183 | .203 |
Spearman test, P≤.05.
Finally, a multivariate analysis was performed with the dependent variables that were significantly different between the two groups (object item and response time). All independent variables were initially included (age, gender and group), but were withdrawn if they did not contribute to the strength of the model. Age and group remained in the covariance analysis (ANCOVA) of the variable object. The group variable is significant (P=.0021) with a coefficient of –3.61 for patients (95%CI, –6.67 to –0.55), the age variable also significantly predicts the selection of the object item (P=.039) with a coefficient of –0.18 (95%CI, –-0.34 to –0.009). The total model is significant, with P=.005, and predicts the object variable at 8% (R adj=.0854). For the response time variable, an ANCOVA was performed, also including age and group, the model was significant (P=.000) and predicted the dependent variable at 42.6% (R adj=.426). The influence of the group was statistically significant (P<.01) with a coefficient for patients of 5.22 (95%CI, 3.86-6.58) and age was also significant (P=.002) with a coefficient of 0.11 (95%CI, 0.04-0.194).
DiscussionThe main objective of the Social Information Preference Test is to examine the type of information that people use to solve ambiguous social situations. Unexpectedly, in our study, people with schizophrenia did not differ from controls in their selection of information; both groups had a strong preference for knowing the thoughts of the characters in the cartoon and were least likely to choose emotional expressions. Also, patients were significantly less likely to choose factual information than comparisons.
Although patients might have found the task slightly more complicated based on their longer response time, both groups showed the same degree of certainty in their responses. Contrary to expectations, patients did not show a greater tendency than controls to choose negative interpretations of the scenes. Although we could not find evidence of an association between the severity of psychotic symptoms and attributional bias, the negative interpretations were associated with the scores on the subscale of negative symptoms. These results are consistent with other reports27–29 and point to a more emotional explanation of attributional biases.
Social cognition comprises different processes, such as the representation, attribution, and application of mental states. Unlike most investigations, the task used in this research did not require recognition or identification of emotions or mental states since this was readily available upon selection. Instead, subjects were asked to apply this information to clarify an ambiguous situation. The results suggest that people with schizophrenia may have a broadly unimpaired theory of mind in first order tasks30 or in tasks that require the representation of cognitive rather than affective information.31 It is possible, however, that the compensated clinical status of the patients has influenced the results.
There is ample evidence of a deficit in social cognition in people with schizophrenia, especially in emotional and perceptive aspects,21,22,32,33 with less being known about more cognitive demands such as social knowledge. The fact that patients in our investigation selected similar information and interpreted the scenes in the same way as controls may imply that they have a preserved understanding of the roles and rules of social interactions, lending support to more focussed social cognition interventions for people with schizophrenia.34 Finally, our results highlight the existence of different processes involved in social cognitive functioning and the need to understand their alteration in schizophrenia as a continuum with different interindividual competences and performances.13
Conflicts of interestThe authors have no conflicts of interest to declare.
