



Morgagni's hernia is a rare type of congenital diaphragmatic hernia that constitutes less than 5% of congenital diaphragmatic defects. It is moderately associated with congenital anomalies, while it is rarely associated with Down's syndrome or trisomy 21. On the other hand, the incidence of anorectal malformations in patients with Down's syndrome is relatively frequent, with an incidence of from 0.36% to 2.7%. We present the case of a newborn baby with Down's syndrome and anorectal malformation without fistula, colostomised, which evolved with episodes of intestinal subocclusion. In the study of a second episode of constipation, with colonography through the colostomy, a Morgagni hernia was found and afterwards surgically resolved. The objective is to point out the rarity of the association between Down's syndrome, Morgagni hernia and anorectal malformation.
La hernia de Morgagni (HM) es un tipo de hernia diafragmática congénita (HDC) rara que constituye menos del 5% de los defectos diafragmáticos congénitos. Se asocia en moderada frecuencia con anomalías congénitas, siendo poco común su asociación con síndrome de Down (SD) o trisomía 21. Por otro lado, la incidencia de malformaciones anorectales (MAR) en pacientes con SD es relativamente frecuente, con una incidencia de 0,36% a 2.7%. Se presenta un caso de un recién nacido con SD y MAR sin fístula colostomizado, que evoluciona con cuadros de suboclusión intestinal. En estudio de segundo episodio de constipación con colografía por colostomía, se pesquisa HM la cual se resuelve quirúrgicamente. El objetivo es señalar la rareza de la asociación entre SD, HM y MAR.
Congenital diaphragmatic hernias (CDH) are defined as a protrusion of the abdominal viscera towards the thorax through a defect that is present at birth. It has an incidence of 1 every 3000 live births, and it is associated with pulmonary hypoplasia and pulmonary hypertension. The most frequent type is Bochdalek (posterolateral) in 90%–95% of cases. Morgagni's hernia (MH) (which is anterior retrosternal or peristernal) is a rare type of CDH that constitutes fewer than 5% of congenital diaphragmatic defects.1–8 On average chromosome abnormalities are detected in 10% of CDH cases,1 and the most frequent ones are trisomy 18 and tetrasomy 12p.2 CDH and trisomy 21 are rarely associated,6–8 although when this is the case MH predominates.1 On the other hand, anorectal malformations (ARM) are one of the most frequently seen congenital anomalies in paediatric surgery, with an incidence that is estimated to stand at from 1 in 2000 to 1 in 1500 live births.4 Anorectal malformations are common in patients with trisomy 21, with an incidence of from 0.36% to 2.7%.3
Clinical caseA newly born male, AEG, with postnatal diagnosis of Down's syndrome (DS), low flow ductus arteriosus and ARM without a fistula (Fig. 1), operated with the creation of a derivative colostomy in the descending colon and evolving acceptably, discharged four days after surgery.

Subsequent consultation in the Emergency Unit of Osorno Hospital Base with a history of few colostomy stools. Physical examination detected abdominal swelling. Simple abdominal X-ray showed no hydroaeric levels. The patient was hospitalised with the diagnosis of intestinal subocclusion – probable faecaloma proximal to the colostomy – and clysis with saline solution was prescribed through a proximal stoma, evolving with a satisfactory response and discharged with a high-fibre diet and oral lactulose.
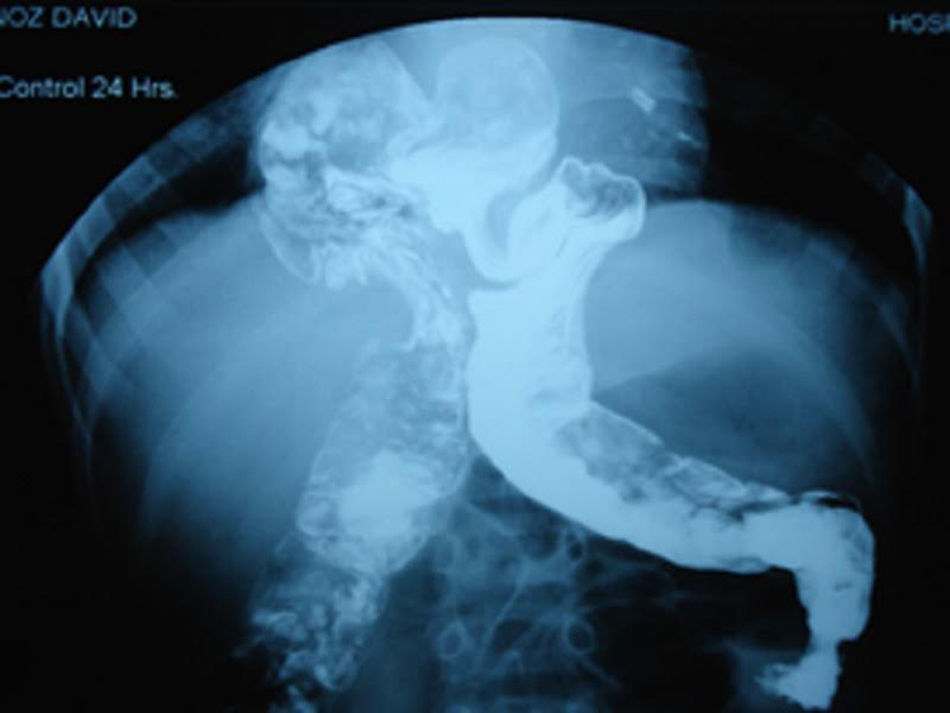
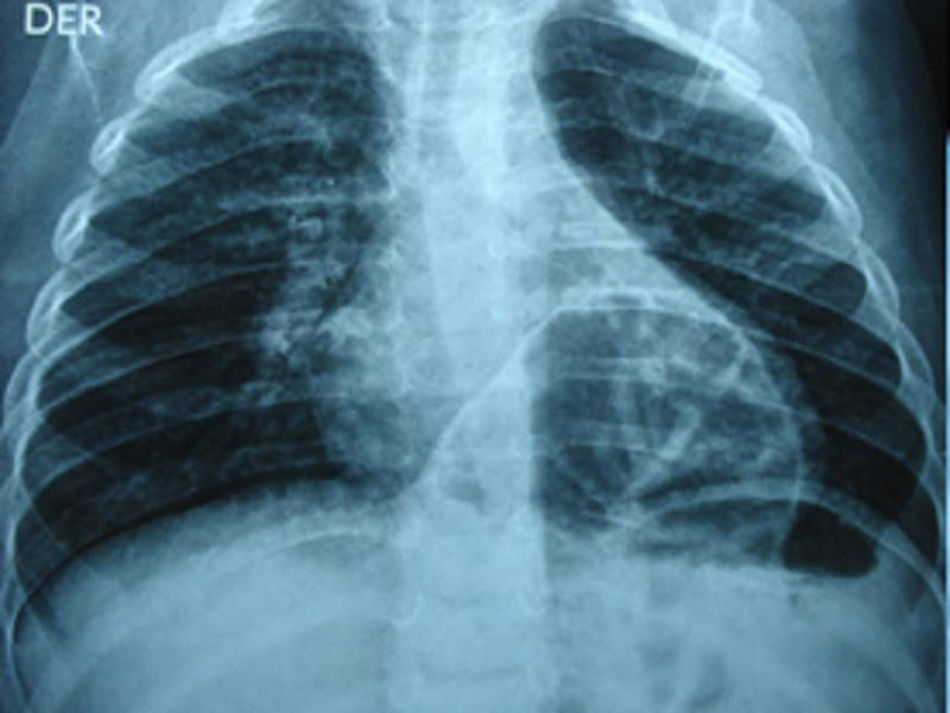
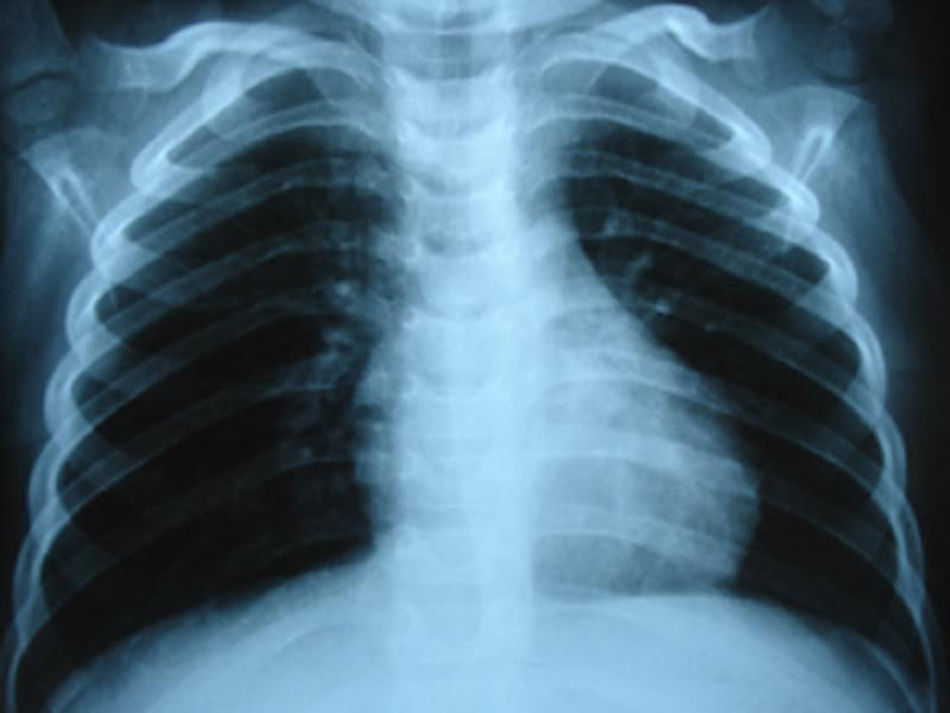
Approximately two month after discharge in a paediatric surgery check-up proximal stoma colonography was requested to evaluate the elimination of stools following a second episode of constipation, in which MH (Fig. 2) was detected. A simple thoracic-abdominal X-ray was taken to document the case (Fig. 3). The decision was taken to resolve the hernia by laparoscopic surgery, which was performed without incidents. A postoperative radiographic check showed no defects in the diaphragm (Fig. 4). The anorectal malformation was corrected subsequently using a posterior sagittal approach, and the absence of a fistula was confirmed.
Discussion


The association between DS, ARM and MH is currently unknown. On the one hand the aetiology of ARMs is unknown. It has been suggested that it may be due to a dominant autosomic hereditary pattern that affect chromosome 7q39. Approximately 50% of ARMs patients have associated anomalies, of which the most frequent are gastrointestinal ones followed by cardiovascular ones and tethered spinal cord syndrome.1 On the other hand, nor do congenital diaphragmatic defects have any known pathogenesis. Some theories attribute them to faults in the closure of the pleuroperitoneal folds between the 4th and 10th week of gestation, while others attribute them to genetic or environmental triggers which interrupt mesenchymal cell differentiation during the formation of the diaphragm.5
Although anorectal ARMs occur moderately frequently in patients with trisomy 21, CDH are less common. In a review of the literature no association was found between DS, ARM and MH, which may be due to a lack of any association between them or the fact that one has yet to be discovered. It is possible that future genetic research may discover a relationship between these three entities.
The pathologies of our patient were resolved surgically without any drawbacks, and more specifically Morgagni's hernia was resolved laparoscopicly with excellent results (Figs. 1–4).
Conflicts of interestThe authors have no conflicts of interest to declare.