





The case deals with a 78 year-old patient who suffered a right ileo- and ischiopubic rami fracture after a casual fall. A few hours later, she presented with sudden abdominal pain and hypotension. Imaging test showed extraperitoneal hemorrhage with active bleeding and hemodynamic compromise. The progressive worsening, with anemia and hemodynamic instability, required her to be sent to the reference hospital for selective embolization of the bleeding point.
After embolization, the patient's situation stabilized, and she was then able to sit down one week later. The fracture consolidated 3 months later.
Although low-energy pelvic fractures by lateral compression do not usually present with complications, sometimes they require a strict control due to the potential risk of vascular injuries.
Paciente de 78 años que sufre fractura de ramas ilio e isquipubiana derechas tras caída casual. A las pocas horas presenta un cuadro de dolor abdominal brusco e hipotensión, siendo diagnosticada de hemorragia extraperitoneal con sangrado activo y repercusión hemodinámica. Ante el progresivo empeoramiento, con anemización e inestabilidad hemodinámica, es remitido al hospital de referencia, donde se realiza embolización selectiva del vaso sangrante.
Tras la embolización, la paciente se estabiliza y permanece ingresada, comenzando sedestación una semana más tarde y con consolidación de las fracturas a los 3 meses.
Las fracturas pélvicas de baja energía por compresión lateral suelen presentar escasas complicaciones, aunque precisan un control exhaustivo por el riesgo potencial de lesiones vasculares. Es estos casos suponen un riesgo vital, siendo la embolización selectiva del punto sangrante un método de control eficaz, que tampoco está exento de complicaciones graves.
Pelvic ring fractures can take place following both low-energy and high-energy trauma, and this will condition their gravity and, therefore, the prognosis and treatment are called for. The prognosis and classification are established using conventional radiography. Other complementary tests, like computed tomography (CT), may provide additional information.
Case reportThe patient was a 78-year-old female who attended the emergency room due to pain in the hip after an accidental fall in her home garden. Her personal history included a probable allergy to penicillin and derivatives, arterial hypertension and severe pulmonary hypertension secondary to scleroderma. She was following a chronic treatment with pravastatin, pantoprazole, sildenafil, nifedipine and strontium ranelate.
The patient reported pain in the right inguinal region since the fall and presented a slight functional impairment. No deformities could be observed and the distal neurovascular exploration was normal.
We conducted imaging studies (lumbar and pelvic radiographs), and diagnosed a non-displaced fracture of the right ilio- and ischiopubic branches, Tile type A2. The patient was admitted for observation and analgesic control (Fig. 1).

After 5h of admission, the patient suddenly suffered dizziness, sweating and abdominal pain symptoms, without thoracic pain (tension 70/40mmHg), so an urgent assessment was requested from the Internal Medicine department, which obtained thoracic and abdominal radiographs, as well as an urgent biochemical analysis and electrocardiogram (ECG). On exploration, the patient appeared oriented and collaborative, eupneic and pallid. Cardiopulmonary auscultation was normal. Abdominal palpation identified an unusual pain in the inferior hemiabdomen, which appeared swollen and hard, with positive rebound. The analysis reported microcytic anemia (hemoglobin 9.4g/dL; mean corpuscular volume 78fL) and glycemia of 220mg/dL, with the remaining analyzed parameters being normal. In the ECG, sinusal rhythm was at 90beats/min. The abdominal radiograph observed a mass effect at the level of the pelvis-hypogastrium, with displacement and abundant air pattern.
Upon suspicion of extraperitoneal hemorrhage by visceral lesion, an abdominal CT study with contrast was requested for differential diagnosis. Absolute diet and serum therapy were initiated, along with transfusion of 2 packed red blood cell concentrates, when a drop of 1.5g/dL was observed in the serum hemoglobin levels.
The patient continued to present episodes of hypotension which responded to perfusion of crystalloids.
The abdominal CT scan obtained showed pericardial hemorrhage and cardiomegaly, with no apparent cause, bibasal atelectasis by hypoventilation, free perihepatic fluid in both paracolic gutters and at the bilateral retroperitoneal level. Retention stomach. Large pelvic hematoma, very heterogeneous, with extravasation into the hematoma being observed after administration of intravenous contrast, in relation with active bleeding. No visceral lesions were observed (Fig. 2).

The persistence of hemodynamic instability led to the case being commented with the Interventionist Radiography Service of the referring hospital and the patient being referred for embolization of the point of bleeding.
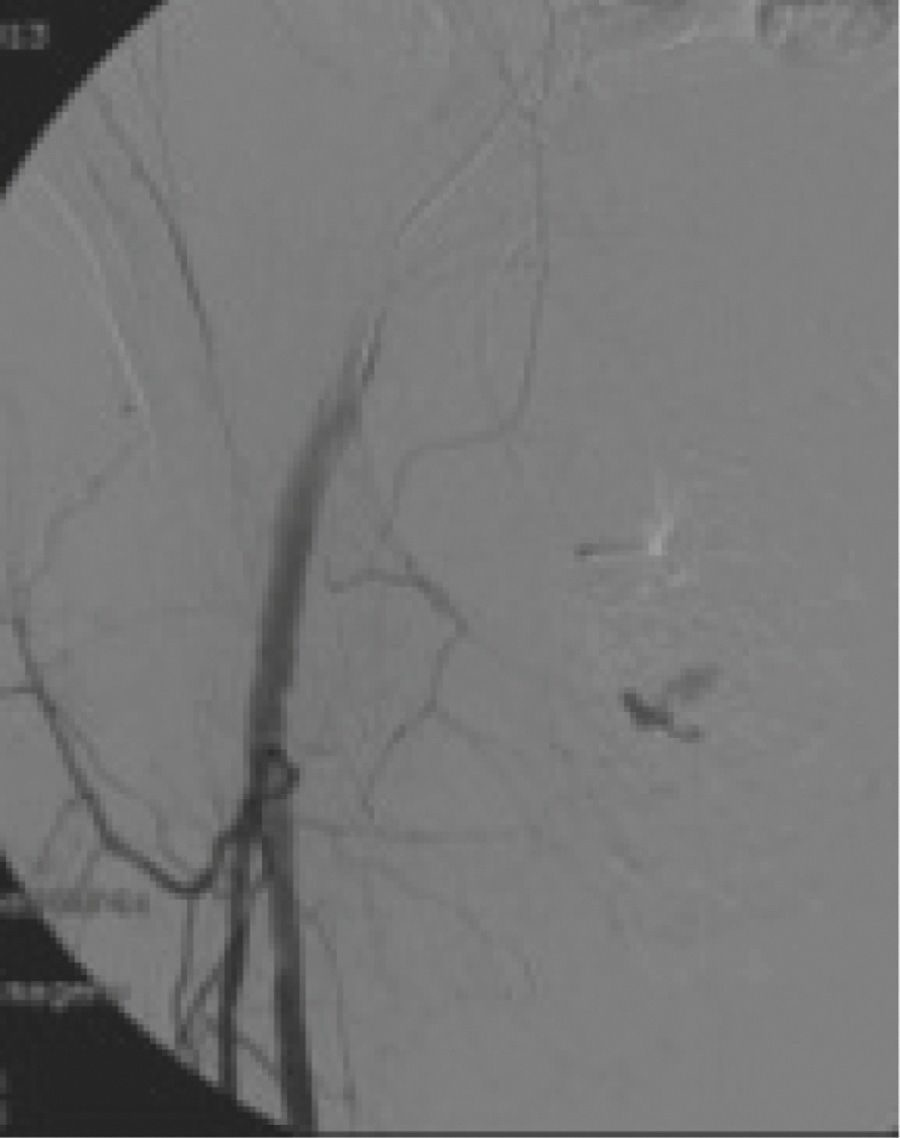
Once there, a pelvic arteriography and selective right external iliac and hypogastric arteriographies were obtained, which showed a focus of contrast extravasation in relation to active bleeding in the suprapubic region, to the expense of branches of the right inferior epigastric artery, which was selectively catheterized and embolized with a good result and with no signs of bleeding in the final control. The selective arteriography of branches of the anterior bifurcation of the right hypogastric artery presented a doubtful focus of bleeding, so it was also embolized with a satisfactory result (Fig. 3).

The subsequent evolution was satisfactory, and the patient began to walk with the aid of a walking frame after 3 weeks, with consolidation of the fracture being observed after 3 months.
DiscussionThe incidence of pelvic fractures ranges between 0.3% and 8%, which represents a low percentage with regard to the total number of fractures. Nevertheless, the number of pelvic fractures is significantly higher among the elderly.
The standard radiographic study of pelvic fractures must include an anteroposterior projection and entry and exit projections at 40°, as per Pennal et al.1 so as to assess rotational deformity and the anterior displacement of the hemipelvis in the case of entry projection, and vertical hemipelvis displacement and anterior pelvis widening or fracture in the case of exit projection. The CT study is not routinely necessary in low-energy fractures, whereas in high-energy fractures it enables assessment of the posterior part of the pelvic ring. Moreover, it is very helpful to assess rotational and anteroposterior displacement with greater precision than in radiographs.
Various classifications of pelvic fractures have been described, with the Tile classification, which divides them into 3 types based on pelvic stability after the lesion, being the most commonly used.
The most frequent complication is hemorrhage: this can occur during direct involvement of the large vessels of the pelvis by a fracture fragment, although the most common cause is bleeding from the fractured ends of the bone and the small retroperitoneal vessels.2 It is important to note that unstable fractures with displacements over 0.5cm are associated with a higher probability of severe hemorrhage.
Other, less frequent complications are located in the urogenital apparatus.
The treatment of non-displaced or minimally displaced fractures (Tile type A2) is usually conservative, based on relative rest between the bed and couch, control of symptoms and progressive gait with the help of a walking frame or crutches, depending on pain tolerance, and the evolution is toward healing without complications in the large majority of patients. Up to 63.6% of these fractures (especially A2 type) do not present significant soft tissue involvement, and only 3.9% of them require surgical stabilization.3 Soft tissue involvement is more frequent in A1 type cases, and can hinder the management of these type of patients.
Selective embolization of bleeding arteries is an effective procedure to stem bleeding, although it is not exempt from complications. Nevertheless, loss of blood added to ischemia caused by the embolization can lead to severe complications. Thus, the work by Matityahu et al.4 on 98 patients described an 11% rate of complications of which 6% were necrosis of the gluteal musculature, 5% presented suture dehiscence, 4% deep infections, 2% impotence, 1 case of superficial infection and 1 case of necrosis of the gall bladder. The risk of mortality for the embolized patients reached 20%. All the cases of gluteal necrosis presented a bilateral embolization.
On the other hand, Papakostidis et al.5 carried out a literature review and concluded that embolization is an efficient means to control severe arterial bleeding following pelvic fractures, with a low percentage of complications (1.1%). Occasionally, it becomes necessary to repeat the procedure in order to control the bleeding.
The presence of extravasated contrast in CT scans presents a high association with the need to carry out pelvic embolization in patients with pelvic fractures, although its absence does not preclude the need to carry out a pelvic angiography to confirm bleeding in suspected cases.6
ConclusionsLow-energy pelvic fractures can represent a vital risk, with selective embolization of the bleeding point being an effective method of control, although it can present severe complications.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation did not require experiments on humans or animals.
Confidentiality of dataThe authors declare that they have followed the protocols of their workplace on the publication of patient data.
Right to privacy and informed consentThe authors declare that this work does not reflect any patient data.
Level of evidenceLevel of evidence V.
Conflict of interestThe authors have no conflict of interest to declare.
Please cite this article as: Fernández-Lombardía J, Paz-Aparicio A, Hernández-Vaquero D. Complicación vascular tras fractura de ramas pélvicas. Rev Esp Cir Ortop Traumatol. 2014;58:407–410.
