





To study the concordance of the radiographic classification of Eaton–Littler for the diagnosis of basal thumb joint osteoarthritis (BTJO). The null hypothesis was that the concordance was due to chance and the alternative was that the concordance was not due to chance.
Material and methodWe have observed the X-rays of 46 patients with symptoms and clinical signs of BTJO. They were independently classified by five physicians: three experts in upper extremity, one in radiology and a fourth year resident of Orthopedics. We studied the concordance in the observations through the global kappa.
DiscussionThe diagnosis of BTJO is based primarily on clinical exploration, radiology is a complementary method of confirmation. The classification of Eaton–Littler proposes 4 stages of the disease, with a therapeutic involvement.
ConclusionsThe concordance of the radiographic classification of Eaton–Littler is moderate.
Estudiar la concordancia de la clasificación radiográfica de Eaton-Littler para el diagnóstico de la artrosis de la articulación trapeciometacarpiana (ATM). La hipótesis nula consideró que la concordancia era debida al azar, y la alternativa que la concordancia no era debida al azar.
Material y métodoSe estudiaron las radiografías de 46 pacientes con síntomas y signos clínicos de artrosis de la ATM. Se clasificaron independientemente por 5 facultativos: tres expertos en extremidad superior, uno en radiodiagnóstico y un residente en COT de cuarto año. Se estudió la concordancia de las observaciones mediante el índice kappa global.
DiscusiónEl diagnóstico de la artrosis de la ATM se basa fundamentalmente en la clínica, siendo la radiografía un método complementario de confirmación. La clasificación de Eaton-Littler propone 4 estadios evolutivos de la enfermedad, con una implicación terapéutica.
ConclusionesLa concordancia de la clasificación radiográfica de Eaton-Littler es moderada.
Osteoarthritis (or arthrosis) of the trapeziometacarpal joint (TMJ) (or basal thumb joint) (BTJ) is a disease present in a considerable percentage of the general population. The prevalence of symptomatic TMJ osteoarthritis is estimated at 6–8% of the population, although the prevalence of radiographic TMJ osteoarthritis is in the range of 29–76% according to the series.1 Both concepts are related to age and are more frequent among females.2 The diagnosis is essentially clinical, obtained through an adequate anamnesis and detailed physical examination. Imaging tests are very useful, both to confirm the diagnosis and to categorize the evolution of the disease.2,3
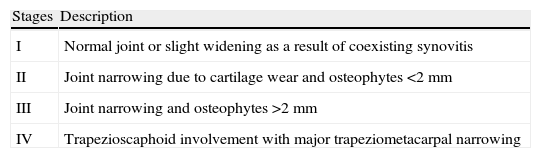
The Eaton–Littler classification, used extensively and based on the analysis of radiographic projections of the trapeziometacarpal joint, proposes 4 evolutionary stages for the disease, with implicit therapeutic relevance4 (Table 1).
Definition of the stages of trapeziometacarpal joint osteoarthritis according to the Eaton–Littler classification.
| Stages | Description |
| I | Normal joint or slight widening as a result of coexisting synovitis |
| II | Joint narrowing due to cartilage wear and osteophytes <2mm |
| III | Joint narrowing and osteophytes >2mm |
| IV | Trapezioscaphoid involvement with major trapeziometacarpal narrowing |
The present work studies the interobserver agreement in the Eaton–Littler classification through simple radiographic projections. The null hypothesis established is that the agreement is due to chance, whereas the alternative hypothesis is that the agreement is not due to chance.
Material and methodDataWe studied the posteroanterior, oblique in stress at 30° and lateral projections of the hands of 46 patients who required a surgical solution for symptoms related to osteoarthritis of the TMJ (Fig. 1A–D).
 Roberts projection (pronated anteroposterior); (B) posteroanterior projection of the TMJ; (C) lateral projection of the TMJ, and (D) oblique projection in stress at 30° of the TMJ.")
All the clinical histories (HP Doctor Hewlett-Packard Spain SA 2001, License HCE 2001) and images (Centricity® 9.5, General Electric, Fairfield, CT, USA) were digitalized. The treatment of data was protected by the Spanish Organic Law on Data Protection (LOPD) and European Directive 95/46/EC.5,6
ObserversThe observers were 3 orthopedic surgeons specializing in upper limb surgery, 1 physician specializing in radiodiagnosis and 1 traumatology and orthopedic surgery fourth-year resident physician. They assessed the compiled images and classified them according to the Eaton–Littler classification.3 The different assessments were collected in a table using the medical history number of each patient as a common key for each evaluation. The observers had no other data relating to patients (Table 2).
Assessment by observers.
| ID | TOS 1 | Rx | TOS 2 | TOS 3 | Res |
| 1 | 3 | 3 | 2 | 3 | 3 |
| 2 | 3 | 4 | 3 | 3 | 3 |
| 3 | 3 | 3 | 3 | 4 | 3 |
| 4 | 4 | 4 | 3 | 4 | 3 |
| 5 | 4 | 4 | 2 | 3 | 2 |
| 6 | 4 | 4 | 2 | 4 | 4 |
| 7 | 3 | 4 | 3 | 3 | 4 |
| 8 | 3 | 3 | 2 | 4 | 4 |
| 9 | 3 | 3 | 2 | 3 | 2 |
| 10 | 3 | 3 | 3 | 2 | 2 |
| 11 | 4 | 4 | 4 | 4 | 4 |
| 12 | 3 | 2 | 2 | 2 | 2 |
| 13 | 4 | 3 | 3 | 2 | 3 |
| 14 | 3 | 3 | 1 | 2 | 2 |
| 15 | 3 | 2 | 2 | 2 | 2 |
| 16 | 3 | 3 | 2 | 3 | 3 |
| 17 | 3 | 3 | 2 | 2 | 2 |
| 18 | 3 | 4 | 3 | 3 | 3 |
| 19 | 4 | 4 | 4 | 4 | 4 |
| 20 | 4 | 3 | 4 | 4 | 3 |
| 21 | 3 | 3 | 2 | 3 | 2 |
| 22 | 4 | 4 | 4 | 4 | 4 |
| 23 | 3 | 3 | 2 | 2 | 3 |
| 24 | 3 | 4 | 2 | 3 | 3 |
| 25 | 3 | 3 | 3 | 3 | 3 |
| 26 | 4 | 4 | 4 | 4 | 4 |
| 27 | 3 | 3 | 2 | 2 | 2 |
| 28 | 2 | 2 | 3 | 3 | 2 |
| 29 | 4 | 4 | 3 | 4 | 3 |
| 30 | 3 | 3 | 2 | 3 | 3 |
| 31 | 3 | 3 | 1 | 2 | 2 |
| 32 | 4 | 4 | 2 | 4 | 3 |
| 33 | 4 | 4 | 2 | 3 | 3 |
| 34 | 4 | 4 | 4 | 4 | 4 |
| 35 | 3 | 3 | 2 | 2 | 3 |
| 36 | 4 | 4 | 2 | 2 | 2 |
| 37 | 4 | 4 | 3 | 3 | 3 |
| 38 | 3 | 2 | 1 | 1 | 2 |
| 39 | 3 | 4 | 3 | 4 | 3 |
| 40 | 3 | 2 | 1 | 1 | 1 |
| 41 | 3 | 3 | 3 | 2 | 2 |
| 42 | 3 | 3 | 2 | 3 | 3 |
| 43 | 4 | 3 | 4 | 4 | 4 |
| 44 | 3 | 2 | 1 | 2 | 3 |
| 45 | 4 | 3 | 3 | 3 | 3 |
| 46 | 4 | 4 | 3 | 3 | 4 |
ID: patient; Res: resident physician in Traumatology and Orthopedic Surgery; Rx: specialist in radiodiagnosis; TOS 1–3: specialists in Traumatology and Orthopedic Surgery.
This classification defines 4 stages of the disease, although a fifth stage has been proposed to represent a situation of “pantrapezial osteoarthritis”.7 Nevertheless, the observers were limited to the original classification (Table 1).
Statistical analysisThe data were entered, coded and stored in a Microsoft Excel® spreadsheet (Windows 2007®, Microsoft Corp., Redmond, WA, USA), and then analyzed using the software package Epidat version 3.1. The statistical analysis was carried out using the kappa global index,8,9 establishing a hypothesis contrast in which the null hypothesis (H0) stated that the level of agreement was due to chance and the alternative hypothesis (H1) stated that it was not due to chance. Thus, 3 different scenarios were established. In the first we analyzed the results offered by the 3 orthopedic surgeons specializing in the upper limbs. In the second, we analyzed the results from the same 3 observers, plus those from the specialist in radiodiagnosis. Lastly, we added the assessments obtained from the traumatology and orthopedic surgery resident physician, and analyzed the results from all 5 observers.
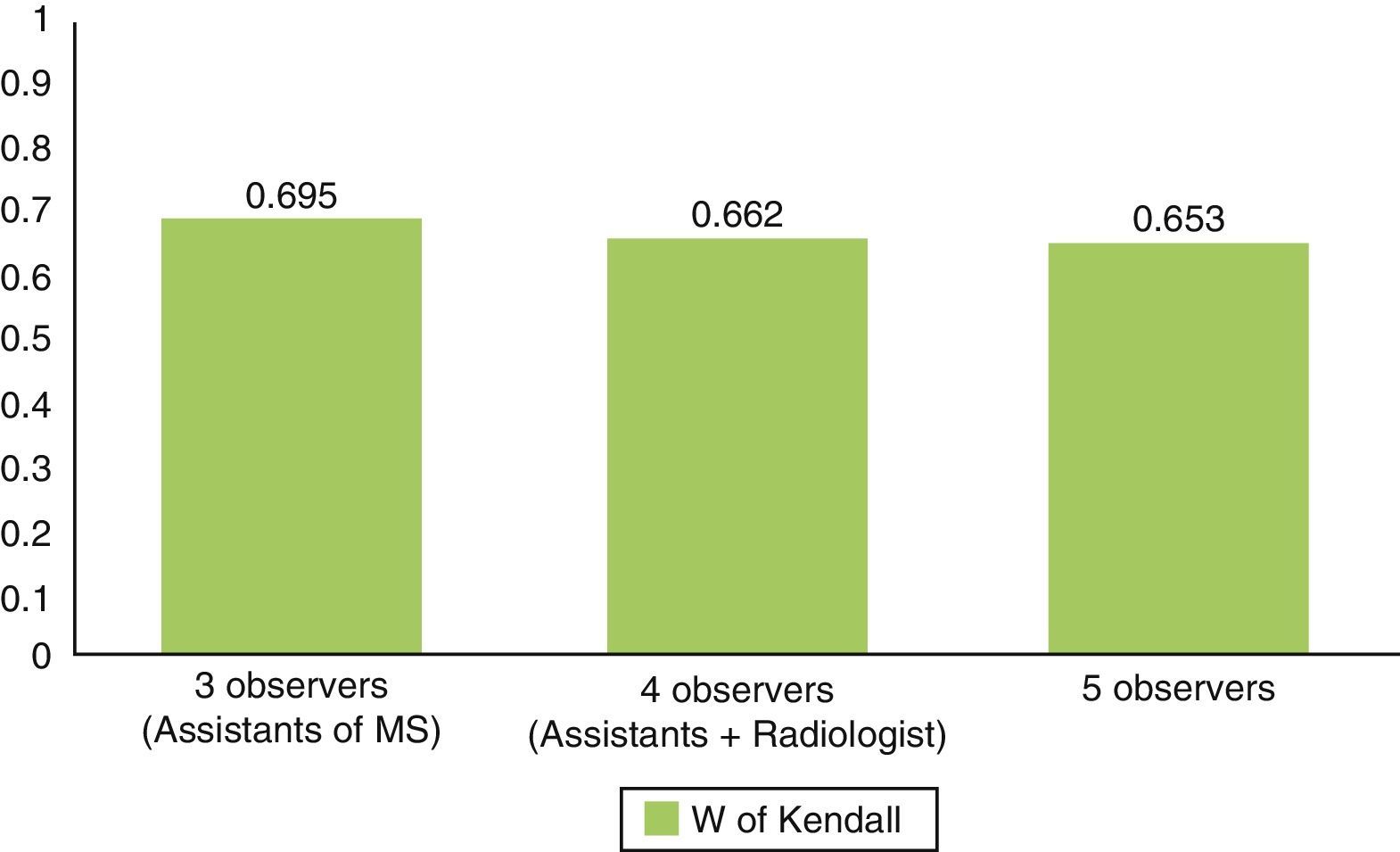
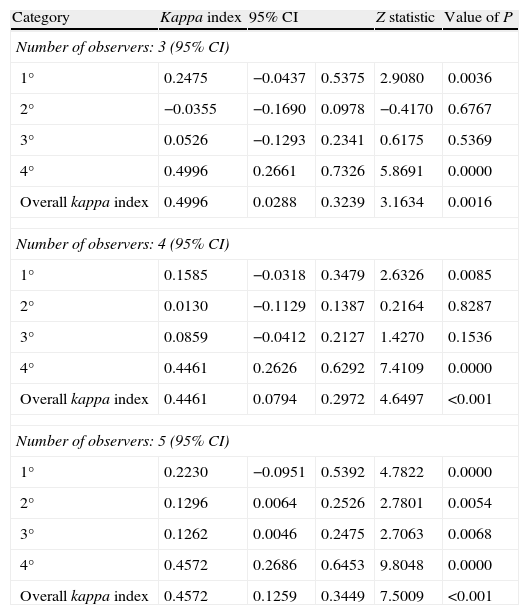
ResultsWe took a sample of 46 patients with a diagnosis of TMJ osteoarthritis, of which 37 were females (80.4%) and 9 were males (19.6%). We assessed the following scenarios: first scenario; kappa global index: 0.4996; P=.0016; second scenario: kappa global index: 0.4461; P<.001, and third scenario: kappa global index: 0.4572; P<.001 (Table 3, Fig. 2). The kappa global index reached a moderate value in a statistically significant manner in all cases.10 This means that the null hypothesis may be ruled out and we can state that the level of agreement reached by the observers was not due to chance.
Level of agreement in the different scenarios.
| Category | Kappa index | 95% CI | Z statistic | Value of P | |
| Number of observers: 3 (95% CI) | |||||
| 1° | 0.2475 | −0.0437 | 0.5375 | 2.9080 | 0.0036 |
| 2° | −0.0355 | −0.1690 | 0.0978 | −0.4170 | 0.6767 |
| 3° | 0.0526 | −0.1293 | 0.2341 | 0.6175 | 0.5369 |
| 4° | 0.4996 | 0.2661 | 0.7326 | 5.8691 | 0.0000 |
| Overall kappa index | 0.4996 | 0.0288 | 0.3239 | 3.1634 | 0.0016 |
| Number of observers: 4 (95% CI) | |||||
| 1° | 0.1585 | −0.0318 | 0.3479 | 2.6326 | 0.0085 |
| 2° | 0.0130 | −0.1129 | 0.1387 | 0.2164 | 0.8287 |
| 3° | 0.0859 | −0.0412 | 0.2127 | 1.4270 | 0.1536 |
| 4° | 0.4461 | 0.2626 | 0.6292 | 7.4109 | 0.0000 |
| Overall kappa index | 0.4461 | 0.0794 | 0.2972 | 4.6497 | <0.001 |
| Number of observers: 5 (95% CI) | |||||
| 1° | 0.2230 | −0.0951 | 0.5392 | 4.7822 | 0.0000 |
| 2° | 0.1296 | 0.0064 | 0.2526 | 2.7801 | 0.0054 |
| 3° | 0.1262 | 0.0046 | 0.2475 | 2.7063 | 0.0068 |
| 4° | 0.4572 | 0.2686 | 0.6453 | 9.8048 | 0.0000 |
| Overall kappa index | 0.4572 | 0.1259 | 0.3449 | 7.5009 | <0.001 |
95% CI: 95% confidence interval.
.")
TMJ osteoarthritis should be considered as an idiopathic primary disorder, so as to distinguish it from cartilage degeneration taking place in other diseases classically known as inflammatory arthropathies, such as rheumatoid arthritis and seronegative arthropathies. TMJ osteoarthritis represents one of the main causes of orthopedic consultation due to pain in the hand.11,12 The trapeziometacarpal joint is the second most commonly affected joint in the first finger, following the distal interphalangeal joint, but it causes greater functional involvement.
The diagnosis of TMJ osteoarthritis is mainly based on the symptoms, with radiographs being a complementary confirmation method. Clinically, these patients present pain at the level of the trapeziometacarpal joint and functional limitation which mainly results in reduced grasping amplitude and loss of lateral pincer movement, which leads to an inability to perform basic activities of daily living, such as turning a key, brushing teeth, grasping objects in an elevated position, opening a jar, etc.7
In general, assessment of this disease through imaging tests has been carried out following the Eaton–Littler classification,7 which is based on specific projections from conventional radiography. Although radiodiagnostic tests have undergone a considerable evolution since this classification was first proposed, it is still very applicable. Therefore, conventional radiography is the standard test for the assessment of TMJ osteoarthritis. Far from being purely descriptive, the Eaton–Littler classification entails therapeutic implications13 which depend on the evolutionary stage of the disease.
Therefore, given the therapeutic implications derived from a correct classification, a precise diagnostic test is considered essential,14 understanding as such those tests with consistent results which correspond to reality when applied once again under similar circumstances. The precision of a procedure depends on 2 variables: the variability inherent to the procedure itself and that inherent to the examiner. Moreover, the precision of the observations can be assessed in different manners depending on the type of agreement being studied (intraobserver, interobserver, etc.).15 An interobserver agreement study is one of the parameters employed to assess the reliability of a diagnostic tool.
In this work we have assessed the level of interobserver agreement in simple radiography as a tool for the diagnosis and classification of TMJ osteoarthritis. Coinciding with other published works, we obtained a moderate level of agreement in the 3 scenarios established.16 Since we also obtained statistical significance, we can assert that the agreement among observers was not due to chance. Conventional radiography represents a reliable procedure for the diagnosis and classification of TMJ osteoarthritis, so the use of other tests, like magnetic imaging resonance scans,17 provides a less cost-effective diagnosis.
Level of evidenceLevel of evidence III.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation did not require experiments on humans or animals.
Confidentiality of dataThe authors declare that they have followed the protocols of their workplace on the publication of patient data and that all patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that this work does not reflect any patient data.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Hirschfeld M, Galán A, Arenas J, del Águila B, Benitez-Parejo N, Costa J, et al. Concordancia interobservador de la clasificación de Eaton-Littler de la artrosis trapeciometacarpiana. Rev Esp Cir Ortop Traumatol. 2014;58:237–241.
