



Cervix cancer usually spreads through direct local extension and via the lymphatics, haematogenous metastasis is relatively infrequent and cutaneous metastases are very rare with a reported incidence ranging from 0.1 to 2%.1–3 Subcutaneous metastasis of certain malignant diseases such as gastric cancer, esophageal cancer, colorectal cancer and breast cancer have been detected with 18F-fluoro-2-deoxyglucose positron emission tomography/computed tomography (FDG-PET/CT).3 This is a rare case with subcutaneous metastases from cervix cancer detected with PET/CT.
Skeletal muscle involvement from cervical carcinoma is very rare, and usually documented in the context of an already far advanced stage tumor. The incidence of skeletal muscle metastases in cervix carcinoma is reported to be less than 1% of metastases of haematogenous origin. The most frequent site being the psoas muscle; however metastasis to masseter, intercostals, biceps and deltoid muscles have also been reported.3 Malignancies known to frequently metastasize to the muscle are melanoma, kidney, lung, thyroid cancer; moreover skeletal muscle metastases have been also reported in lymphoma, leukaemia and colon cancer patients.3
A 46-year-old woman with carcinoma of the cervix was treated with chemo-radiation therapy. Six months later during follow up, FDG-PET/CT (Siemens Biograph 6, Chicago, USA) imaging was applied for restaging. FDG-PET/CT images were obtained approximately 60min after the intravenous injection of 10mCi (370MBq) FDG. Prior to the examination, 40ml of ionic iodinated contrast agent diluted in 1500ml of water was given to patient orally. No other iv contrast material was used for the CT scans.
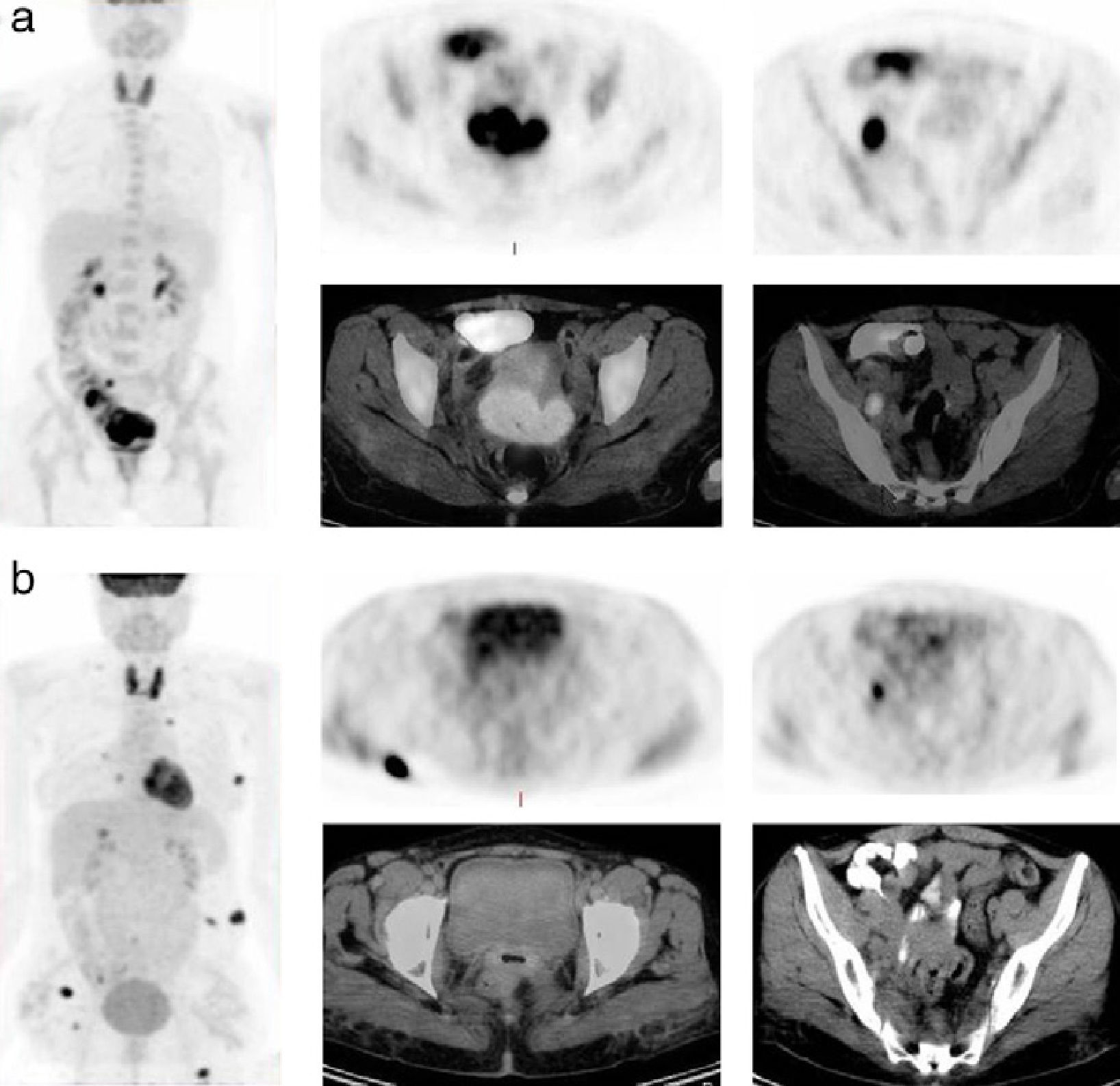
Pretreatment maximum-intensity projection (MIP) of FDG-PET/CT data showed increased heterogeneous FDG uptake (maximum standardized uptake values (SUVmax): 15.3) within large cervical mass together with internal and external iliac lymph nodes (Fig. 1a). Post-treatment MIP of FDG-PET/CT data (Fig. 1b) revealed focally increased (SUVmax: 5.4) within residual cervical mass and iliac lymph nodes, consistent with partial metabolic response and multiple hypermetabolic foci of FDG uptake within subcutaneous tissue in left lower lateral chest, hepatorenal area, right gluteal area, left upper anterior region of the thigh, left lower quadrant of abdominal wall and several muscles (left abdominal oblique muscle, right iliopsoas muscle) (Fig. 2). CT scan detected subcutaneous nodular lesions in the same areas. The excisional biopsy of subcutaneous metastasis revealed metastatic atypic squamous epithelial cells.
 within large cervical mass together with internal and external iliac lymph nodes (a). Posttreatment MIP of FDG-PET/CT data (b) revealed focally increased (SUVmax: 5.4) within residual cervical mass and iliac lymph nodes, consistent with partial metabolic response and multiple hypermetabolic foci of FDG uptake within several muscles and subcutaneous areas.")
Pretreatment MIP of FDG-PET/CT data showed increased heterogeneous FDG uptake (SUVmax: 15.3) within large cervical mass together with internal and external iliac lymph nodes (a). Posttreatment MIP of FDG-PET/CT data (b) revealed focally increased (SUVmax: 5.4) within residual cervical mass and iliac lymph nodes, consistent with partial metabolic response and multiple hypermetabolic foci of FDG uptake within several muscles and subcutaneous areas.
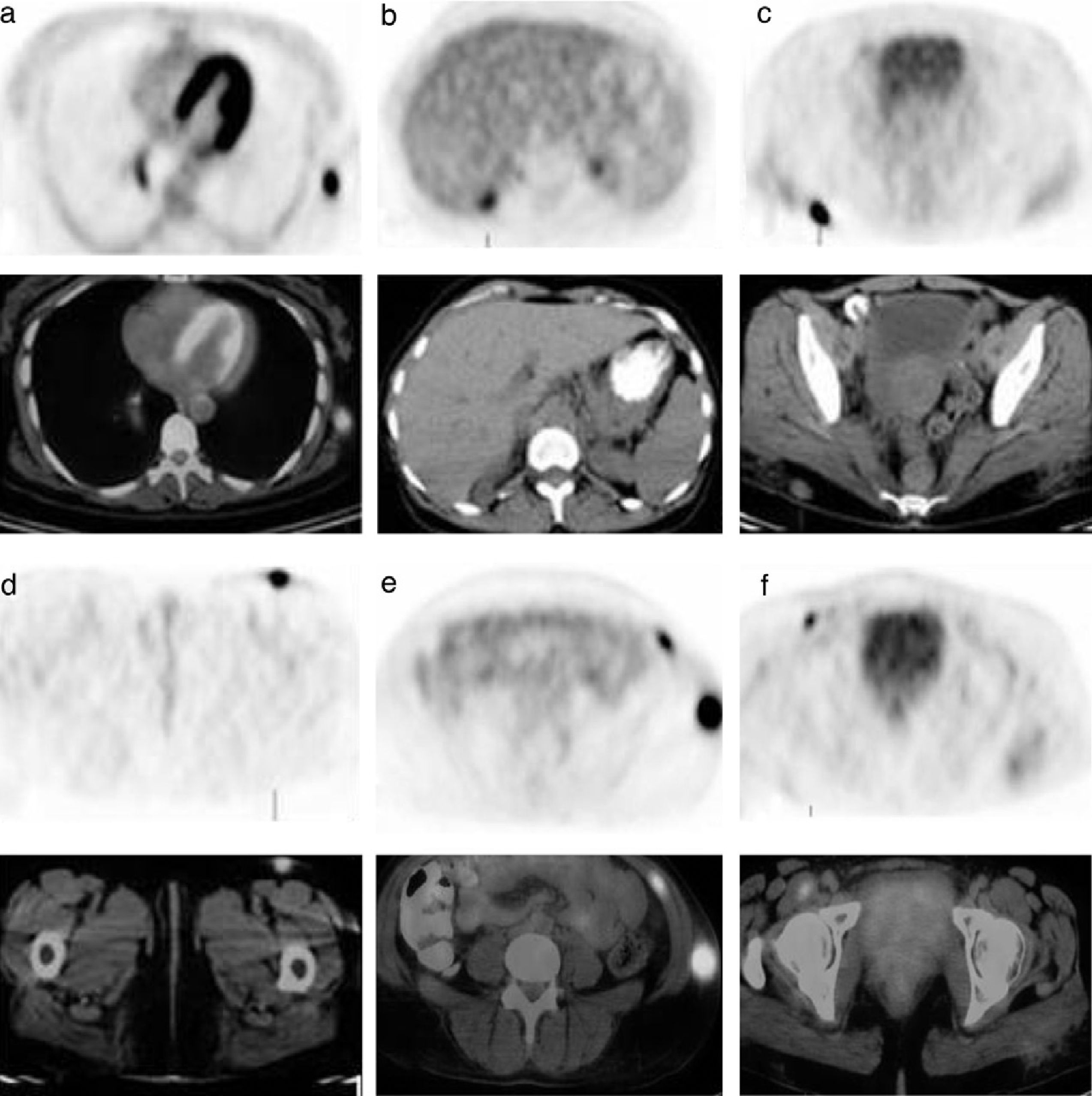
 subcutaneous tissue in left lower lateral chest (a), hepatorenal area (b), right gluteal area (c), left upper anterior region of the thigh (d), left lower quadrant of abdominal wall and the left abdominal oblique muscle (e), and right iliopsoas muscle (f).")
Posttreatment FDG-PET/CT revealed increased FDG uptake (SUVmax: 19.8) subcutaneous tissue in left lower lateral chest (a), hepatorenal area (b), right gluteal area (c), left upper anterior region of the thigh (d), left lower quadrant of abdominal wall and the left abdominal oblique muscle (e), and right iliopsoas muscle (f).
