



A 19-year-old man presented with abdominal pain for 6 months. Abdominal enhanced CT showed extensive irregular soft tissue masses in the pelvic cavity and thickening of the peritoneum, with inhomogeneous enhancement. Abdominal puncture biopsy revealed desmoplastic small round-cell tumor (DSRCT). Subsequently, four cycles of chemotherapy (cisplatin plus etoposide) were performed. However, the patient reported experiencing discomfort including thrombocytopenia, leukopenia, nausea, and vomiting after chemotherapy. Thus, chemotherapy was stopped. Then, the patient was admitted to our hospital. With the patient's informed consent, he was included in the clinical trial of 68Ga-FAPI-04 PET/CT in tumors. The MIP image of 68Ga-FAPI PET/CT (Fig. 1) revealed increased FAPI uptake in the pelvic cavity (solid arrow) and lower abdomen (dotted arrows), which showed the irregular soft tissue masses with intense uptake (SUVmax, 7.9) in the pelvic cavity (solid arrows). Diffuse thickening of the peritoneum (dotted arrows) with increased tracer uptake (SUVmax, 6.8) was also observed. The PET/CT finding were consistent with DSRCT. Subsequently, the patient received 177Lu-FAP2286 therapy (dose of 7.4 GBq, first cycle) with stable disease. Further follow-up is still under observation.
 image of 68Ga-FAPI PET/CT revealed increased FAPI uptake in the pelvic cavity (solid arrow) and lower abdomen (dotted arrows). On the axial (B), coronal (C), and sagittal (D) images of PET/CT images showed the irregular soft tissue masses with intense uptake (SUVmax, 7.9) in the pelvic cavity (solid arrows). Diffuse thickening of the peritoneum (dotted arrows) with increased tracer uptake (SUVmax, 6.8) was also observed (upper row: PET; middle row: CT; lower row: fused PET/CT).")
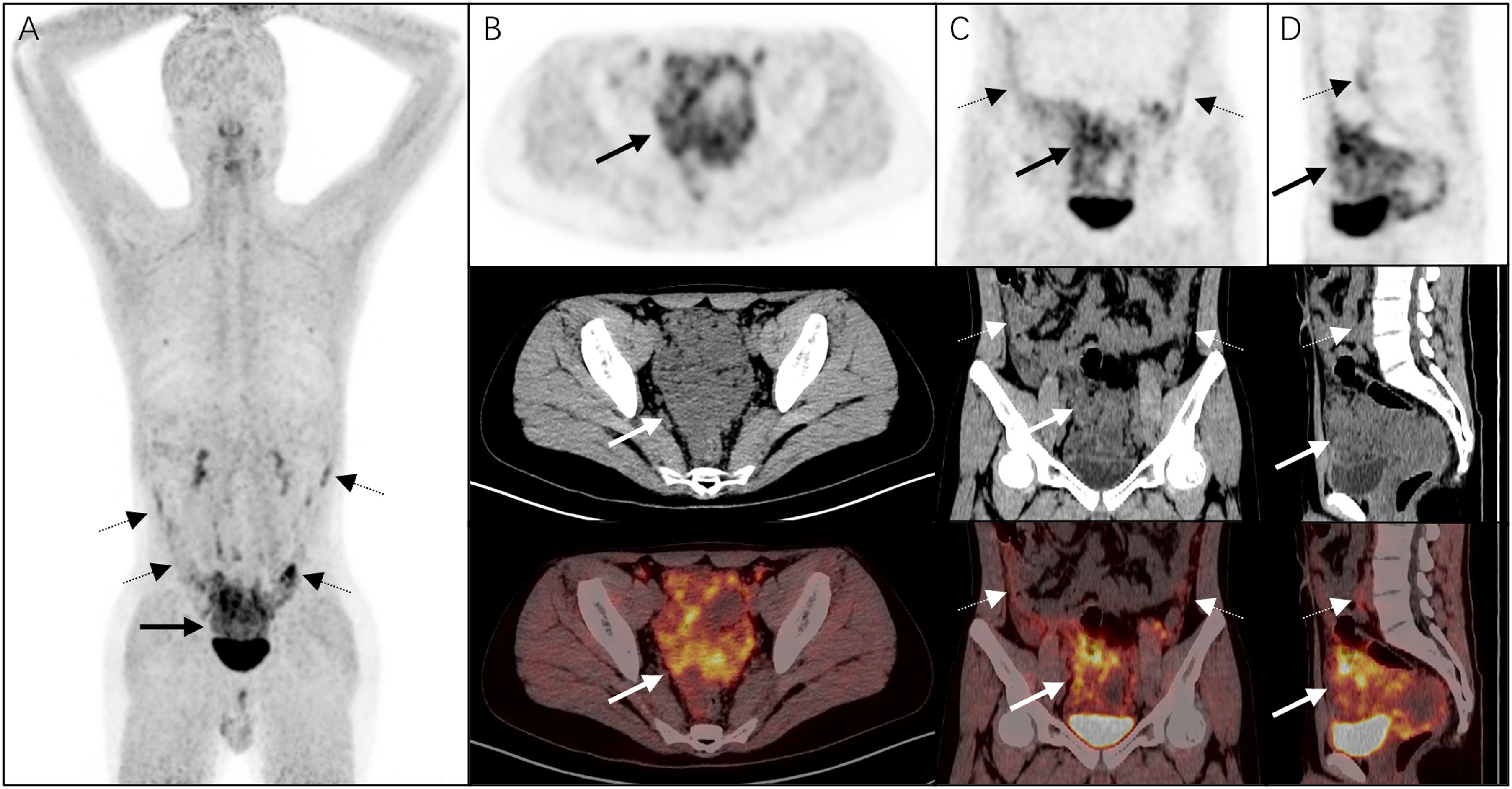
The MIP (A) image of 68Ga-FAPI PET/CT revealed increased FAPI uptake in the pelvic cavity (solid arrow) and lower abdomen (dotted arrows). On the axial (B), coronal (C), and sagittal (D) images of PET/CT images showed the irregular soft tissue masses with intense uptake (SUVmax, 7.9) in the pelvic cavity (solid arrows). Diffuse thickening of the peritoneum (dotted arrows) with increased tracer uptake (SUVmax, 6.8) was also observed (upper row: PET; middle row: CT; lower row: fused PET/CT).
DSRCT is a rare, highly aggressive malignancy, that predominantly occurs in adolescents, and it often presents as multiple uneven density masses in the abdominal and pelvic cavities, involving the peritoneum and abdominal lymph nodes, lacking a definite organ origin.1 Thus, DSRCT is difficult to distinguish from other abdominal tumors. Furthermore, previous studies have preliminarily shown that 18F-FDG PET/CT is essential for the diagnosis, staging, and management of DSRCT.2 However, sometimes it cannot distinguish between certain infections and malignant tumors, and due to the physiological uptake of FDG in the gastrointestinal tract, this may limit its use in certain situations. 68Ga-FAPI is based on the molecular targeting of the FAP, known to be highly expressed in the major cell population in tumor stroma,3 which might be considered as the preferred imaging modality for monitoring DSRCT patients. Meanwhile, our case suggests that 68Ga-FAPI PET/CT may also be helpful in guiding the precise therapy of 177Lu-FAP2286 in DSRCT.
Ethical statementAll procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Conflicts of interestNone declared.
Informed consentWritten informed consent for publication of this report was obtained from the patient.
