





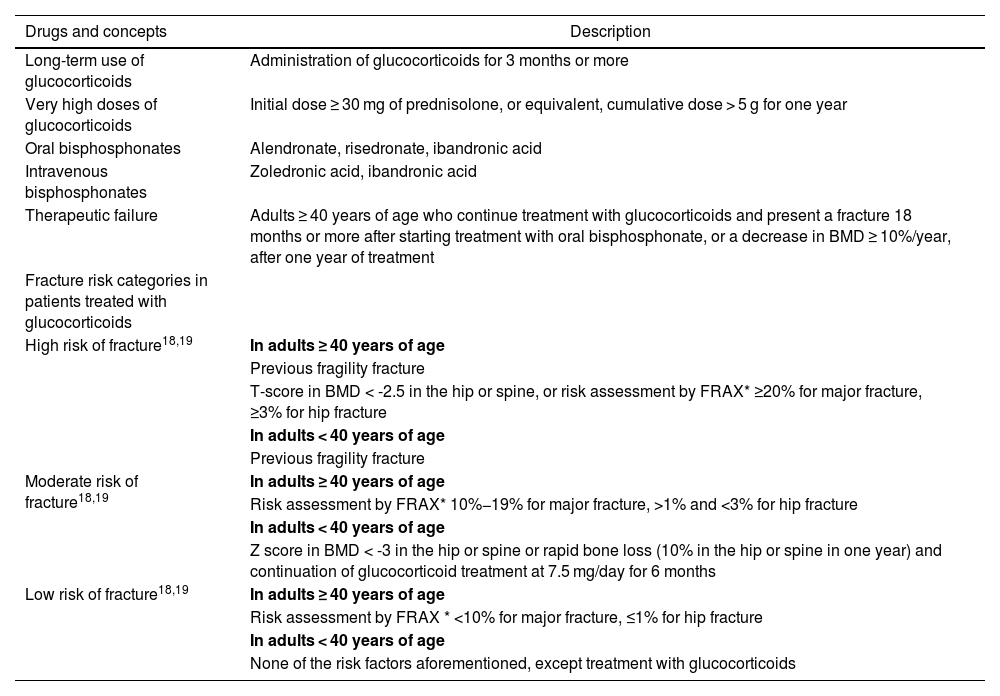
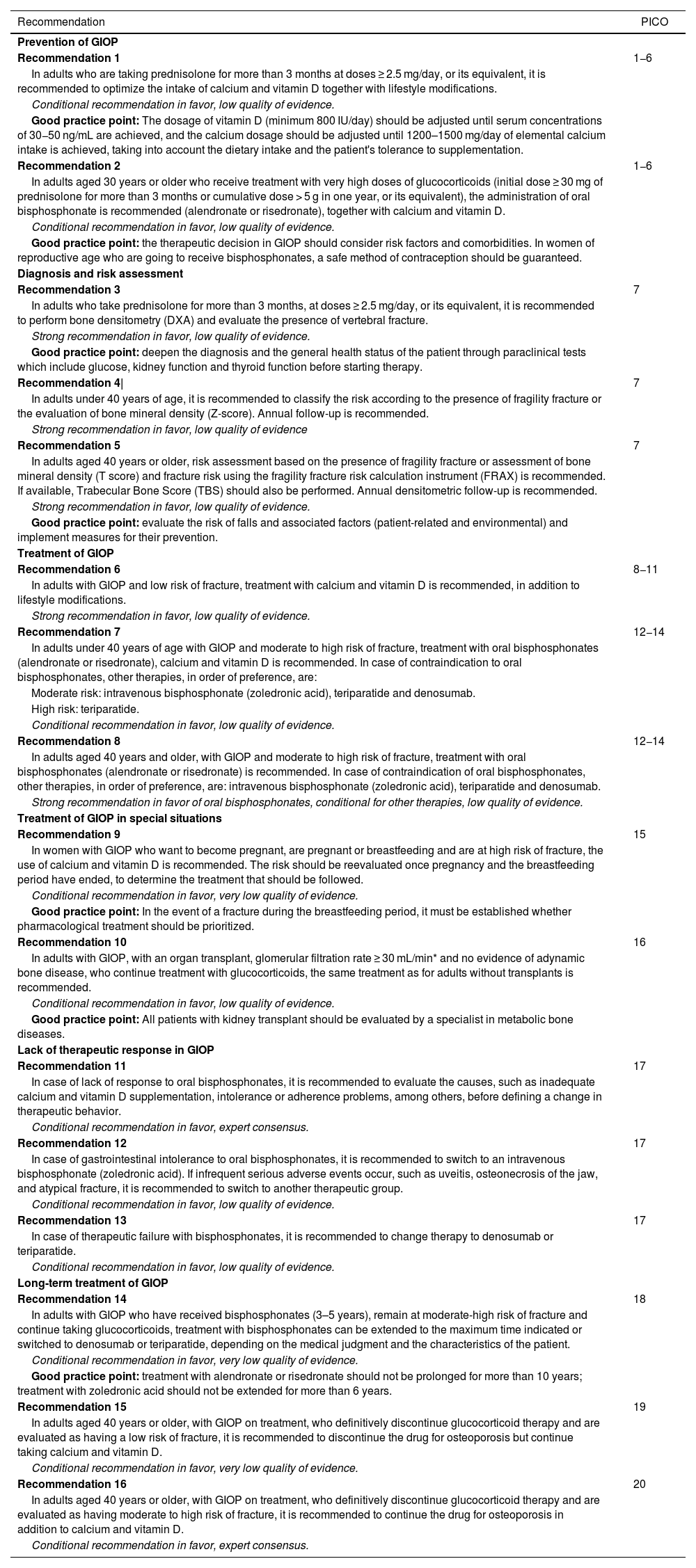
The use of glucocorticoids is the most frequent cause of osteoporosis and osteoporotic fractures. Considering that glucocorticoid-induced osteoporosis (GIOP) is an underestimated and generally untreated problem, the Bone Metabolism study group of the Colombian Association of Rheumatology decided to create this Clinical Practice Guideline (CPG) in order to support rheumatologists and other specialists in the country who use this type of medication to manage inflammatory and autoimmune conditions, with recommendations on prevention, diagnosis, and treatment of GIOP. The recommendations presented here were constructed following the GRADE-ADOLOPMENT methodology. The American College of Rheumatology guideline, Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis, was selected as the source for updating the literature searches. The development of this CPG also included the participation of clinical experts from different specialties, patients, and the EpiThink Health Consulting technical-methodological team.
El uso de glucocorticoides es la causa más frecuente de osteoporosis y fracturas osteoporóticas. Puesto que la osteoporosis inducida por glucocorticoides (OIG) es un problema subestimado y generalmente no tratado, el grupo de estudio de Metabolismo Óseo de la Asociación Colombiana de Reumatología decidió elaborar esta guía de práctica clínica (GPC), con el fin de apoyar a los reumatólogos y a otros especialistas del país que usan este tipo de medicamentos para el manejo de condiciones inflamatorias y autoinmunes, con recomendaciones sobre prevención, diagnóstico y tratamiento de la OIG. Las recomendaciones aquí planteadas se construyeron siguiendo la metodología Grade-Adolopment. Se seleccionó la guía del Colegio Americano de Reumatología, Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis, como fuente para la actualización de las búsquedas de la literatura. El desarrollo de esta GPC contó además con la participación de expertos clínicos de diferentes especialidades, pacientes y el equipo técnico metodológico de EpiThink Health Consulting.
