



Tracheobronchial tree is reported to harbor benign processes like inflammatory origin, foreign bodies, pulmonary aspirations, mucous plugs and benign tumors (most of them of mesenchymal origin), as well as malign processes: primary (of epithelial origin), and secondary (by direct infiltration or hematogenous spread).1,2
We report a patient with history of squamous carcinoma in the right lung (stage IIIB), who was treated with chemotherapy and radiotherapy in 2008, with complete morphological response being achieved. On a follow-up CT 5 years later, a nodule in upper lobe of the left lung was detected together with tracheal and main bronchial mucosa thickening, thought to be mucous secretion. A PET/CT study with 18F-FDG was performed 3 days later to characterize metabolically the pulmonary nodule, as well as the thickening of the tracheobronchial mucosa, for disease restaging purposes.
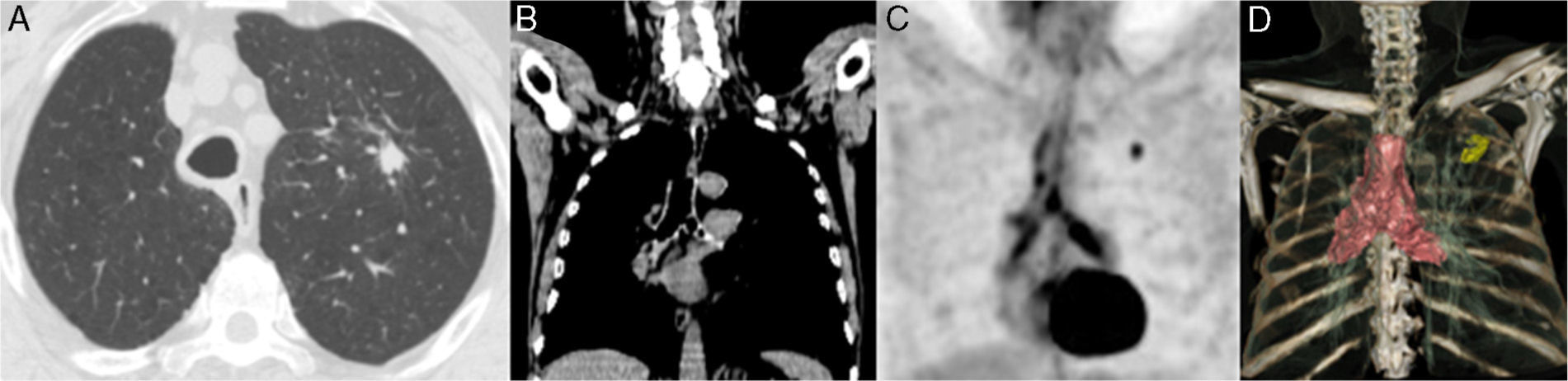
PET/CT images with 18F-FDG showed intense uptake in pulmonary nodule, consistent with malignancy. Diffuse uptake was also depicted in trachea and main bronchi, suggestive of malignant origin (Fig. 1C and D. PET and PET/CT volumetric three-dimensional 3D reconstruction).
 Axial CT slice with lung window. (B) Sagital CT slice with mediastinum window. (C) PET imaging, volumetric 3D reconstruction. (D) PET/CT imaging, volumetric 3D reconstruction. A 13mm nodule with spiculated margins in left upper lobe of lung (A) is seen, with metabolic uptake consistent with malignancy (maximum SUV 5.4) (C and D). Mucosa thickening of trachea and major bronchi is also seen, that may be due to mucous secretion or malignancy (B). PET imaging show diffuse high uptake in trachea and major bronchi (SUVmax 5.9) that corresponds with thickening of tracheobronchial mucosa, and thus suggesting malignancy again (C and D).")
(A) Axial CT slice with lung window. (B) Sagital CT slice with mediastinum window. (C) PET imaging, volumetric 3D reconstruction. (D) PET/CT imaging, volumetric 3D reconstruction. A 13mm nodule with spiculated margins in left upper lobe of lung (A) is seen, with metabolic uptake consistent with malignancy (maximum SUV 5.4) (C and D). Mucosa thickening of trachea and major bronchi is also seen, that may be due to mucous secretion or malignancy (B). PET imaging show diffuse high uptake in trachea and major bronchi (SUVmax 5.9) that corresponds with thickening of tracheobronchial mucosa, and thus suggesting malignancy again (C and D).
Considering the hypermetabolic thickening of tracheobronchial mucosa, bronchoscopy was performed 5 days later, which showed mamelon-like appearance on a thickened tracheal lining, as well as mucosa breakdown of both major bronchi, with mucous mamelons that caused narrowing of bronchial lumen, mostly on right tree, as well as total obstruction of right upper lobe lumen. Bronchial biopsy, brush cytology and bronchoalveolar lavage were all positive for squamous carcinoma.
Several CT appearances have been described for lung malignancies: polyploid, sessile, asymmetric narrowing of bronchial lumen, or round thickening of wall. There are also specific CT findings for benign tumors like popcorn calcifications in hamartoma and fat density in lipoma. However, despite of high CT sensitivity for the detection of endobronchial lesions, specificity for differentiating benign from malignant obstructive disease is low.1,2
In this setting, hybrid PET/CT allows also for characterization of 18F-FDG uptake in lung lesions. Most of benign endobronchial lesions show low or absent tracer uptake (due to low cellularity or fibrosis), whereas malignancies show high metabolic uptake.3
In our case, metabolic characterization with 18F-FDG PET of morphological findings with CT allowed for the diagnosis of malignant diffuse infiltration of the tracheobronchial tree. Availability of volumetric 3D reconstruction with PET and PET/CT resulted in powerful images with high diagnostic performance.
Please cite this article as: Garcia JR, Sanchez R, Bassa P, Moragas M, Soler M. Infiltración difusa del árbol traqueo-bronquial diagnosticada por tomografía por emisión de positrones/tomografía computada con 18F-fluordesoxiglucosa. Rev Esp Med Nucl Imagen Mol. 2015;34:213–214.
