



The objective of the present study is to characterise the epidemiological and legal data on medical malpractice ruled by the Chilean Supreme Court (CSC) in the years 2014 and 2015.
Material and methodA search of the CSC electronic database was conducted to identify and analyse CSC rulings for criminal and civil medical malpractice cases.
ResultsA total of 110 malpractice cases were identified. The CSC received only civil cases of medical malpractices during the studied period. The average duration of the trial was 39 months. Gynaecologists faced suits more frequently than any other type of specialist. The majority of cases were associated with the public health system. More claims were associated with scheduled than with emergency care. Likewise, more claims were associated with non-surgical treatment than with surgical procedures. More than a third (39%) of the cases resulted in the patient's death. The majority of CSC rulings were in favour of the defendants.
ConclusionsAn urgent analysis of the risk factors is necessary, not only of the occurrence of malpractice, but also of doctor–patient conflicts by judicial means, especially in the gynaecological-obstetrics area. In addition, considering that the trials not only involve a high economic cost, but also psychological and emotional one, for all involved, an analysis of the judicial mechanisms of these types of cases could help resolve them, and when possible, in preliminary courts or in shorter judicial processes, benefiting all parties.
Analizar los datos epidemiológicos y jurídicos de los casos por responsabilidad médica fallados por la Corte Suprema de Justicia chilena los años 2014 y 2015.
Material y métodoSe realizó un estudio retrospectivo, revisando los fallos de la Corte Suprema de Justicia en la base de datos electrónica del Poder Judicial chileno. Se seleccionaron y analizaron los fallos por responsabilidad médica.
ResultadosSe detectó un total de 110 casos por responsabilidad médica. Todos correspondieron a causas civiles. La duración promedio de los procedimientos fue de 39 meses. La especialidad más demandada fue ginecología. La mayoría de las demandas afectó al Sistema Público de Salud. Los casos que dan origen a las demandas son, en su mayoría, de atención programada frente a los de urgencias, y de tratamiento frente a procedimientos quirúrgicos. El 39% de los casos resultaron en muerte del paciente. La mayoría de las demandas resultó desfavorable para los demandantes.
ConclusionesSe requiere un urgente análisis de los factores de riesgo, no solo de la ocurrencia de mala praxis, sino de la judicialización de los conflictos médico-paciente, especialmente en el área ginecoobstétrica. Además, dado que los juicios conllevan un alto coste no solo económico, sino también psicológico y emocional para todos los involucrados, un análisis de los mecanismos judiciales propios de este tipo de casos podría contribuir a que estos se resolvieran, en la medida de lo posible, en instancias prejudiciales o en procesos judiciales más cortos, beneficiando a todos los involucrados.
In recent decades, advances in medicine have made medical action increasingly more complex. This, together with changes in the doctor–patient relationship, and the empowerment of health service users, has lead to the ever-more-common judicialisation, both nationally and internationally, of the inevitable problems that arise during medical care.1
Medical liability is the obligation of medical professionals to repair, respond to and compensate for damage caused to patients as the result of faults committed during exercise of their profession. Professional liability has been required of all professionals throughout history. In medicine, we find antecedents in the Hammurabi Code, in the legislation of the Romano-Germanic Empire, in the Carolingian Code and in Henry the Eighth's England, to name but a few.2,3
Under Chilean law, doctors are subject to different types of liability, each of which has a specific legal regime4:
- –
Criminal liability seeks to punish health professionals who fail to comply with the medical Lex Artis with a custodial sentence.5,6
- –
Civil liability obliges physicians to pecuniary compensation for damage caused, public health institutions for a lack of service and private institutions for negligent failure to comply with their oblications.7
- –
Administrative liability falls to the physician working in a public health facility due to contravention of the Administrative Statute.8
Legal doctrine sets a series of requirements to produce a quasi-delict of medical liability with extra-contractual liability, namely: the author must hold a professional title, the damage must have been caused in an act inherent to professional activity, there must be objectifiable damage to the patient, there must be a causal relationship between the act and the professional must have acted with fault.2,4,7
Criminal medical liability claims only reach the Chilean Supreme Court (CSC) in the event that the second instance judgement (Court of Appeal) infringes rights guaranteed under the Constitution or under international treaties ratified by Chile.5
Civil medical liability claims can be appealed by either party by submitting an appeal in cassation to the Supreme Court, either in form or in substance.7
The objective of this study was to analyse the epidemiological and legal data of medical liability cases decided by the Supreme Court in 2014 and 2015. The judgements of the CSC were selected because it is the highest court in the Chilean justice system, and therefore its judgements are conclusive and irrevocable.
Material and methodsA qualitative, retrospective study. A search was carried out for CSC rulings during the years 2014 and 2015. For this purpose, the electronic database of the Judiciary Branch was accessed.9 Proceedings related to the provision of medical services were selected, In reviewing them in detail, the following information was extracted:
- –
Characteristics of the intervening parties: sex and age of the patient; sex and age of the plaintiff; sex, age and specialty of the treating professional; type of health system; and the respondent institution or health personnel.
- –
Clinical criteria: type of care, medical procedure and outcome.
- –
Legal criteria: type of trial, subject matter and duration of trial, first instance, Court of Appeal and Supreme Court judgements.
An Excel spreadsheet was used to record the data. Stats and absolute and relative frequencies were used for the descriptive analysis.
ResultsOver the period studied, a total of 55,360 CSC rulings were recorded, of which 110 were on grounds of medical liability (.2%); 38 cases were adjudicated in 2014 and 72 cases in 2015. A record was found of 2 rulings for the same case, recording only one.
Characteristics of the intervening partiesThe distribution by sex of the patients affected, out of a universe of 111 people, was 46.8% males and 53.2% females. Age was reported only in 17 cases and ranged from 0 to 83 years.
The plaintiffs were mostly female (55.9%).
The sex of the defendant physician was reported in 53 cases, and 59 physicians were involved. Of the defendants, 83.1% were men, while only 16.9% were women.
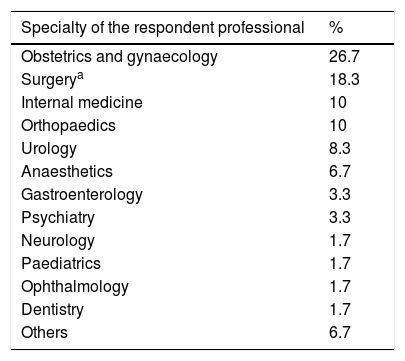
The specialty of the respondent physician was reported in 57 cases, and 60 specialists were involved. The percentage distribution of the respondent specialties is shown in Table 1.
Specialties affected by rulings of the Chilean Supreme Court, between 2014 and 2015.
| Specialty of the respondent professional | % |
|---|---|
| Obstetrics and gynaecology | 26.7 |
| Surgerya | 18.3 |
| Internal medicine | 10 |
| Orthopaedics | 10 |
| Urology | 8.3 |
| Anaesthetics | 6.7 |
| Gastroenterology | 3.3 |
| Psychiatry | 3.3 |
| Neurology | 1.7 |
| Paediatrics | 1.7 |
| Ophthalmology | 1.7 |
| Dentistry | 1.7 |
| Others | 6.7 |
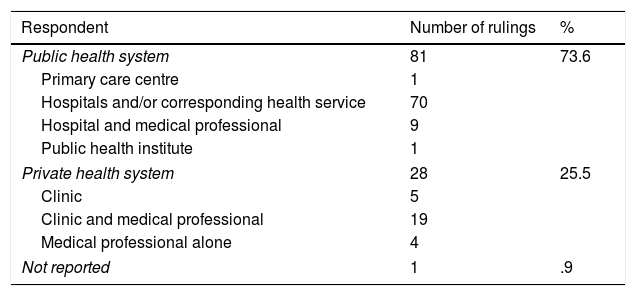
Most of the claims were against the Public Health System, at 73.6% of the total. The breakdown is shown in Table 2.
Respondent in cases decided by the Chilean Supreme Court between 2014 and 2015.
| Respondent | Number of rulings | % |
|---|---|---|
| Public health system | 81 | 73.6 |
| Primary care centre | 1 | |
| Hospitals and/or corresponding health service | 70 | |
| Hospital and medical professional | 9 | |
| Public health institute | 1 | |
| Private health system | 28 | 25.5 |
| Clinic | 5 | |
| Clinic and medical professional | 19 | |
| Medical professional alone | 4 | |
| Not reported | 1 | .9 |
Of the total 110 cases, 56.4% corresponded to scheduled care, and 43.6% to emergency care. Surgical interventions accounted for 46.4%, and non-surgical medical procedures for 53.6%.
The medical procedure resulted in the death of the patient in 43 cases (39.1%), physical sequelae in 44 cases (40%), and moral damage claim in 23 cases (20.9%).
Of the total 43 patients who died, 69.8% were adults (over 18 years of age), and the rest were children or foetuses. Forty-five point two percent were males, 31% were females and 23.8% foetuses, whose sex was not recorded in the claim.
Of the deaths, 83.3% occurred in public hospitals. Gynaecology was the specialty most affected by patient death at 26.2%, followed by internal medicine (9.5%) and orthopaedics (7.1%).
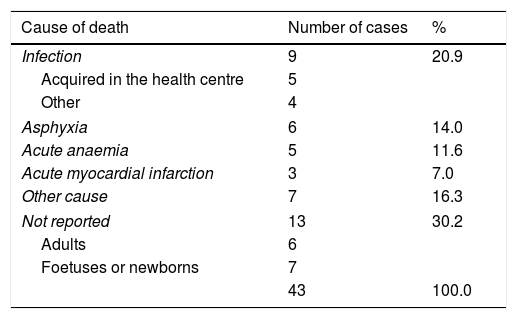
The most frequent causes of death are shown in Table 3.
Causes of death in cases ruled by the Chilean Supreme Court, between 2014 and 2015.
| Cause of death | Number of cases | % |
|---|---|---|
| Infection | 9 | 20.9 |
| Acquired in the health centre | 5 | |
| Other | 4 | |
| Asphyxia | 6 | 14.0 |
| Acute anaemia | 5 | 11.6 |
| Acute myocardial infarction | 3 | 7.0 |
| Other cause | 7 | 16.3 |
| Not reported | 13 | 30.2 |
| Adults | 6 | |
| Foetuses or newborns | 7 | |
| 43 | 100.0 | |
All the judicial proceedings were civil suits for damages. Their average duration was 39 months. Of the 110 rulings, 58.2% were unfavourable for the plaintiffs, and 41.8% favourable. On breaking down the cases according to the outcome of the medical care, we found that when the outcome was the death of the patient the decision was favourable in 46.5% of cases; when the outcome was a physical sequela the decision was favourable in 40%, and when moral damage was alleged, the decision was favourable in 34.8%.
DiscussionThere are several international studies that characterise different aspects of judgements in medical liability cases in the different judicial instances or preliminary claims.10–15 the Supreme Court is the highest court in the different legislations, and therefore its rulings are conclusive and irrevocable. Given the importance of these decisions, we preferred to collect these data for preparing this study, since this is the first of its kind in Chile. On an international level there are the studies by Wu et al. on last-instance judgements.16,17
There are several interesting findings that are worthy of mention in this study.
The proceedings originated exclusively in civil justiceThe fact that there were no judgements originating in the criminal justice system in the period studied is striking. An important reason for this could be that there are very few grounds for a decision of the first instance courts to be reviewed by the CSC. On the other hand, it is also possible that plaintiffs prefer to bring their charges exclusively through civil proceedings, with a view to receiving greater monetary compensation.18
The judicialisation period of the cases was very longThe proceedings reaching the CSC took, on average, 39 months to be completely closed, with a maximum of 118 months. During this period, which can last up to 9 years, the accused physician lives with the burden of this stressful process, which can interfere with his/her clinical practice and emotional state, as defined by Hurtado Hoyo in 1993 termed “Judicial Clinical Syndrome” to describe “all the disturbances that modify the state of health of a subject who is undergoing litigation, be it at the beginning (arraignment, summons, court orders), during the ensuing steps of it, and/or after it.” “It encompasses all physical, mental and moral disturbances that can occur”.19,20 As a consequence, defensive medicine is generated, i.e., the medical professional prescribes diagnostic and/or therapeutic procedures mainly with a view to protecting him/herself from possible future litigation, rather than effectively contributing to the diagnosis and/or treatment of their patients.21 Even if the physician has civil liability insurance that partially covers the amount of compensation, nothing compensates for the emotional wear and tear or loss of professional reputation to which he or she will be exposed.15 Likewise, it is exhausting for the plaintiff to have to wait for so long with no response to their claim.
Most claims were made against the Public Health SystemA plausible hypothesis to explain this fact could be the greater bargaining power of private entities, when offering compensatory payment in the first judicial instance or, even in preliminary hearings. Likewise, it is plausible that plaintiffs perceive that the State can compensate them for a much higher amount than a professional alone. This would also explain why it is all the more common for a lawsuit to be directed against the Health Services rather than the doctor responsible for the procedure being litigated.
Most affected specialitiesOf the results obtained in this study, it is striking that most of the cases that reached the CSC were due to care in the area of obstetrics and gynaecology (26.7%), which is also the area most affected by the death of a patient.
There is further history in this regard in Chile:
The Legal Department of the Fundación de Asistencia Legal del Colegio Médico de Chile reported in their 2011–2016 executive account that 278 malpractice trials were completed in 2015, defended by them. The specialties with the most claims were general medicine (20.5%), obstetrics and gynaecology (20.14%) and surgery (19.78%).10
Moscoso and Smok reported, in their 2015 study, that among the requests for expert opinion submitted to the Medical Liability Unit of the Chilean Legal Medical Service (SML), the specialties most affected were Gynaecology (24.8%), Surgery (14.5%) and Internal Medicine (13.1%).11
We found international studies on cases of medical malpractice that use the databases of insurance companies. In Spain, for example, Arimany-Manso (2013), with data from the Professional Liability Service of the General Council of Medical Associations of Catalonia, reported that of a total of 5246 cases of malpractice claims closed between 1986 and 2005, the most affected specialties were orthopaedic surgery and trauma at 15.7%, obstetrics and gynaecology at 12.5%, and general surgery at 7.7%.12
In Taiwan, Wu (2018) reported that between 2002 and 2013, of a total 946 medical liability suits closed in their district courts, the 3 most affected specialties were obstetrics (10.7%), orthopaedics (9.8%) and emergency medicine (8.5%).13
It is interesting to note that, regardless of the source of the data used in the different studies cited (expert opinion, claims to insurance companies, different judicial instances), the specialty of gynaecology is one of the most affected by claims in all cases. It is necessary to research the causes of this concerning situation to guide medical professionals in prevention.
Limitations of the studyThis study has certain limitations that merit comment.
Firstly, the information available on CSC rulings was analysed, with no access to the complete clinical history of each case, and therefore our vision of these cases was often limited. Statistical data were not always available, such as the sex and age of the plaintiffs and defendants, or the medical specialty of those involved, which prevented a thorough analysis of each case and detection of risk factors for claims against clinical care.
Furthermore, the claims brought before the CSC represent only a fraction of all the claims for medical practice. Studies on judicialised cases in previous instances should be conducted to complete the picture. However, it should be noted again that the decisions of the CSC are final and irrevocable, and therefore this is information that is indubitably useful for analysing the issue.
ConclusionsFrom analysis of the medical liability cases ruled by the CSC in Chile, and in accordance with much observed in the international literature, it is clear that urgent analysis of the risk factors is required, not only of malpractice, but of the judicialisation of doctor–patient conflicts, especially in the area of obstetrics and gynaecology, the area most affected by these types of problems in Chile.
In addition, given that trials involve high costs, not only financial, but also psychological and emotional, for all those involved (the State, public and private health institutions, medical professionals, patients and their families), an analysis of the judicial mechanisms inherent to these types of cases could help in resolving them, as far as possible, in preliminary hearings or in shorter judicial processes, to the benefit of all involved.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Raineri Bernain G, Bravo Rodríguez L, Lagos Tissie D, Ciocca Gómez L. Análisis de los fallos de la Corte Suprema de Justicia de Chile en casos de responsabilidad médica, años 2014 y 2015. Rev Esp Med Legal. 2019;45:108–113.