



Although much has been published on the effect of the pandemic on trauma emergencies, it has not been analysed whether the incidence of infection or different organisation of available resources according to the Spanish region were influential factors. We present a multicenter study of three tertiary hospitals in three Spanish cities with different characteristics to study how these factors influenced paediatric trauma emergencies during the first wave of the pandemic.
Material and methodsWe present a retrospective cohort study that compares and analyzes paediatric trauma emergencies in three different hospitals during the period of the first wave of the COVID-19 pandemic and we compare them with the same period of the previous year, analyzing the number of emergencies, the severity of the pathology, the average age of the patients, the days of admission and the waiting time of the cases that required surgical treatment.
ResultsA total of 6474 paediatric trauma emergency episodes have been analysed. There was a drastic reduction in activity in the three hospitals, but in different amounts: 83.5% in the hospital located in Madrid, 75% in the hospital located in Valencia and 65.9% in the one located in Palma, Majorca. The emergencies attended were more serious in 2020 compared to 2019. The average age of patients treated during the pandemic was lower compared to the previous year. There were no differences in the days of admission, but there were differences in the delay in surgery for surgical fractures.
ConclusionsThe impact of the first wave of the COVID-19 pandemic and the decreed confinement had a different impact on paediatric trauma emergencies in the different hospitals according to the incidence of infection and the measures adopted in the different regions. In all cases there was a significant reduction in activity, a greater proportion of medium and severe pathologies were attended to, the average age of the patients attended was lower and a delay was observed in surgeries performed in the emergency room, probably due to the need to request a PCR test to detect a COVID-19 infection.
Aunque se ha publicado mucho sobre el efecto de la pandemia en las urgencias traumatológicas, no se ha analizado si la incidencia de la infección o la distinta organización de los recursos disponibles según la comunidad autónoma fueron factores influyentes. Presentamos un estudio multicéntrico de 3 hospitales terciarios de 3 ciudades españolas con distintas características para estudiar cómo estos factores influyeron a las urgencias traumatológicas pediátricas durante la primera ola de la pandemia.
Material y métodosPresentamos un estudio retrospectivo de cohortes que compara y analiza las urgencias traumatológicas pediátricas en 3 hospitales distintos durante el periodo de la primera ola de la pandemia COVID-19 y comparamos sus resultados con los del mismo periodo del año anterior, analizando el número de urgencias, la gravedad de la dolencia, la edad media de los pacientes, los días de ingreso y el tiempo de espera de los casos que requirieron tratamiento quirúrgico.
ResultadosSe han analizado 6.474 episodios de urgencias traumatológicas infantiles. Se produjo una drástica reducción de la actividad en los 3 hospitales, pero en distinta cuantía: del 83,5% en el hospital localizado en Madrid, del 75% en el hospital localizado en Valencia y del 65,9% en el ubicado en Palma de Mallorca. Las urgencias atendidas fueron de mayor gravedad en el año 2020 en comparación con el año 2019. La edad media de los pacientes atendidos durante la pandemia fue menor en comparación con el año anterior. No hubo diferencias en los días de ingreso, pero sí en la demora de la cirugía de las fracturas quirúrgicas.
ConclusionesLa repercusión de la primera ola de la pandemia de COVID-19 y el confinamiento decretado tuvieron una repercusión distinta en las urgencias traumatológicas pediátricas en los distintos hospitales según la incidencia de la infección y las medidas adoptadas en las diferentes comunidades autónomas. En todos los casos hubo una reducción importante de la actividad, se atendió una mayor proporción de dolencias medias y graves, la edad media de los pacientes atendidos fue menor y se observó un retraso en las cirugías realizadas en urgencias, probablemente por la necesidad de solicitar una prueba PCR para detectar una infección por COVID-19.
The COVID pandemic has changed many aspects of our lives, including healthcare at many levels. The first wave, in the spring of 2020, had the greatest impact on all levels of medical care, as it was accompanied by a lockdown of the population, decreed on 14 March 2020.1 This has never been experienced before and is worth studying and analysing for the future.
Many studies have been published on how this situation affected medical emergencies in hospitals, and trauma emergencies in particular, but none have analysed whether the consequences were different according to the geographical region due to different incidences of infection and the different organisation of available resources according to the autonomous community.
We present a multicentre study of three tertiary hospitals of three Spanish cities with different incidences of COVID-19, different ways of reorganising available resources and a different rate of de-escalation during the first wave of the pandemic, and study how the activity of paediatric trauma emergency departments was affected compared to the same period of the previous year.
Material and methodsThis is a retrospective cohort study comparing and analysing paediatric trauma emergencies attended in three hospitals in different Spanish cities during the first wave versus the same period in the previous year.
We selected three tertiary hospitals in three different cities, one with a high incidence, where it was decided to allocate all paediatric trauma emergencies to another paediatric hospital (Hospital 12 de Octubre in Madrid), another with a medium incidence and without any measures regarding paediatric trauma emergencies (Hospital Universitario y Politécnico la Fe in Valencia), and a third in a region with a low incidence and which was the referral centre for all these emergencies (Hospital Son Espases in Palma de Mallorca).
Incidence data were calculated according to the cases reported to the National Epidemiological Surveillance Network (RENAVE) of the Instituto de Salud Carlos III. As of 29 May 2020, 64,408 cases of Coronavirus infection had been reported in the Community of Madrid, 13,777 in the Community of Valencia, and 2084 in the Community of the Balearic Islands.2
We collected the number of paediatric trauma emergencies per day during the first wave (15 March to 21 June 2020) and during the same period of the previous year (15 March to 21 June 2019) in the three hospitals. We collected age and diagnosis, grouping them into mild conditions not requiring specialist follow-up (sprains, contusions, minor injuries), moderate conditions not requiring admission but requiring specialist follow-up (non-displaced or slightly displaced fractures, more serious injuries), and severe conditions requiring admission and surgical treatment. We also recorded whether, if surgery was required, a PCR test had to be performed, and if so, the result of this test, and whether this delayed the surgery.
For statistical processing, the data from each hospital were divided into two groups according to date: pre-pandemic and during the pandemic. Qualitative variables were compared using Pearson's χ2 test. For quantitative variables, normal distribution and homogeneity of variances were tested with the Shapiro–Wilk test and Levene's test, respectively. When these applicability hypotheses were met, the analysis of variance method (ANOVA) was used, otherwise the non-parametric Kruskal–Wallis test was used.
In all cases a 95% confidence interval was assumed and p-values of less than .05 were considered statistically significant differences. R Commander graphical user interface to the R software was used for the statistical analysis.
ResultsA total of 6474 episodes of paediatric trauma emergencies were included. Of these, 5240 were in 2019 and 1234 in 2020.
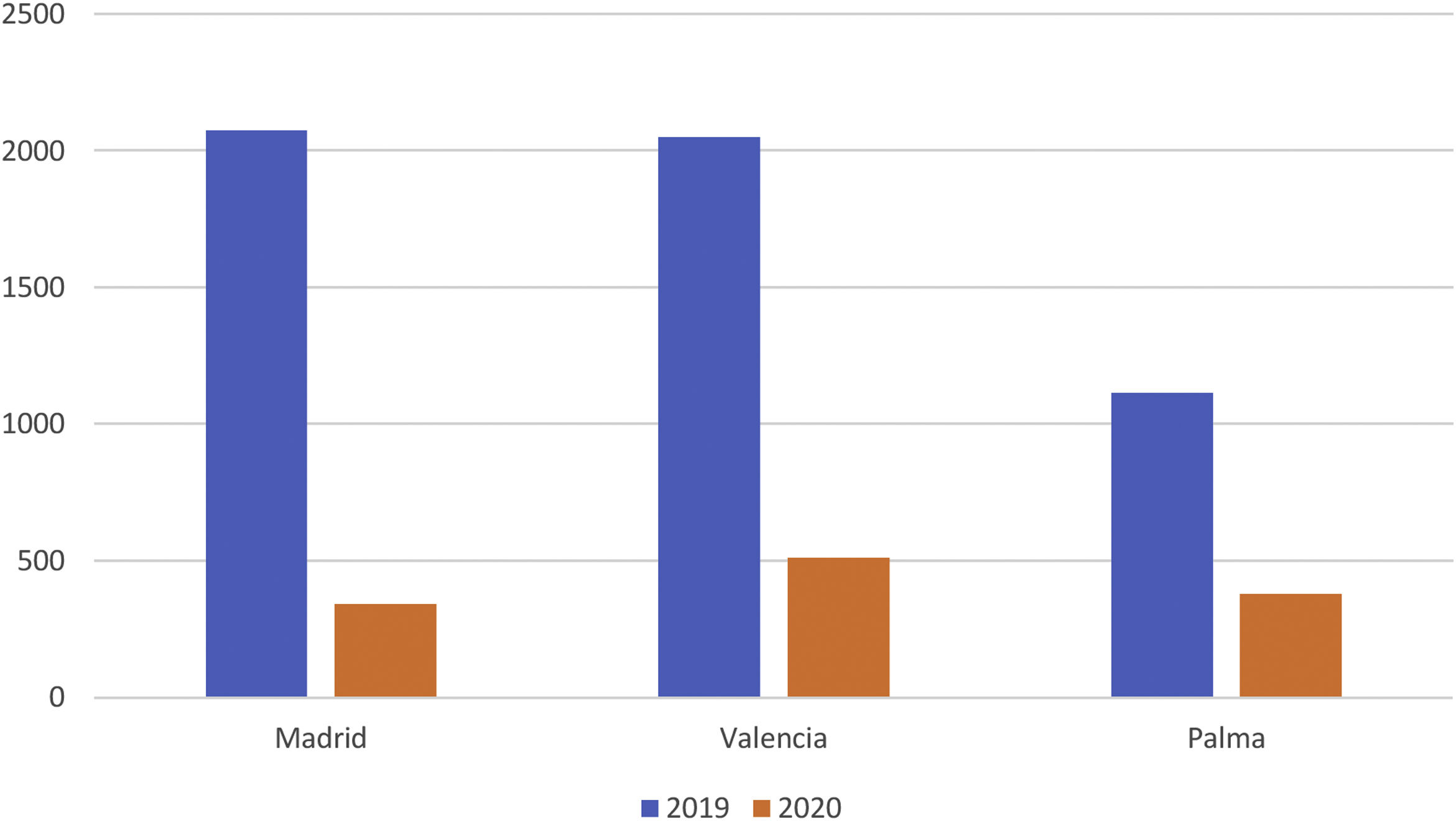
The three hospitals experienced a drastic reduction in their activity during the first wave of the COVID-19 pandemic in our country, when a total lockdown was enforced with respect to the same period of the previous year, although the reduction differed due to the different health measures taken in each autonomous community. In the Madrid hospital paediatric emergency care decreased by 83.5%, in the Valencia hospital by 75% and, finally, in the Palma de Mallorca hospital the reduction was 65.9% (Fig. 1).

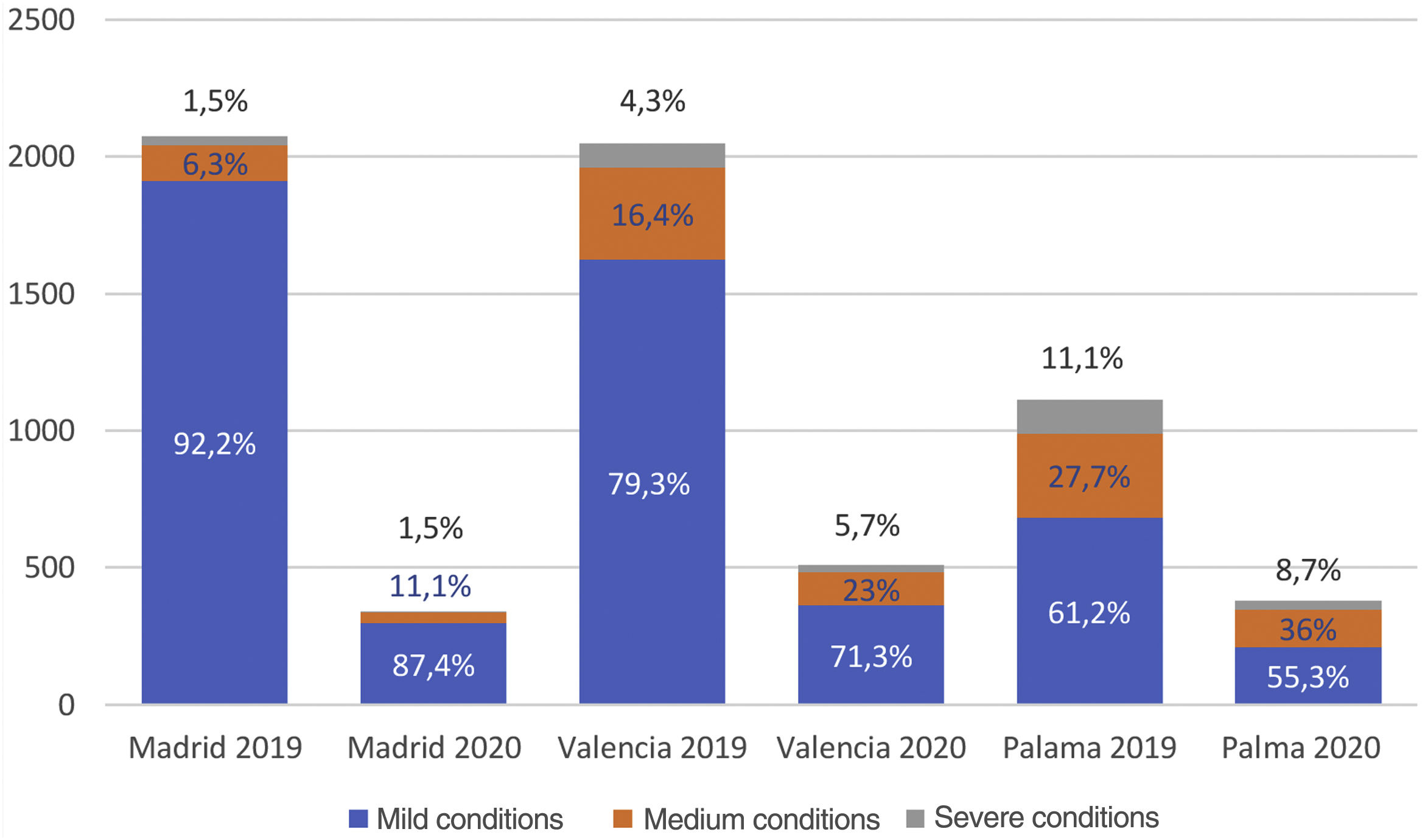
In terms of the type of conditions treated during this period, the proportion of moderate and severe conditions was higher in all three hospitals. In the Madrid hospital, during 2019, before the pandemic, the percentage of mild conditions attended in the emergency department was 92.2%, the percentage of moderate conditions was 6.3%, and the percentage of severe conditions was 1.5%, compared to 87.4%, 11.1%, and 1.5% in 2020, respectively. In the Valencia hospital, the percentage of emergencies attended in 2019 was 79.3% for mild conditions, 16.4% for moderate conditions, and 4.3% for severe conditions, compared to 71.3%, 23%, and 5.7% in 2020, during the first wave of the pandemic, respectively. Finally, in the Palma de Mallorca hospital, the percentage of mild conditions attended in 2019 was 61.2%, moderate conditions 27.7%, and severe conditions 11.1%, compared to 55.3%, 36%, and 8.7% in 2020, respectively. In other words, during the pandemic, a statistically significant higher percentage of moderate and severe conditions were treated in the three hospitals (Madrid, p=.005525; Valencia, p=.000511, and Palma de Mallorca, p=.005907) and overall (p=4.0e−16) (Fig. 2).
, emergencies with medium conditions (non-displaced fractures, wounds sutured with local anaesthesia, etc.) requiring follow-up in outpatient clinics, and emergencies with severe conditions requiring admission or surgical treatment.")
Rate of trauma emergencies attended in the three hospitals during the two periods studied divided into emergencies with mild conditions (sprains, contusions, epiphysiolysis type I, superficial wounds, etc.), emergencies with medium conditions (non-displaced fractures, wounds sutured with local anaesthesia, etc.) requiring follow-up in outpatient clinics, and emergencies with severe conditions requiring admission or surgical treatment.
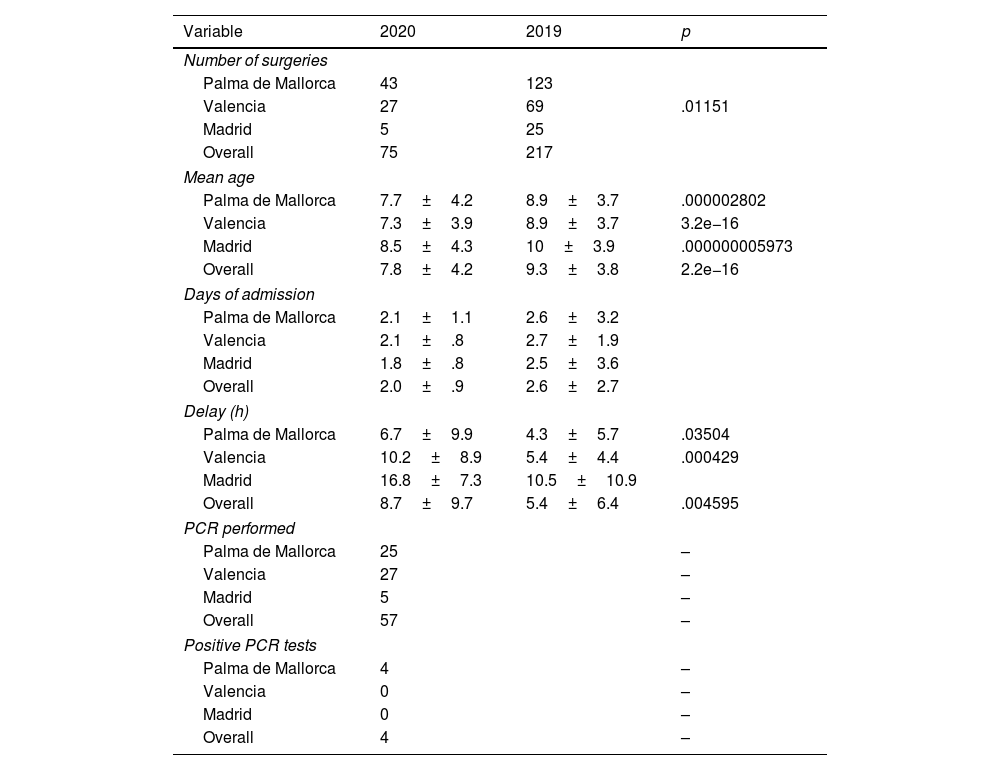
In 2020, PCR testing for SARS-CoV-2 was requested for 100% of the surgeries performed in the Madrid and Valencia hospitals, but only for 58% in the Palma de Mallorca hospital, because it was not a requirement for procedures performed under sedation in that centre. In the hospitals of Madrid and Valencia no positive COVID cases were detected from the tests performed, whereas in Palma de Mallorca 4 positive cases were detected (Table 1).
Data from the three hospitals and overall data on the number of surgeries performed in the two periods studied: mean age of the patients, days of admission, delay from admission to emergency department to surgery measured in hours, PCR tests performed, and positive cases.
| Variable | 2020 | 2019 | p |
|---|---|---|---|
| Number of surgeries | |||
| Palma de Mallorca | 43 | 123 | |
| Valencia | 27 | 69 | .01151 |
| Madrid | 5 | 25 | |
| Overall | 75 | 217 | |
| Mean age | |||
| Palma de Mallorca | 7.7±4.2 | 8.9±3.7 | .000002802 |
| Valencia | 7.3±3.9 | 8.9±3.7 | 3.2e−16 |
| Madrid | 8.5±4.3 | 10±3.9 | .000000005973 |
| Overall | 7.8±4.2 | 9.3±3.8 | 2.2e−16 |
| Days of admission | |||
| Palma de Mallorca | 2.1±1.1 | 2.6±3.2 | |
| Valencia | 2.1±.8 | 2.7±1.9 | |
| Madrid | 1.8±.8 | 2.5±3.6 | |
| Overall | 2.0±.9 | 2.6±2.7 | |
| Delay (h) | |||
| Palma de Mallorca | 6.7±9.9 | 4.3±5.7 | .03504 |
| Valencia | 10.2±8.9 | 5.4±4.4 | .000429 |
| Madrid | 16.8±7.3 | 10.5±10.9 | |
| Overall | 8.7±9.7 | 5.4±6.4 | .004595 |
| PCR performed | |||
| Palma de Mallorca | 25 | – | |
| Valencia | 27 | – | |
| Madrid | 5 | – | |
| Overall | 57 | – | |
| Positive PCR tests | |||
| Palma de Mallorca | 4 | – | |
| Valencia | 0 | – | |
| Madrid | 0 | – | |
| Overall | 4 | – | |
p-values are expressed when differences are statistically significant; blank spaces correspond to statistically non-significant values.
The mean age of the patients treated was lower during the period of pandemic compared to the previous year in the three hospitals studied, with a statistically significant difference. In the Madrid hospital the mean age of patients seen in 2020 was 8.5 years, compared to 10 years in 2019; in the Valencia hospital it was 7.3 in 2020 compared to 8.9 in 2019, and in the Palma de Mallorca hospital it was 7.7 compared to 8.9 in 2019 (Table 1).
We found no statistically significant differences in the mean number of days of admission, although it was slightly lower during the pandemic period. In the Madrid hospital it was 2.5 days in 2019 versus 1.8 days in 2020; in the Valencia hospital it was 2.7 days in 2019 versus 2.1 in 2020, and in the Palma de Mallorca hospital it was 2.6 days in 2019 versus 2.1 in 2020 (Table 1).
We did find statistically significant differences in the waiting hours for interventions performed in the emergency department, noting an increase in hours of delayed surgery during the pandemic period in two of the three hospitals, which could be attributed to waiting for PCR test results. The mean waiting time in the Valencia hospital was 5.4h in 2019 versus 10.2h in 2020, and in the Palma de Mallorca hospital it was 4.3h in 2019 versus 6.7h in 2020 (Table 1).
DiscussionThe COVID-19 pandemic has affected our work in an unprecedented and universal way. We need to analyse these changes to understand the significance of what has happened.
The influence of the first wave and of lockdown on trauma emergencies in the adult population has been well studied. A study carried out in a health area of the Valencian Community showed a reduction of 58.8% in trauma emergencies attended compared to the previous two years and a reduction of 37.6% in fractures requiring emergency admission or surgery, with a change in the distribution of the type of fractures attended, since although appendicular fractures of the upper and lower limbs decreased, the rate of osteoporotic fractures of the hip and vertebrae remained stable. The authors attribute this to the fact that appendicular fractures are associated with physical activity that predisposes to falls or trauma, while osteoporotic hip and vertebral fractures occur spontaneously or after a simple fall at home.3 Interestingly, in this study the delay in emergency surgery was less than in previous years, which the authors relate to less pressure on operating theatres.
Other national studies have also observed a constant rate of osteoporotic hip fractures during the lockdown, despite a decrease in the total number of fractures.4,5 A review of articles published worldwide on the number of fractures in adults shows a decrease in the number of fractures in the adult population of an average of 53%, with a range from 20.3% to 84.6%.6
In our study, paediatric trauma emergency activity was affected in the three hospitals studied, but to a different extent depending on the health measures adopted by the different communities. In Madrid, where it was decided that paediatric trauma emergencies should be referred to a specialist paediatric hospital, the reduction was 83%; in Valencia, where no measure was taken in this regard, the reduction was 75%, while in Palma de Mallorca, where it was decided that this hospital would be the referral centre for paediatric trauma emergencies, as was routine, the reduction was 65.9%. The type of organisation was not related to incidence but to a decision by each autonomous community, and only refers to the distribution of patients in the emergency department.
This difference in the reduction of trauma emergencies could also be because the first wave of the pandemic also affected the three cities in the study differently; the highest incidence was in Madrid, medium in Valencia, and low in Palma de Mallorca.2
This reduction was greater than in other studies of trauma emergencies in adults, perhaps because the mechanism of fracture production in children is directly related to leisure and sporting activities outside the home.7,8
A study conducted in Finland on paediatric surgical emergencies from 1 March to 31 May 2020 compared to the same period 3 years earlier showed no significant reduction in the number of appendectomies and interventions required for intestinal torsion, but there was a significant reduction in surgical interventions to treat fractures, mainly of the lower limb, closely related to practising sports. Unlike Spain, there was no complete lockdown in Finland, but schools were closed, and all collective sporting activities were suspended.9
Bram et al.10 studied the paediatric fractures treated in a level 1 hospital in the United States during the first wave of the pandemic, comparing them with the same period in the previous two years. There was no total lockdown in the United States either, but schools were closed, and sporting activities were limited. These authors note a reduction in the number of paediatric fractures of 60% compared to the previous 2 years, mainly due to a decrease in fractures related to sporting activities. This means that the average age of the patients was lower during the period of the pandemic.10
Similar studies have been published on the incidence of paediatric fractures in the United Kingdom,11,12 Ireland,13 Turkey,14 Iran,15 the United States,16,17 and New Zealand,18 all showing a clear decrease in the number of paediatric fractures treated, with a decrease in the average age of the patients, with a greater proportion of fractures in older children and adolescents related to sports and outdoor activities.
In our review, the mean age of patients was also lower in 2020, during the pandemic, compared to 2019, with a statistically significant difference in the three hospitals studied.
We only found one published work in which more paediatric fractures were observed during the lockdown, but the study focuses on a single hospital, with a really low number (8 surgical fractures in 2020 compared to 3 in the same period in 2018). This may have influenced the results, although the authors attribute this to the children remaining at home increasing the chances of fractures due to lack of supervision.19
All the studies that we have cited include the number of paediatric fractures, but not the number of paediatric trauma emergencies. In our study we also collected other types of traumatic conditions, such as contusions, sprains, etc. We therefore divided the type of conditions into three groups according to severity and observed that during the period of the pandemic, patients with moderate or severe conditions attended in greater proportion than the group with mild conditions, compared to the previous year. This could be due to the population's fear of going to hospital because of the risk of contracting the virus.20,21
In a study conducted in a paediatric hospital in Barcelona, an area which also had a high incidence of COVID infection, and which acted as the referral hospital for paediatric trauma emergencies, a decrease of 78.6% was observed in the total number of fractures, with greater severity in patients attending the emergency department during this period. However, the differences with the same period in 2018 and 2019 were not statistically significant.22
In our study, there were 75 surgical fractures during the pandemic. A mean delay from admission to the emergency department to surgery of 8.7h was observed, compared to 5.4h in 2019, and this difference was statistically significant. It is possible that this delay is due to the need for the patient to take a PCR test to undergo surgery.
The mean length of stay of patients admitted during the pandemic was slightly shorter (2.0 days) compared to the previous year (2.6 days), but this difference was not statistically significant.
The incidence of COVID-19 infection in the paediatric population has been estimated to be much lower than in the adult population: around 2%.23,24 In all patients who took PCR tests because they required admission or surgery, only 4 positive cases were detected, surprisingly in Palma de Mallorca, where the incidence of infection was the lowest in the country at the time. Other authors did not detect positive cases in the paediatric population treated for a fracture,19 unlike in the adult population, where up to 5.68% of positive COVID-19 results were found in patients treated for a fracture.6
The limitations of this study lie in its retrospective nature, but it is the first at national level to compare three tertiary hospitals in cities where the incidence of the pandemic differed during the first wave, the available health resources were also organised differently according to their autonomous community. Furthermore, although several articles have been published on this subject worldwide, most focus on fractures treated and not on all the trauma emergencies attended; this information is very useful for planning available resources.
ConclusionsThe first wave of the COVID-19 pandemic in Spain and the lockdown enforced to contain infections led to a drastic reduction in paediatric trauma emergencies attended in the three hospitals studied, although this reduction varied according to the measures adopted to organise healthcare resources and the incidence of the pandemic. In all three hospitals, a higher proportion of moderate and severe conditions were treated compared to the previous year. The average age of the patients treated was lower compared to the same period in the previous year. A delay was observed in surgeries performed in the emergency department compared to the previous year, probably because a PCR test for COVID-19 infection was required.
Level of evidenceLevel of evidence III.
FundingNo specific support from public sector agencies, commercial sector or non-profit organisations was received for this research study.
Conflict of interestsThe authors have no conflict of interests to declare.
