



To analyse the clinical symptoms, aetiology and biomechanical aspects related to Sinding-Larsen-Johansson (SLJ) disease.
Materials and methodsA case control study was conducted, analysing the following variables: age, gender, clinical follow up, side of body with the symptoms, sporting activity, radiological stage, presence of patella alta, presence of short hamstring tendons, and increased posterior tibial slope.
ResultsA total of 15 knees in 14 patients were studied; one case with bilateral disease. The large majority of cases were 85.7% were male, and the mean age was 10.86 (standard deviation 1.61). All of them practised sport and physical activity at a high level with a variable duration of symptoms (1–36 months). There was predominance in side. The majority were radiological grade II (53.3). The data analysis did not show any significant difference (P>.05) between the study groups regarding the Caton and modified Insall indexes. There was a significant difference in the popliteal angle measured in the affected knees (mean: 32.50, SD: 8.9) compared with the control group (mean: 17.67, SD: 8.21). The difference in the posterior slope angle in the affected knees was also statistically significant (mean: 10.47, SD: 2.82) compared with the control (mean: 8.33, SD: 1.4).
ConclusionsAccording to our data, patients have short hamstring tendons and increased posterior tibial slope compared to the control group, and this difference is statistically significant.
Analizar los factores clínicos, etiológicos y biomecánicos asociados a la enfermedad de Sinding-Larsen-Johansson (SLJ).
Material y métodoEstudio de casos-control valorando los siguientes parámetros: edad, sexo, tiempo de evolución clínica, lateralidad, nivel de actividad deportiva, grado radiológico, existencia de patela alta, existencia de retracción de isquiotibiales y aumento de la caída posterior de la tibia.
ResultadosPresentamos 15 rodillas en 14 pacientes (un caso de afectación bilateral). El porcentaje de varones es del 85,7% y la edad media de afectación es de 10,86 años (d.t. 1,61). Todos ellos presentaban un nivel de actividad física y deportiva elevado con una duración de los síntomas muy variable (1-36 meses). Sin tendencia clara en cuanto a la lateralidad, la mayoría se incluyen en un grado radiológico tipo ii (53,3%). El análisis de los datos no muestra diferencias significativas (p>0,05) entre los grupos respecto al índice de Caton ni de Insall modificado. En la medición del ángulo poplíteo en las rodillas lesionadas, sí encontramos diferencias significativas (media: 32,50 d.t.:8,90) con respecto al grupo control (17,67; 8,21). La diferencia en la medición del ángulo de caída posterior en las rodillas lesionadas también ha resultado estadísticamente significativo (10,47; 2,82) con respecto a las rodillas de los casos control (8,33; 1,40).
ConclusionesLos pacientes con la enfermedad tienen un aumento de la pendiente tibial y retracción de isquiotibiales respecto al grupo control y esta diferencia es estadísticamente significativa.
Sinding-Larsen-Johansson (SLJ) disease is part of the osteochondrosis group of diseases. Osteochondrosis describes enchondral ossification disorders of an apophysis or epiphysis.1 In 1921–22 Sinding-Larsen and Johansson, independently but almost simultaneously, described the symptoms of the disease which eventually was named after both.2 Along with others such as Osgood-Schlatter disease, Blount disease, etc., these are lesions related to trauma or abnormal strain, with no pathological evidence of osteonecrosis.1 Initially, the first publications considered it as an epiphysitis with avascular necrosis,3 but subsequent studies showed the absence of bone necrosis.1
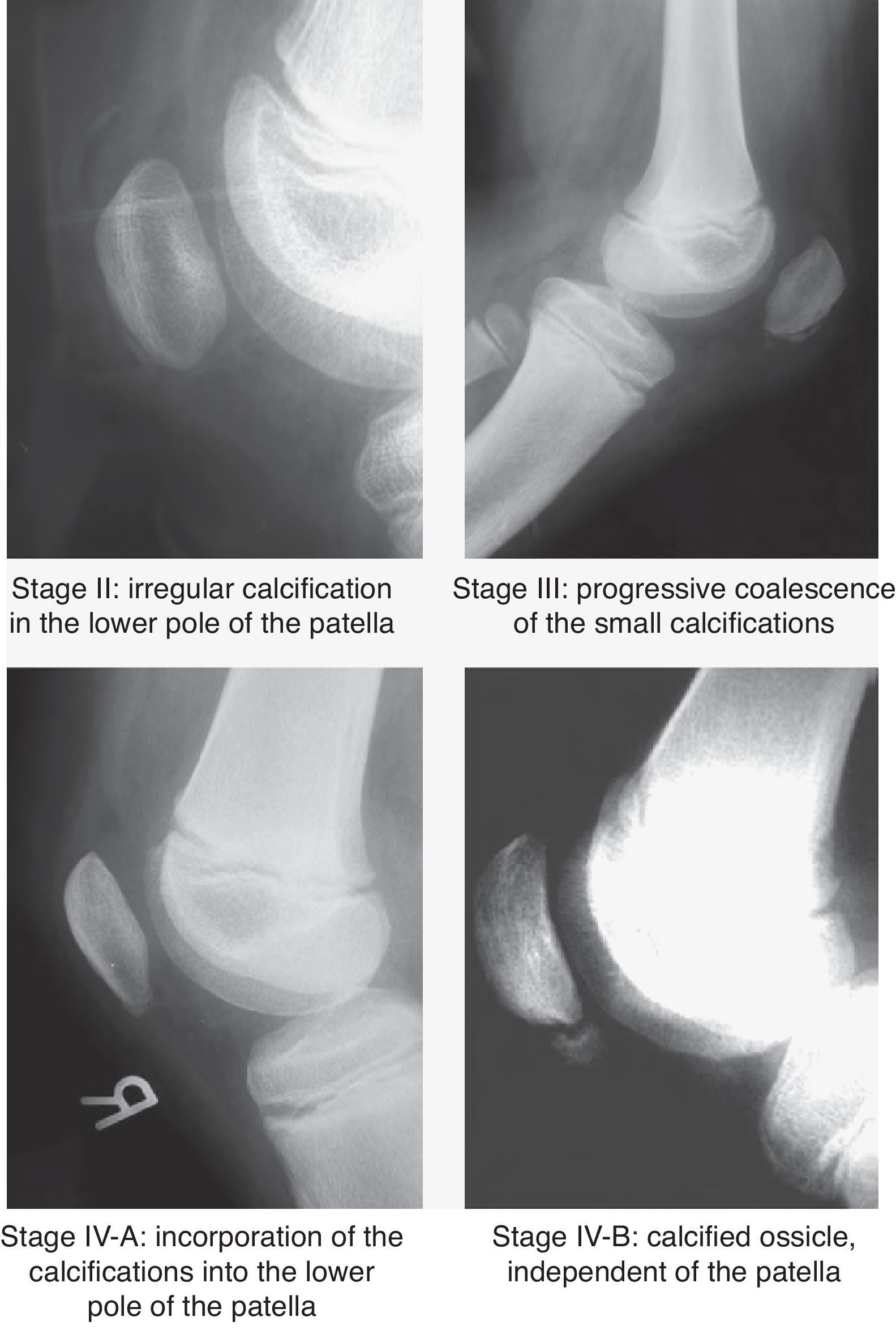
SLJ disease is a frequent cause of local pain and functional impairment of the knee in adolescent athletes in age of rapid growth, without previous trauma. There is a painful site in the lower pole of the patella and the proximal region of the patellar tendon, with local inflammatory signs that lead to functional impairment of the knee. The rest of the examination is normal.2 The radiographic images of bone fragmentation in the distal pole of the patella appear within weeks of these symptoms. There have been 4 radiographic stages described in SLJ disease (Fig. 1).3

The differential diagnosis is primarily established with sleeve fracture in the lower pole of the patella. Other entities to be to ruled out include stress fracture of the patella, type I bipartite patella and patellar tendinitis or “jumper's knee”.2
In some cases it is possible to observe the radiographic signs of Osgood-Schlatter disease and SLJ disease in the same knee.8 This pathology is also considered as traction apophysitis with symptoms located in the anterior tibial tuberosity. In both entities it is essential that the patient and family are informed of the self-limiting nature of the symptoms and their approximate duration of 12 months prior to spontaneous resolution. Conservative treatment should be implemented and surgery is not usually necessary.2
The aim of this study is to analyse the factors related to SLJ disease in terms of clinical characteristics (age, gender, laterality, duration of symptoms, radiographic stage), aetiology (practicing sports and which types) and biomechanics (variation in popliteal angle, posterior slope angle and relationship or not with the existence of high patella). Since other authors have established a relationship between the existence of high patella and the development of osteochondrosis,10 the working hypothesis of this study was to study a relationship between the existence of high patella, shortened hamstrings and increased posterior slope angle of the tibia, with the development of SLJ disease.
Materials and methodsWe performed a case–control study with 14 patients and 15 knees (1 case suffered bilateral involvement) versus 15 controls. The sample was collected prospectively for controls and through a historical cohort for cases included in the files of the Paediatric Orthopaedic Service of Hospital Teresa Herrera, a part of the Juan Canalejo complex in La Coruña, Spain. The study was approved by the Ethics Committee of the hospital. Data collection for cases was performed through a review of medical records and a personal interview to evaluate missing data.
The inclusion criteria for cases were: adolescents with non-traumatic pain in the distal patellar pole and with compatible radiographic findings. The criteria for controls were: adolescents who attended the Emergency Service for trauma or pain not related to SLJ disease and who had undergone knee radiographs (Tables 1–3).
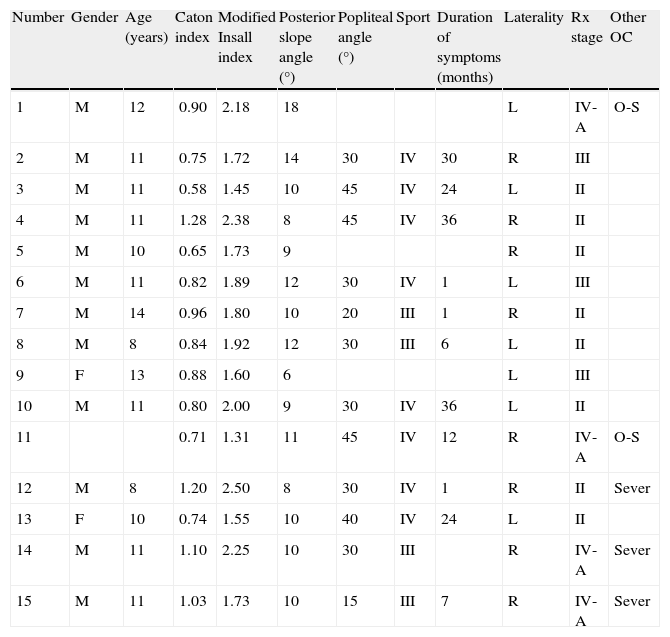
Cases of Sinding-Larsen Johansson disease.
| Number | Gender | Age (years) | Caton index | Modified Insall index | Posterior slope angle (°) | Popliteal angle (°) | Sport | Duration of symptoms (months) | Laterality | Rx stage | Other OC |
| 1 | M | 12 | 0.90 | 2.18 | 18 | L | IV-A | O-S | |||
| 2 | M | 11 | 0.75 | 1.72 | 14 | 30 | IV | 30 | R | III | |
| 3 | M | 11 | 0.58 | 1.45 | 10 | 45 | IV | 24 | L | II | |
| 4 | M | 11 | 1.28 | 2.38 | 8 | 45 | IV | 36 | R | II | |
| 5 | M | 10 | 0.65 | 1.73 | 9 | R | II | ||||
| 6 | M | 11 | 0.82 | 1.89 | 12 | 30 | IV | 1 | L | III | |
| 7 | M | 14 | 0.96 | 1.80 | 10 | 20 | III | 1 | R | II | |
| 8 | M | 8 | 0.84 | 1.92 | 12 | 30 | III | 6 | L | II | |
| 9 | F | 13 | 0.88 | 1.60 | 6 | L | III | ||||
| 10 | M | 11 | 0.80 | 2.00 | 9 | 30 | IV | 36 | L | II | |
| 11 | 0.71 | 1.31 | 11 | 45 | IV | 12 | R | IV-A | O-S | ||
| 12 | M | 8 | 1.20 | 2.50 | 8 | 30 | IV | 1 | R | II | Sever |
| 13 | F | 10 | 0.74 | 1.55 | 10 | 40 | IV | 24 | L | II | |
| 14 | M | 11 | 1.10 | 2.25 | 10 | 30 | III | R | IV-A | Sever | |
| 15 | M | 11 | 1.03 | 1.73 | 10 | 15 | III | 7 | R | IV-A | Sever |
F, female; L, left; M, male; OC, osteochondrosis; O-S, Osgood-Schlatter disease; R, right.
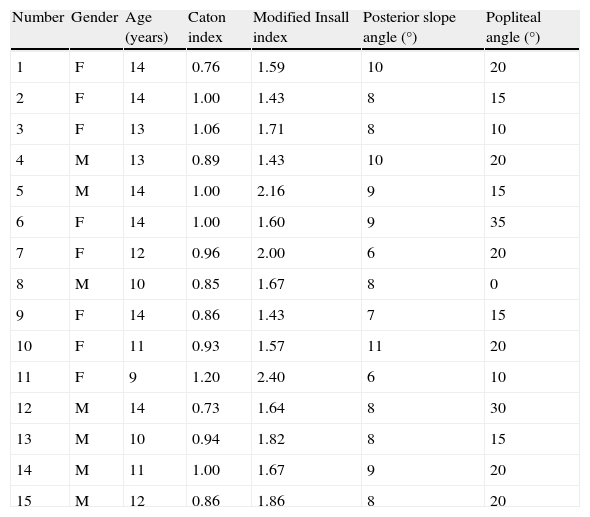
Normal knees.
| Number | Gender | Age (years) | Caton index | Modified Insall index | Posterior slope angle (°) | Popliteal angle (°) |
| 1 | F | 14 | 0.76 | 1.59 | 10 | 20 |
| 2 | F | 14 | 1.00 | 1.43 | 8 | 15 |
| 3 | F | 13 | 1.06 | 1.71 | 8 | 10 |
| 4 | M | 13 | 0.89 | 1.43 | 10 | 20 |
| 5 | M | 14 | 1.00 | 2.16 | 9 | 15 |
| 6 | F | 14 | 1.00 | 1.60 | 9 | 35 |
| 7 | F | 12 | 0.96 | 2.00 | 6 | 20 |
| 8 | M | 10 | 0.85 | 1.67 | 8 | 0 |
| 9 | F | 14 | 0.86 | 1.43 | 7 | 15 |
| 10 | F | 11 | 0.93 | 1.57 | 11 | 20 |
| 11 | F | 9 | 1.20 | 2.40 | 6 | 10 |
| 12 | M | 14 | 0.73 | 1.64 | 8 | 30 |
| 13 | M | 10 | 0.94 | 1.82 | 8 | 15 |
| 14 | M | 11 | 1.00 | 1.67 | 9 | 20 |
| 15 | M | 12 | 0.86 | 1.86 | 8 | 20 |
F, female; M, male.
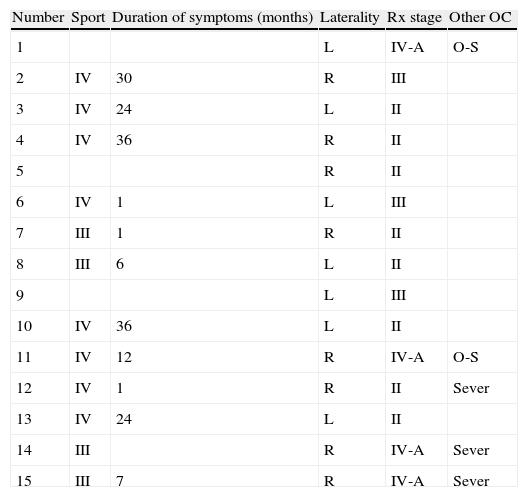
Normal knees.
| Number | Sport | Duration of symptoms (months) | Laterality | Rx stage | Other OC |
| 1 | L | IV-A | O-S | ||
| 2 | IV | 30 | R | III | |
| 3 | IV | 24 | L | II | |
| 4 | IV | 36 | R | II | |
| 5 | R | II | |||
| 6 | IV | 1 | L | III | |
| 7 | III | 1 | R | II | |
| 8 | III | 6 | L | II | |
| 9 | L | III | |||
| 10 | IV | 36 | L | II | |
| 11 | IV | 12 | R | IV-A | O-S |
| 12 | IV | 1 | R | II | Sever |
| 13 | IV | 24 | L | II | |
| 14 | III | R | IV-A | Sever | |
| 15 | III | 7 | R | IV-A | Sever |
L, left; OC, osteochondrosis; O-S, Osgood-Schlatter disease; R, right.
The exclusion criteria for cases were: patients with compatible symptoms but with stage I radiographs or radiographic silence, since these could act as a confounding factor if there was no radiographic progression. Neither did we include patients with some form of neurological disease that could alter muscle tone. We also excluded boys and girls in both groups whose radiographs were not in a purely lateral projection.
The study variables were gender, age, sports activity performed, duration of symptoms, laterality, radiographic classification, other associated osteochondrosis, measurement of the popliteal angle and radiographic measurements on the lateral knee projection (posterior slope angle of the tibia, as well as evaluation of high patella). All measurements were performed by the same observer.
Regarding sports activities, these were classified into the following 4 groups:
- ∘
GRADE I: inactivity.
- ∘
GRADE II: sport at school.
- ∘
GRADE III: non-competitive extracurricular activity.
- ∘
GRADE IV: competitive sport.
Patients were classified according to the 4 radiographic stages described in SLJ disease (Fig. 1):
- -
Stage I: normal patella.
- -
Stage II: irregular calcification in the lower pole of the patella.
- -
Stage III: progressive coalescence of the small calcifications.
- -
Stage IV: divided into:
- •
Stage IV-A: incorporation of the calcifications into the lower pole of the patella.
- •
Stage IV-B: calcified ossicle, independent of the patella.
- •
In order to assess the existence of other osteochondrosis we reviewed medical records in search of suspicious symptoms which could point to their presence (e.g. Sever disease). In the case of Osgood-Schlatter disease, the diagnosis was established by radiography.
In order to measure the popliteal angle, patients were placed in the supine position with the hip flexed to 90° and the contralateral limb resting on the table. We established this angle as the extension deficit of the knee under study.
We used the Caton–Deschamps11 and the modified Insall–Salvati12 indices for the radiographic assessment of the relationship between the patella and the patellar tendon length. This was because neither method requires taking into account the morphology of the patella, since they use the articular surface of the patella rather than its entire length. The Caton–Deschamps index establishes a high patella when the ratio between the distance from the articular surface of the patella to the plateau divided by the length of the articular surface of the patella is greater than 1.3.11 The modified Insall–Salvati index considers a high patella when the ration between the distance from the articular surface of the patella to the anterior tuberosity of the tibia and the length of the articular surface of the patella is greater than 2.12
Statistical analysis was performed using the software package SPSS® 15.0. We considered as statistically significant a value of P<.05. Descriptive statistics were expressed as absolute frequencies and percentages, means, ranges and standard deviations. We conducted statistical analysis to study the association between the different numerical variables (quantitative). In order to use the parametric Student t-test, due to its higher power than the non-parametric, Mann–Whitney alternative test, we began by verifying the degree of adjustment to the Normal model for each of the numerical variables with the Kolmorogov–Smirnov test. The results showed that the variables were in accordance with the Normal model (P<.05) in all cases, despite the small number of cases. Therefore, we decided to use the Student t-test. However, in order to confirm that the test results were not affected by the small number of subjects, we also used the alternative, non-parametric, Mann–Whitney test to corroborate the results of the Student t-test. These were verified in all cases.
ResultsThere was a predominance of males (85.7%) in the case group, whereas in the control group both genders were almost balanced. However, we did not observe a statistically significant difference (P>.05) between the 2 samples (Chi2 corrected for continuity; 1 df; =3.312 with P=.069). Nevertheless, we can say that there was a significant majority (P<.05) of males in the case group (Chi2; 1 df; =7.143 with P=.008).
The group of cases included children aged between 8 and 14 years, with a mean value of almost 11 years (10.86 and standard deviation of 1.61 years). The control group included patients aged between 9 and 14 years, with a slightly higher mean age (12.33 with a standard deviation of 1.76 years).
All cases were in groups III and IV of the radiographic grading method used (canoeing, judo, skating, etc.), with soccer being the most popular sport (almost 75%). Three patients could not be contacted due to a change of residence, so their sports practice was unknown.
The durations of the lesions were between 1 and 36 weeks, with a mean value of just over 16 weeks (95% confidence interval: 6.69–26.67) and high variability (standard deviation of 14.13 weeks), as well as a slight asymmetry towards the right side.
There were no significant differences regarding laterality.
The radiographic classification was divided into 5 stages. According to it, 53.3% of cases were type II, 26.7% were type IV-A and the remaining 20% were type III. There were no patients in stage I, since this was a reason for exclusion, and we did not find any patients in stage IV-B.
We found an association with other osteochondrosis in a high percentage of cases. Specifically, these were Sever disease in 20% of cases and Osgood-Schlatter disease in 13% of cases.
In the assessment of the relationship with the existence of high patella with respect to the Caton index, the mean value of the controls was 0.93 and that of the cases was 0.88. No statistically significant differences were observed (P[T]=.425 and P[M–W]=.331).
When analysing the modified Insall index, the mean value of the controls was 1.73 and that of cases was 1.86. No statistically significant differences were observed (P[T]=.245 and P[M–W]=.187).
Regarding the measurement of the popliteal angle, the mean value of the controls was 17.67° and that of cases was 32.50°. The differences were statistically significant (P<.05) in both the t-test (t=4.282; 23 df; P=.000) and the Mann–Whitney U-test (U=19.00; P=.001).
Regarding the measurement of the posterior slope angle of the tibia, the mean value of the controls was 8.33° and that of cases was 10.47°. This difference was statistically significant (P[T]=.014 and P[M–W]=.01).
DiscussionWe conducted a case–control study to assess the factors involved in the epidemiology of Sinding-Larsen-Johansson disease. Although it seems clear that the origin of this pathology is traction on the insertion of the patellar tendon1 in the inferior pole of the patella, there are many medical conditions that are confused with different pathogenesis.
The epidemiological data of our sample corresponded to the data of the samples of the leading studies on this subject. Thus, in a prospective study, Medlar and Lyne3 analysed 8 patients of whom 7 were male, all aged between 10 and 13 years. The series by Iwamoto et al.4 consisted of 7 males aged between 11 and 13 years. Tyler and McCarthy5 published 2 cases of osteochondrosis in girls aged 7 and 11 years, although in this case the pathology was studied in the proximal pole of the patella. The existence of a majority of males, although not statistically significant compared with controls, could lead to a suspicion of bias, or else it could mean that this lesion is more prevalent among males.
When we evaluated sport activities as described in the aforementioned series, we observed that soccer was the most popular sport in all cases,4 followed by various martial arts in the series originating in the East. It seems clear that sports with higher demands on the extensor apparatus are to be blamed for the development of this disease, especially if started at the age in which the patella begins its ossification, which is around the age of 5 or 6 years,6 and if they are practiced with a competitive intensity.
In relation to overload of the quadriceps muscle and the development of SLJ disease, Rosenthal and Levine7 described the appearance of this condition in 7 children in a series of 85 patients suffering paediatric cerebral palsy. They concluded that it was the result of excessive traction of the quadriceps within a flexion contracture. In this sense, Perry et al.8 found that quadriceps strength increased by 6% for each degree of flexion, in order to stabilise the patella.
In accordance with the series in the works reviewed, the duration of symptoms was very variable. In our work, the duration varied from 1 to 36 weeks, but in the literature we found variations between 6 and 14 weeks according to Iwamoto, and variations between 3 weeks and 1 year in the series of Medlar. Although some authors have related these prolonged symptoms with the natural evolution of the disease from its initial stages until complete ossification of the calcification (stage IVB), a continuation of physical activity could also be considered as a reason for this variability. The stage of the disease at the time of consultation was widely variable, but the pathology requires an interruption of physical activity in order for symptoms to remit. In our study we failed to establish a relationship between radiographic grade and time of evolution. Neither did Medlar and Iwamoto find such a relationship in their series.
As in other series in the literature, there is no clear trend in laterality, although we must remember that all the series are small, so this could limit the observation of statistically significant differences.
Regarding the radiographic stage, the sample was dispersed and without clear convergence in the early stages, which would be expected at the time of the first consultation. It seems clear that the symptoms do not always appear in the first radiographic stage, so there is no relationship between the radiographic stage and the appearance of symptoms. This fact is supported by the reports of Medlar of patients with radiographic abnormalities and without clinical manifestations. This fact makes it more difficult to assess the true incidence of the disease, since only those patients with clinical manifestations attend consultation. We could not find a statistically significant association between radiographic stage and duration of symptoms, so we could not establish that finding an image in a patient in an advanced stage would result in the remission of symptoms within a short period of time. It is possible that further studies with larger numbers of cases would prove the existence of a correlation between radiographic stage and appearance or disappearance of symptoms.
The association with other osteochondrosis has also been reported in the literature.9 Above all, there have been mentions of the association with Osgood-Schlatter disease, which in this study appeared in 13% of cases. Conversely, we found no references to the concomitant appearance of Sever disease, located in the calcaneus around the age of 9–11 years, which in our series appeared in 20% of cases. The reasons why several osteochondrosis may appear simultaneously are not known.
One of the main objectives of this study was to assess the relationship of SLJ disease with the existence of a high patella, as reported by Aparicio et al.10 for Osgood-Schlatter syndrome. In his series, Medlar also observed this fact, but only assessed it in 5 patients in stage IV-A, in whom there was neither high nor low patella. There are reports in the literature10 on how a high patella can increase tension in the patellar tendon insertion. The lever arm decreases in the last degrees of extension, thus requiring more force to achieve a full extension. The Caton index is a simple and reproducible method which is not affected by skeletal maturity, making it an ideal method for measuring the height of the patella during adolescence.10 In addition, we also used the modified Insall index for this measurement, as it offers the same advantages. In the present series we could not establish an association between SLJ disease and the existence of high patella. Regarding the existence of high patella in patients with Osgood-Schlatter disease and SLJ disease, of the 2 patients with Osgood-Schlatter disease, only 1 presented a modified Insall index greater than 2.
Almost our entire series of patients showed a shortening of the hamstring muscles. In order to asses this, we measured the deficit in knee extension with the hip flexed to 90°, as well as the posterior slope angle of the tibia, which could favour a tendency towards knee flexion and, therefore, a greater burden on the quadriceps.8 There is a small series with N=12 cases which measured the popliteal angle. Despite being small, it was the longest series in the literature consulted and was sufficient to find statistically significant differences. The assessment of posterior slope was performed in 15 cases. Since we found no evidence of any studies regarding this issue, it thus becomes the most important contribution of this work. Therefore, we could suggest that practicing sports which involve running and kicking at an early age may promote an increase in the posterior slope angle of the tibia and, similarly, a shortening of the hamstring muscles. This in turn would trigger an overload in the quadriceps and the possibility of developing SLJ disease. This working hypothesis requires further studies focused on that line of investigation.
In the present series we have attempted to relate other assessed factors (radiographic stage and duration of symptoms, laterality and type of sport practiced) but could not draw any such conclusions. Perhaps a larger sample would enable us to do so. Moreover, we did not carry out a follow-up of the radiographic progression after discharge.
The present work offers more data on the pathogenesis of this disease, confirming our hypothesis that a shortening of the hamstring muscles and an increase in the posterior slope angle of the tibia are associated with the development of SLJ disease.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation did not require experiments on humans or animals.
Confidentiality of dataThe authors declare that they have followed the protocols of their workplace on the publication of patient data and that all patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare having obtained written informed consent from patients and/or subjects referred to in the work. This document is held by the corresponding author.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: López-Alameda S, et al. Enfermedad de Sinding-Larsen-Johansson: análisis de factores asociados. Rev Esp Cir Ortop Traumatol. 2012;56:354–60.
