













A conservative treatment for a patient with serious aesthetic problems related to the presence of anomalous teeth is hereby presented. Aside from the malocclusion, the patient had upper lateral incisors with microdontia, mild lower crowding and squared arch form. The treatment plan was conservative and for better results, multidisciplinary, involving orthodontics, periodontal treatment and minimally invasive restorations. Treatment time was 20 months. A positive result was observed after a 2-year follow-up.
Se presenta el caso de un paciente de 11 años con graves problemas estéticos relacionados con la presencia de dientes anómalos. Además de la maloclusión, se observaron incisivos laterales con microdoncia, apiñamiento leve inferior y forma cuadrada de arcos. El plan de tratamiento fue conservador y para obtener los mejores resultados, fue multidisciplinario: ortodoncia, tratamiento periodontal y restauraciones estéticas mínimamente invasivas. El tiempo de tratamiento fue de 20 meses, el resultado positivo se observó después de un periodo de dos años de seguimiento.
Microdontia is an anomaly in which teeth are smaller than normal. It presents problems which affect arch length and facial aesthetics. When the width of the upper lateral incisor (ULI) is less than, equal to or up to 0.7mm wider than the lower lateral incisor, the result would be an excess of lower dental material in relation to the upper.1 Tooth size is determined genetically and its diminishment is due to weakening of the enamel body during the differentiation period. Microdontia may occur due to both genetic and environmental factors and it is classified in localized or generalized being more common the first condition.2 Binder and Cohen, based on data provided by Moorrees and Moyers where the normal size of the teeth was determined, indicate that the upper lateral incisors is 12-14% wider than the lower lateral incisor.3 In a study conducted in Mexico by Gómez-Fernández et al., it was concluded that 42.5% of the studied models presented microdontia in the upper lateral incisors according to the criteria determined by Binder and Cohen which should be considered in orthodontic treatment planning.4 It has been suggested that the mesiodistal width of the lateral incisors is smaller in people with class III malocclusion,5 however, other studies have shown that there is no statistically significant difference between malocclusions and the presence of lateral incisors with microdontia.6
CASE REPORTA patient of 11 years and 4 months of age, mesofacial, who in his medical and dental interrogation referred no clinically relevant information, is presented (Figure 1).

Intraoral analysis. Microdontic lateral incisors, a 0.5mm deviation to the left of the lower dental midline in relation to the upper dental midline, molar and canine class I, mild lower crowding and arch form were observed (Figure 2).
 Front, B) Right side, C) Left side, D) Upper occlusal, E) Lower occlusal.")
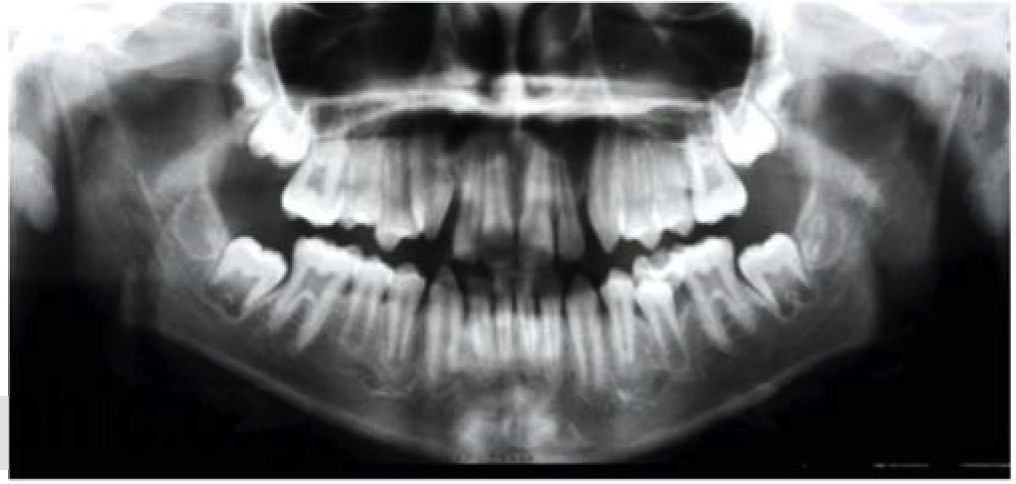
Radiographic analysis. A hyperdivergent skeletal class I was diagnosed (Figure 3). In the panoramic X-ray (Figure 4) the presence of the right deciduous second molar and inadequate root parallelism may be observed.


Goals of treatment. To improve the facial profile, correct mandibular crowding, achieve normal overbite and overjet, bilateral canine class I and matching dental midlines, as well as maintaining the bilateral molar class I, achieve correct intercuspation, canine guidance and a mutually protected occlusion.
Treatment. Treatment began with alignment and leveling of the arches. Space closure was reciprocal using a boot loop that was activated 1mm per month.
Stripping was performed for detailing and afterwards, retention. In the treatment progress analysis it was observed a facial change as well as an improvement in arch form (Figures 5 to 7).



In the treatment progress lateral headfilm a significant change occurred in the profile and at dental level. The latter was corroborated with the following cephalometric measurements: Upper incisor to SellaNasion, upper incisor to palatal plane, lower incisor to mandibular plane, interincisal angle, nasolabial angle and mentolabial angle. These values showed an upper incisor retroclination, lower incisor retroclination and a change in soft tissues (Figure 8).

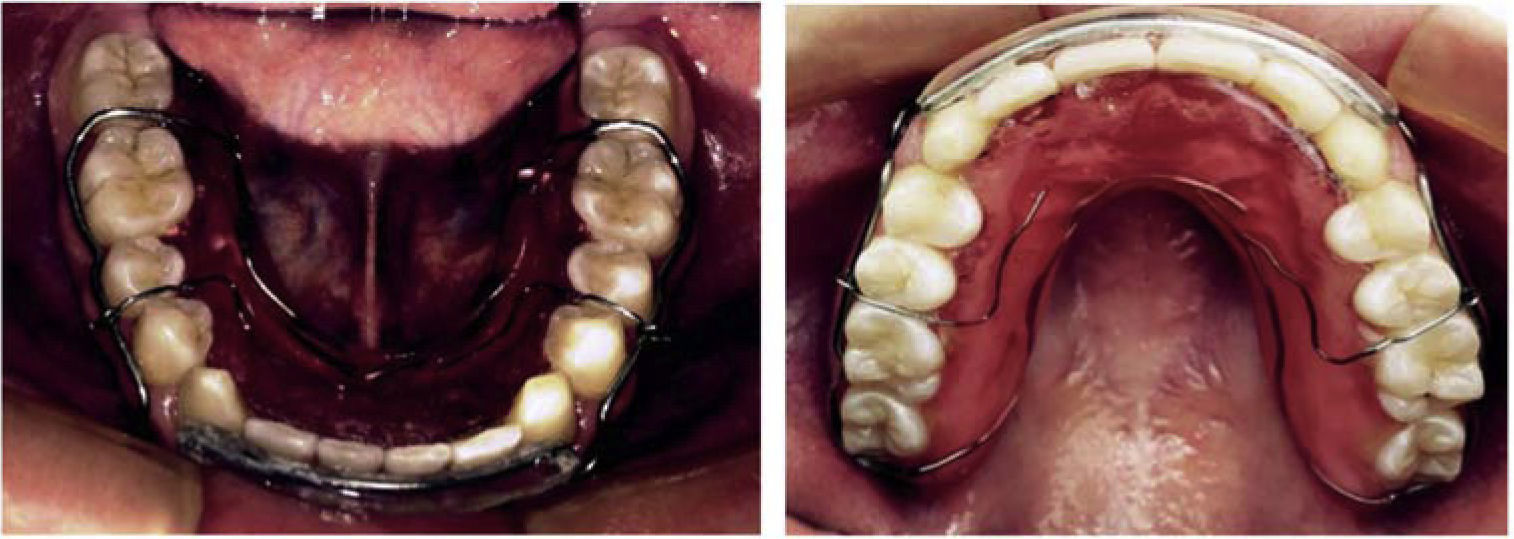
Results of treatment. In the final extraoral photographs it may be observed that the patient remained dolichofacial with a nice profile. Normal overbite and overjet were achieved as well as matching dental midlines, canine class I, molar class I and good intercuspation. Direct composite restorations were performed in the upper lateral incisors. In the occlusal view, a continuous, oval shape of the maxillary and mandibular arches may be observed upper and lower circumferential retainers were placed (Figures 9 to 11).



In the lateral headfilm it may be observed that the hyper-divergent skeletal class I was maintained with a slight dental change compared with the progress analysis. In the panoramic X-ray an acceptable root parallelism is noted as well as the eruption of the third molars (Figures 12 and 13).
DISCUSSION

Authors such as Kubodera et al. identified the mesiodistal size of teeth in Mexicans and found that in the upper arch the tooth which presents the greatest variability was the lateral incisor.7 The present case had affected lateral incisors. However, the results obtained were positive and coincide with what was stated by Gibilisco: that the most susceptible area for size anomalies such as microdontia is the upper anterior region, more specifically, the upper lateral incisors followed by upper third molars, but without ruling out its appearance in any other place in the arches, for example, premolars and lower incisors.8 Microdontia has a direct impact on tooth alignment thus preventing a good relationship with the antagonists and favoring a variety of anomalies that trigger malocclusions as well as alterations in the eruption path of the upper canines, causing retention and making it impossible to achieve canine and anterior guidance.9
CONCLUSIONDue to the psychosocial impact that upper lateral incisor microdontia causes by compromising aesthetics and given the fact that these patients attend orthodontic consultation seeking aesthetics; the decision on what treatment to perform will be a consensus among the orthodontist, the oral rehabilitation specialist and the patient, taking into consideration the cost/benefit according to the patient's needs and expectations and finishing the case with optimal or favorable dental results.
Second year Resident of the Masters Program in Orthodontics and Maxillofacial Orthopedics at the Centro de Estudios Superiores de Ortodoncia (CESO).
This article can be read in its full version in the following page: http://www.medigraphic.com/ortodoncia.