



Connections are common communications between 2 similar anatomical elements. Some of the most common are in the forearm between the median and ulnar nerves and are clinically important because they produce variations in motor and sensory innervation and can cause confusion when diagnosing peripheral nerve pathology.
MethodDescriptive, cross-sectional, observational study. A total of 127 patients older than 18 years were studied, electromyography was performed on the upper limbs and the frequency of presentation of the connections was obtained.
ResultThe Riche-Cannieu connection was present in 16.5% of the total patients studied, of which 42.9% presented in the left arm and 89.3% in isolation. The Marinacci connection was the second in frequency with 15.7%, of which 40% was presented in the left arm and 45.8% coexisted with another connection. The Berrettini connection was the third in frequency with 9.4%, 50% presented in the left arm and 53.3% of the sample was found in isolation. Martin-Grüber's connection was the least frequent at 7.1% of our cases, of which 44.5% presented bilaterally and 90% associated with another connection.
ConclusionIt is concluded that of the 4 types of connection studied the most frequent in our environment was the Riche-Cannieu with predominance of the left arm and in isolation.
Las conexiones son uniones frecuentes entre 2elementos anatómicos similares. En el antebrazo, entre los nervios mediano y cubital se presentan algunas de las más comunes, las cuales tienen importancia clínica debido a que producen variaciones en la inervación motora y sensitiva que pueden crear confusiones al momento de diagnosticar alguna enfermedad del nervio periférico.
MétodoEstudio descriptivo, transversal, observacional. Se estudió a un total de 127 pacientes mayores de 18 años, se les realizó electromiografía en miembros superiores y se obtuvo la frecuencia de presentación de las conexiones.
ResultadoLa conexión de Riche-Cannieu se presentó en un 16,5% del total de los pacientes estudiados. De estos, en un 42,9% se presentó en el brazo izquierdo y el 89,3% de forma aislada. La conexión de Marinacci fue la segunda en frecuencia, con un 15,7% de los casos, de los cuales un 40% se presentó en el brazo izquierdo y el 45,8% coexistía con otra conexión. La conexión de Berrettini fue la tercera en frecuencia con el 9,4%: el 50% se presentó en el brazo izquierdo y en un 53,3% de la muestra se halló de forma aislada. La conexión de Martin-Grüber fue la menos frecuente, con un 7,1% de nuestros casos, de los cuales el 44,5% se presentó de forma bilateral y el 90% asociado con otra conexión.
ConclusiónSe concluye que, de los 4tipos de conexión estudiados, la más frecuente en nuestro medio es la conexión de Riche-Cannieu con predominio del brazo izquierdo y de forma aislada.
Communications, earlier called anastomoses,1 are connections between 2 similar anatomical elements. They frequently occur in human beings, so they should be considered an anatomical variant and not an anomaly. Some of the most frequently described nerve communications are found in the forearm and hand between the median and ulnar nerves; these connections are very clinically significant because they produce variations in motor and sensory innervation of the hand, variations that can lead to confusion when evaluating the function of these structures.2–5
Throughout history, communications have been described as communication branches between the median and the ulnar nerves. They were first noted in the illustrations by Berrettini (1741), while later authors such as Martin (1763), Grüber (1870), Brooks (1886), Spourgitis (1895), Riche (1897) and Gehwolf (1921) detailed them based on anatomical dissections. That is why these anastomoses are named after the first to characterise them. In 1966 Mannerfeld was the first to use electrophysiology to detect these connections.6
Communications can be found at any point in the nerve path, whether at the elbow or below it, in the distal or proximal forearm or in the palm. Consequently, the forearm communication branches that emerge from the median to the ulnar nerves are called Martin-Grüber communications (MGCs), mainly involving motor fibres; and the ulnar to median nerve connection by nerve fibres is called the Marinacci communication (MC). In the palm of the hand, the connection between the recurrent branch of the median nerve and the deep branch of the ulnar nerve, with motor fibres, is called the Riche-Cannieu communication (RCC); likewise, the palm communication of the common digital nerves of the superficial ulnar and median nerves, which carries sensory fibres, is called the Berrettini communication (BC).5,7,8
In the Joyeeta et al.8 metaanalysis in Poland, a prevalence of 19.5% was found for MGC, 0.7% for MC, 55.5% for RCC and 60.9% for BC. These researchers also found that MGC is most commonly present unilaterally (66.8%), in the right side (15.7%), following an oblique path (84.8%) and originating in the anterior interosseous nerve with a prevalence of 57.6%. According to other studies, MGC incidence ranges from 15% to 54%, without a significant difference in appearance by sex. Some authors propose that there might be a autosomal dominant hereditary factor involved.7–10 In the study carried out by Rojas et al. in Colombia,7 146 upper limbs were dissected, finding MGC in 56.5%, MC in 6.5%, BC in 90% and RCC in 88% of the cases: their conclusion was that the communications between the median and ulnar nerves are continual and that the finding could serve in other clinical applications. According to the study by Diazgranados et al., RCC has a probable incidence of 59%11; Kimura et al.12 found an incidence of 83.3%, which caused them to indicate that it was more a normal condition than an anatomical variant.8,11,13 According to several studies, the frequency of BC presentation varies considerably and the BC is thought to be from an anatomical variant to a normal finding.5,14 Finally, we can say that MC is considered to be rare: based on various studies, its frequency varies from 1% to 16.7%.8,15
The variability in the indications of frequency of the different communications, the possibility that there might be a hereditary factor (and hence racial) in its presentation and the clinical implications of not recognising its presence lead us to the objectives of this study: determining the frequency of the communications of the median and ulnar nerves in our population using electromyography, as well as evaluating whether there are differences based on sex or on laterality of location in the upper limbs.
Material and methodThis was a descriptive, observational, cross-sectional study carried out in Lima (Peru). As our hospital is third-level and a centre of reference for part of the population outside the capital, evaluating a representative population sample is possible. We included all patients aged 18 years and older of both sexes sent to Neurophysiology at the Hospital Nacional Arzobispo Loayza, from February to July 2016, for upper limb electromyographic study, regardless of the underlying condition. Patients with a serious nerve lesion that would prevent assessing the nerve communications were excluded. Almost all patients seen in that time period were seen, except for those who could not tolerate the procedure.
Standard electromyography equipment (Nihon Kohden Neuropack M, Japan) was used. The study motor was performed stimulating both the median and ulnar nerves, distally and proximally. The motor unit potentials in the abductor brevis thumb muscle, the digiti minimi fifth finger muscle and the first dorsal interosseous muscle were evaluated.
The sensory study involved stimulating the distal medial nerve and evaluating the second finger. For the ulnar nerve, the third and fifth fingers were evaluated. It should be mentioned that some of these evaluations are not routine and were performed to verify the whether the communications mentioned were present.
Data analysis was carried out using the Microsoft Excel 2013 program, together with IBM SPSS Statistics 20. Non-parametric Mann–Whitney tests were used to determine the relevance between the sexes.
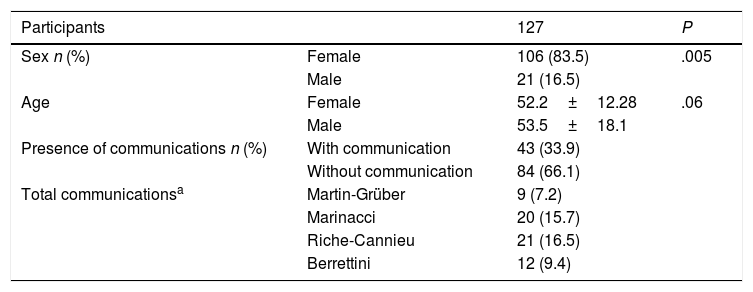
ResultsA total of 127 patients participated in this study (Table 1), of which 106 (83.5%) were females and 21 (16.5%) were males (P<.005). Age at diagnosis had a range of 53.5±18.1 for the males and of 52.2±12.28 for the females (P<.06). Of the 127 individuals studied, 43 (33.9%) presented some form of nerve communication, while 84 (66.1%) participants had no communications.
Characteristics studied in the total population.
| Participants | 127 | P | |
|---|---|---|---|
| Sex n (%) | Female | 106 (83.5) | .005 |
| Male | 21 (16.5) | ||
| Age | Female | 52.2±12.28 | .06 |
| Male | 53.5±18.1 | ||
| Presence of communications n (%) | With communication | 43 (33.9) | |
| Without communication | 84 (66.1) | ||
| Total communicationsa | Martin-Grüber | 9 (7.2) | |
| Marinacci | 20 (15.7) | ||
| Riche-Cannieu | 21 (16.5) | ||
| Berrettini | 12 (9.4) |
Statistical significance: P<.05; Mann–Whitney U.
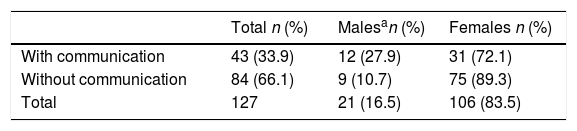
Of the 127 patients studied, 21 (16.5%) were male (Table 2): 12 of them presented some type of communication, while 9 had no communication. Females constituted 106 patients (83.5%), of which 31 women presented some type of communication and 75 had none. The great difference in between the sexes was due to the fact that women were referred mainly for upper limb studies, especially for carpal tunnel study. It seems that men do not come for evaluation of more minor symptoms such as paresthesias, they wait until the symptoms are severe and cause pain or occupational disability.15,16
Communication frequency according to sex.
| Total n (%) | Malesan (%) | Females n (%) | |
|---|---|---|---|
| With communication | 43 (33.9) | 12 (27.9) | 31 (72.1) |
| Without communication | 84 (66.1) | 9 (10.7) | 75 (89.3) |
| Total | 127 | 21 (16.5) | 106 (83.5) |
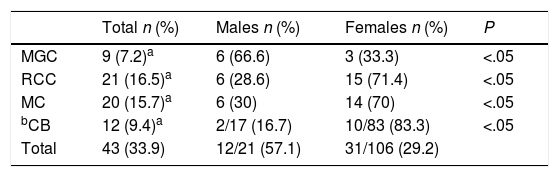
Our findings included the frequency of each type of communication (Table 3). The most frequent was the RCC, with 21 patients (16.5%) of the 127 studied; of these, 15 (71.4%) were females and 6 (28.6%), males. The second most frequent was the MC, with 20 individuals (15.7%); of these, 14 (70%) were females and 6 (30%) were males. The third in frequency was the BC, with 12 individuals (9.4%) of a total of 100 patients: 10 (83.3%) were females and 2 (16.7%) were males (the BC communication was not sought in the first cases evaluated, so there were fewer participants than the total of 127). Lastly, MGC was found in 9 people (7.2%): 6 (66.6%) were males and 3 (33.3%), females.
Frequency by type of communication (of the total participants).
| Total n (%) | Males n (%) | Females n (%) | P | |
|---|---|---|---|---|
| MGC | 9 (7.2)a | 6 (66.6) | 3 (33.3) | <.05 |
| RCC | 21 (16.5)a | 6 (28.6) | 15 (71.4) | <.05 |
| MC | 20 (15.7)a | 6 (30) | 14 (70) | <.05 |
| bCB | 12 (9.4)a | 2/17 (16.7) | 10/83 (83.3) | <.05 |
| Total | 43 (33.9) | 12/21 (57.1) | 31/106 (29.2) |
The evaluation is based on the number of individuals with some type of communication, whether it is in one or both upper limbs.
BC, Berrettini communication; MC, Marinacci communication; MGC, Martin-Grüber communication; RCC, Riche-Cannieu communication.
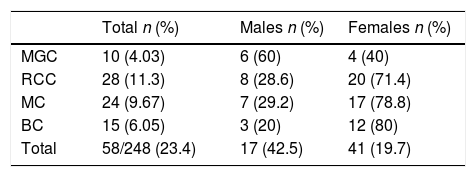
Some studies defined the prevalence of these variants not by case, but by limb studied: we evaluated the communications in this way as well (Table 4). There were 248 upper limbs evaluated (some patients who did not tolerate the procedure received a unilateral assessment): 58 (23.4%) of the limbs presented some type of communication. RCC was found in 28 (11.3%) limbs: 20 (71.4%) in females and 8 (28.6%) in males. The next most frequent communication found was MC, with 24 (9.67%) limbs: 17 (78.8%) in females and 7 (29.2%) in males. This was followed by BC, with 15 (6.05%) limbs: 12 (80%) in females and 3 (20%) in males. Lastly, MGC was found in 10 arms (4.03%).
Frequency by type of communication (of the total limbs).
| Total n (%) | Males n (%) | Females n (%) | |
|---|---|---|---|
| MGC | 10 (4.03) | 6 (60) | 4 (40) |
| RCC | 28 (11.3) | 8 (28.6) | 20 (71.4) |
| MC | 24 (9.67) | 7 (29.2) | 17 (78.8) |
| BC | 15 (6.05) | 3 (20) | 12 (80) |
| Total | 58/248 (23.4) | 17 (42.5) | 41 (19.7) |
The evaluation is based on the number of limbs with a communication, whether or not it is in the same person.
BC, Berrettini communication; MC, Marinacci communication; MGC, Martin-Grüber communication; RCC, Riche-Cannieu communication.
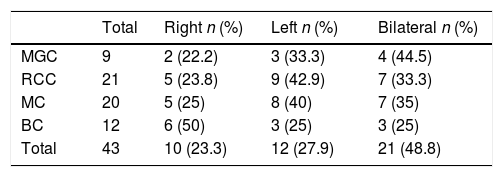
Observing the frequency of the communications according to their laterality (Table 5), 21 (48.8%) communications were bilateral in their presentation, 12 (27.9%) were found in the left arm and 10 (23.3%) in the right arm. In the left arm, RCC predominated, with 9 patients out of a total of 21; followed by MC, with 8 patients of the total of 20 patients with that communication. In the right arm, BC predominated, with 6 patients. Bilaterally, RCC and MC presented in 7 patients each, of a total of 21 and 20 patients studied, respectively.
Communication frequency according to location laterality.
| Total | Right n (%) | Left n (%) | Bilateral n (%) | |
|---|---|---|---|---|
| MGC | 9 | 2 (22.2) | 3 (33.3) | 4 (44.5) |
| RCC | 21 | 5 (23.8) | 9 (42.9) | 7 (33.3) |
| MC | 20 | 5 (25) | 8 (40) | 7 (35) |
| BC | 12 | 6 (50) | 3 (25) | 3 (25) |
| Total | 43 | 10 (23.3) | 12 (27.9) | 21 (48.8) |
BC, Berrettini communication; MC, Marinacci communication; MGC, Martin-Grüber communication; RCC, Riche-Cannieu communication.
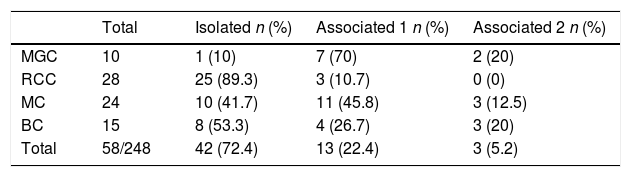
The frequency of communications found together was also analysed (Table 6). Of a total of 58 limbs with communications, 42 (72.4%) were found in isolation, 13 (22.4%) were found associated with another communication and only 3 (5.2%) were associated with 2 different communications. The communication that was most frequently found in association was MGC.
Frequency of associated communications by limb.
| Total | Isolated n (%) | Associated 1 n (%) | Associated 2 n (%) | |
|---|---|---|---|---|
| MGC | 10 | 1 (10) | 7 (70) | 2 (20) |
| RCC | 28 | 25 (89.3) | 3 (10.7) | 0 (0) |
| MC | 24 | 10 (41.7) | 11 (45.8) | 3 (12.5) |
| BC | 15 | 8 (53.3) | 4 (26.7) | 3 (20) |
| Total | 58/248 | 42 (72.4) | 13 (22.4) | 3 (5.2) |
BC, Berrettini communication; MC, Marinacci communication; MGC, Martin-Grüber communication; RCC, Riche-Cannieu communication.
The most frequent communication in our environment was RCC, with 16.5% of the population studied. In the meta-analysis by Joyeeta et al. (in Poland),8 a prevalence of 55.5% was found for RCC, which was the second most prevalent, preceded by BC, with 60.9%. Kimura et al.12 found an incidence of 83% for RCC in their study. Using anatomical dissections in Colombia, Rojas et al.7 found an incidence of 88% for RCC. As for the sex, RCC was more frequent in females; however, we are unable to state that this is true due to the few males in this study. In the study by Nieto et al.17 with 84 hand dissections, 10% were women and 90% were men; the frequency per limb observed was 11.3%, of which 71.4% were females and 28.6% were males. A certain similarity with our study can be seen here, with greater frequency in women and less in men for RCC. As for the frequency according to laterality, we found that 42.9% presented in the left arm, 23.8% in the right and 33.3% bilaterally. Rojas et al.7 found 100% of bilateral cases in their study. The frequency for RCC association with other communications was 89.3% in isolation and 10.7% with an association. We have found no references analysing the superposition of communications in the same limb.
The second most frequent communication was MC, with 15.7% of the patients: of a total of 248 limbs, the frequency per limb was 9.7%, mostly in females. Joyeeta et al.,8 in their meta-analysis, indicate a prevalence of 0.7% for MC, the lowest prevalence in their study. In the study by Meenakshi-Sundaram et al. in India,15 this communication is observed to be more frequent than what other investigators find, with a prevalence of 1.3%. With respect to frequency by sex, we find that 70% of the cases were females. As for laterality of presentation, of the 15.7% that present MC in our study, 40% are located in the left arm, 35% are located bilaterally and 25% are found in the right arm. For Meenakshi-Sundaram,15 of 4 patients with MC, it was bilateral in 3 and only 1 person had an isolated MC, in the right arm. Our findings are that most MC present associated with another type of nerve communication (Table 6).
The third most commonly found communication in our study was the BC, with 9.4% of the cases, or 6.05% of the limbs studied, with predominance of females. In their study, Joyeeta et al.8 find a prevalence of 60.9%, BC being the most prevalent in their study; they considered it more a normal condition than an anatomical variant. Analysing subgroups of studies in North America and Europe revealed BC prevalence of 79.5%: it was the most frequent communication for North Americans. Rojas et al.7 reported a prevalence of 90% for this nerve communication. With respect to its frequency by sex, 83.3% were found in females and 16.7%, in males. In the Sirasanagandla study in Japan (2013),18 no differences were observed between age, race or sex. We found that 50% were identified in the right arm, while the other 50% were distributed evenly: 25% in the left arm and 25% bilaterally. Joyeeta et al.8 found that BC presented bilaterally in 60.5% of the cases and that its prevalence was almost the same in the right arm as in the left. As for its association with other communications, in our study 53.3% were found in isolation, 26.7% associated with another communication and 20%, associated with 2. Regarding clinical importance, some authors described a patient with traumatic laceration of the BC that led to a sensory loss in the areas between the middle and ring finger. The sensory loss decreased after surgical repair of the laceration.18
The least frequent communication in our study was MGC, with 7.2%. Joyeeta et al.8 found a prevalence of 19.5% for MGC, which was the third most prevalent in their study. However, in the individual studies with which the meta-analysis was carried out, the incidence reported ranged from 10% to 73.6%. In the analysis of subgroups based on geographic location, Joyeeta showed that MGC was most common among North Americans (with a prevalence of 29.1%), followed by Asians and Europeans (prevalence rates of 19.7% and 18.0%, respectively), and was less common among South Americans. Rojas et al.8 reported a prevalence of 56.5% for MGC. In their study, Cho et al.19 indicated that MGC prevalence differed according to the researcher and the research method, and they estimated a range of 6.6–54%. We find that, with respect to sex, MGC frequency is 66.6% in males, and that this is the sole communication in our study that is more frequent in the males. Joyeeta et al.8 did not mention a significantly important distinction between the two sexes. Our findings show that the frequency per limb is 4.04%: 60% are males and 40%, females. Of these, 44% are found bilaterally, 33.3% in the left arm and 22.2% in the right. Lee et al.20 observed that, in the 40.7% of their study cases for which they knew the sex, 52% were males and 48% were females, and that MGC presented bilaterally in 14.7%. Joyeeta et al.8 found that MGC is more common unilaterally, with dominance of the right side. However, in the reports that they revised from Kimura et al., Lee et al. and Kasakos et al.,12,20,21 they observed the opposite: that is, that MGC predominantly presents on the left and bilaterally, a result that is very similar to that of our study. In 90% of the cases, MGC is found in association with other communications.
ConclusionThe most frequent nerve communication in our environment is RCC, which principally presents in the left arm and in isolation.
Level of evidenceLevel of evidence V.
Conflict of interestsThe authors have no conflicts of interest to declare.
Please cite this article as: Lazo Velásquez JC, Barreto Montalvo J, Atoche Jasaui DR. Conexiones entre los nervios mediano-cubital por electromiografía en Lima (Perú), 2016. Rev Esp Cir Ortop Traumatol. 2018;62:415–420.
