


Odontoma is the most commonly found odontogenic tumor (35- 76%). Odontoma is a benign tumor originating from an alteration of differentiated mesenchymal and epithelial odontogenic cells; it has the capacity of forming enamel, dentin and cement. They are classified into compound and complex, in a 2:1 relationship, the difference between both being dental tissue organization. Etiology is still unknown but relation to infections, hereditary anomalies, odontoblastic hyperactivity and trauma has been explored. Since these tumors are asymptomatic, 75% of all cases are diagnosed before the second decade of life, due to a delay in eruption of permanent teeth. Treatment of choice for these tumors is enucleation, attempting to preserve the tooth; relapse is very uncommon.
Los odontomas corresponden a los tumores odontogénicos más comunes (35-76%). Es un tumor benigno originado a partir de una alteración de células odontogénicas epiteliales y mesenquimatosas diferenciadas con capacidad de formar esmalte, dentina y cemento. Se clasifican en compuestos y complejos en una relación de 2:1, siendo la diferencia entre ambos la organización del tejido dentario. La etiología es desconocida pero se ha explorado la ocasión a infecciones, anomalías hereditarias, hiperactividad odontoblástica y traumatismos. El 75% de los casos se diagnostican antes de la segunda década de vida debido a un retraso en la erupción dental permanente, ya que son asintomáticos. El tratamiento es la enucleación tratando de conservar el diente permanente, siendo las recidivas poco frecuentes.
Presently, the World Health Organization (WHO) classifies odontoma within the category of odontogenic tumors (OT) composed by epithelium and odontogenic ectomesenchyme with or without formation of mineralized dental tissues.1 The term odontoma was coined by Pierre Paul Broca in 1867, with it he described any tumor created by the excessive transitory or full growth of dental tissues.2 Later on, in 1946 Thoma KM and Goldman HM formulated a presently disused odontoma classification.3 Odontoma are classified taking into account organization and degree of alteration of odontogenic cells, there are two classifications: compound (CpO) and complex (CO).1,4 Compound odontogenic tumor (CpO) exhibits morphological and histological differentiation, while complex odontogenic tumor (CO) only presents histological differentiation.5 In CpO multiple amorphous dental structures are formed (denticles), while in CO a solid mass of dental soft and hard tissues is formed, these tissues are haphazardly arranged and do not resemble the morphology of a tooth.4,6,7
EtiologyEtiology of theses tumors is unknown, nevertheless, some authors have described the possible relationship with trauma in primary dentition, Malassez paradental remains, inflammation processes, odontoblastic hyperactivity and hereditary anomalies (Gardner and Herman syndrome).8–12
Epidemiological aspectsWorldwide reported frequency of odontogenic tumors varies to a wide range (1-32%).13 Most of these series report odontoma as the most prevalent lesion of odontogenic tumors in an interval of 35 to 76%.13–19 Buchner et al,13 studied in 2006 a sample of 1,088 odontogenic tumors, of which 76% corresponded to odontoma. Previous to that, in 1997, Mosqueda Taylor et al examined 349 odontogenic tumors, out of which 35% were odontoma.14 This difference in prevalence among various studies can be due to differences in terminology and classification; possible association to ethnic or genetic aspects is equally suggested.8
Odontoma frequency according to gender has been variously reported in several studies, to this date no consensus has been reached, this can be due to the subtle prevalence differences reported between both genders.8
Some authors report higher prevalence in females17,20–22 while others have reported higher prevalence in males.13,23–25 Hidalgo O et al conducted in 2008 a meta-analysis on epidemiological characteristics of odontoma. They studied 3,065 cases and mention in their results that 49.4% were female patients and 50.6% males.8 Concluding thus there was no significant difference according to gender; this concurs with different studies.14,26–28 According to age diagnosis, odontoma can be identified at wide age ranges, nevertheless a high prevalence peak is reported in the second decade of life.21,25,27–30
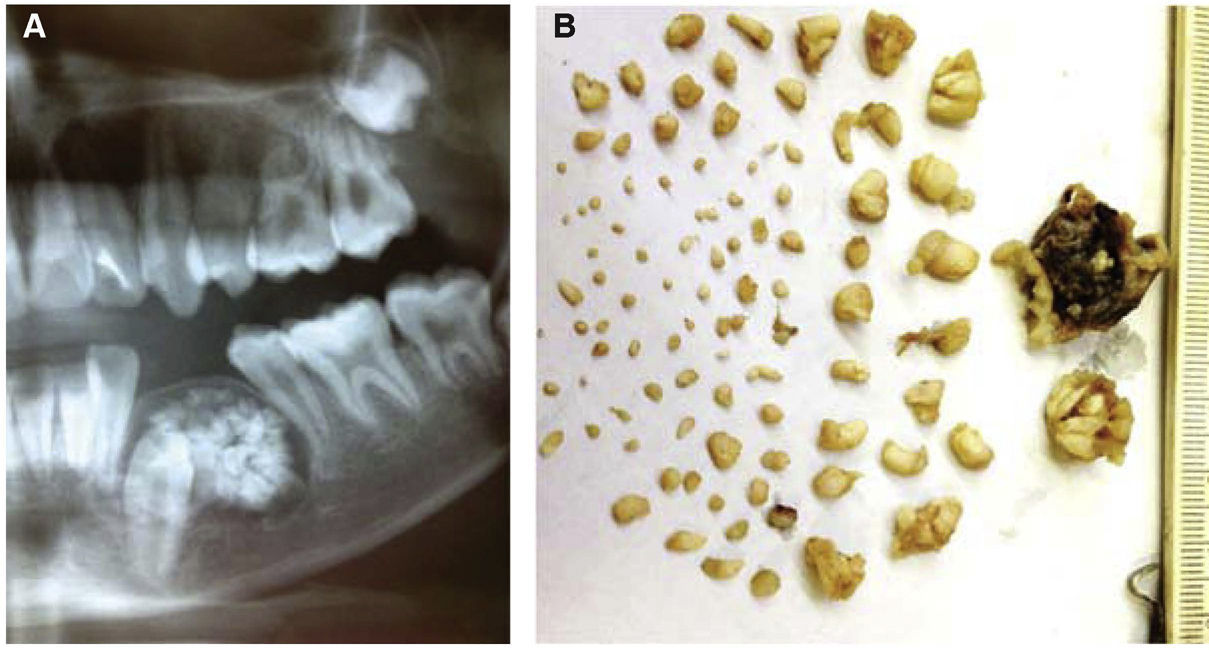
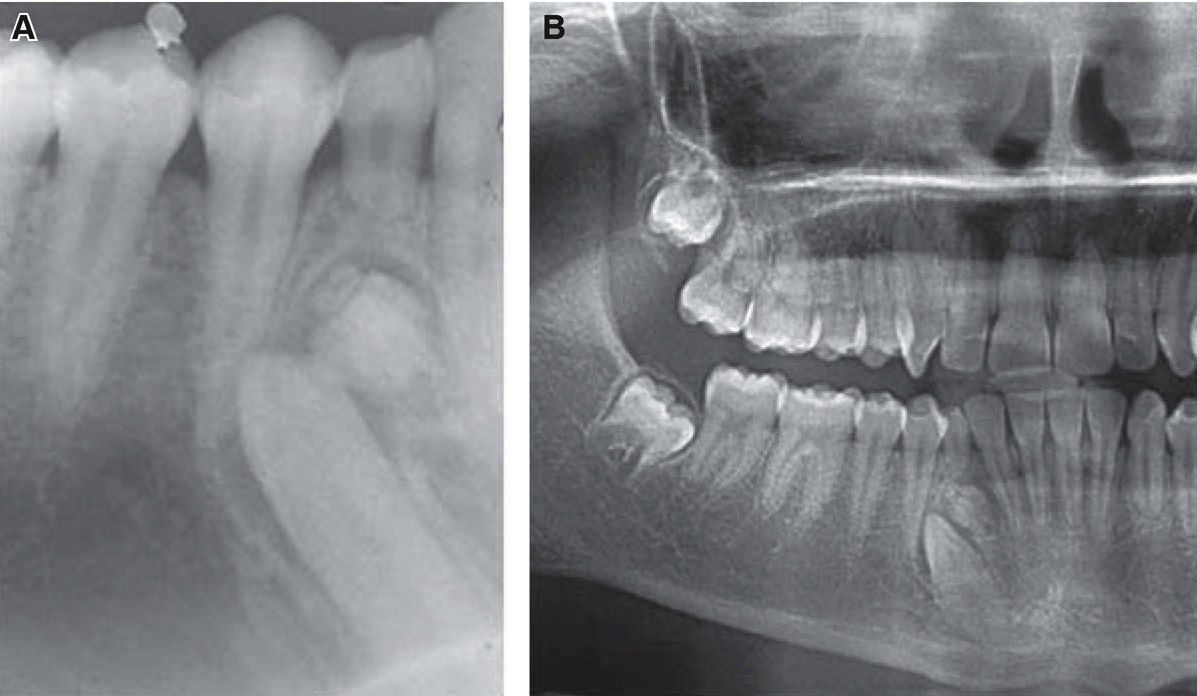
Clinical characteristicsIn scientific literature, three clinical presentations of odontoma have been recognized: intra-osseous, extra-osseous and erupted. Intra-osseous odontoma are the most frequent.31 The most frequently reported location is the incisor-canine area of the upper jaw (67%) followed by lower-anterior and lower-posterior areas of the lower jaw (33%).14,26–28,32 CpO clearly appear more frequently than complex odontoma in the anterior section of the upper jaw over the crown of one of more non-erupted teeth, or between roots of erupted teeth (61%) (Figure 1), whereas complex odontoma most frequently appears in the posterior section of the mandible (59%) (Figure 2).8,33,34
 Compound odontoma in lower premolars. B) Macroscopic image of compound odontoma constituted by a capsule of fibrous tissue and multiple denticles.")
 Periapical projection of complex odontoma. B) Complex odontoma in the area of lower premolars (orthopantomography).")
Some other more uncommon isolated cases have been reported in the maxillary sinus, nasal cavity and floor of the orbit.8
Odontoma are benign, not very aggressive tumors which usually do not elicit symptoms; over half the cases are discovered as radiographic findings (57%).8 Different studies report an association (16-61%) with impacted teeth.35,36
Most odontoma are intra-osseous, nevertheless there are reported cases of odontoma which have erupted into the oral cavity.7 Crespo et al, reported a case of chronic maxillary sinusitis secondary to drain obstruction caused by an odontoma;37 Suenaga et al presented the case of a complex odontoma located in the right nasal fossa which caused nasal obstruction and bleeding.18
Amado-Cuesta et al conducted a literature review in which they reviewed 38 cases of compound odontoma. In that review denticle numbers varied from 4 to 28. In a case reported by Sharma et al a compound odontoma with 37 denticles was extracted; denticles exhibited concrescence, fusion and laceration.11
Radiographic characteristicsCompound odontoma (Figure 1) can be observed as radio-opaque masses with irregular margins adopting a tooth-like configuration; they present radiolucid peripheral borders, whilst complex odontoma exhibit unique radio-opacity.4 According to the degree of odontoma calcification, three stages of development can be identified: in the first stage the lesion appears radio-lucid (due to lack of calcification of dental tissues), the intermediate stage is characterized by partial calcification, and in the final stage the odontoma appears radio-opaque and surrounded by a radio-lucid halo (Figure 2).21
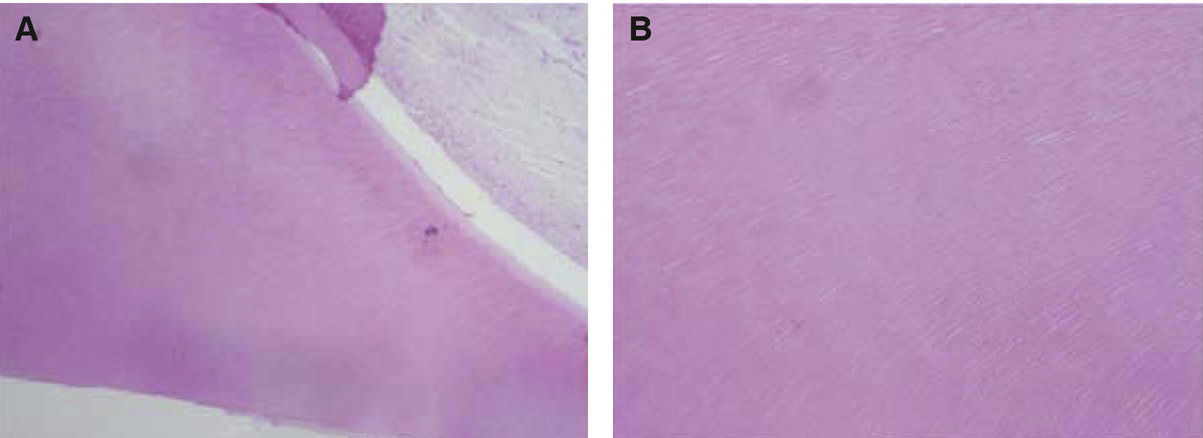
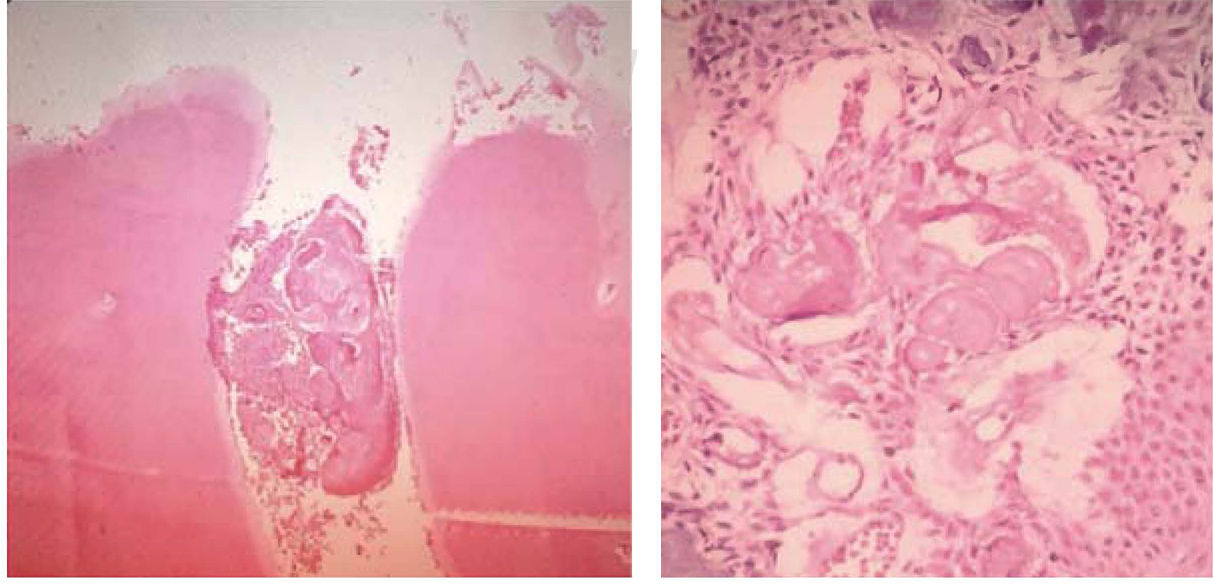
Histological characteristicsFrom a histological point of view, compound odontoma (Figure 3) are characterized by presence of dental tissue, demineralized enamel, dentin, cement and pulp, arranged in an organized manner of dental structures and partially surrounded by a connective tissue capsule. Conversely, complex odontoma (Figure 4) exhibit a disorganized mass of hard dental tissue;6 odontogenic epithelium strands can be found in the periphery,20 and sometimes, presence of phantom cells, cementicles and ameloblastic epithelium can be detected.4 These tumors can be associated to other odontogenic tumors such as ameloblastoma, ameloblastic fibro-odontoma, odonto-ameloblastoma, calcifying epithelial odontogenic tumor, adenomatoid odontogenic tumor and dentigerous cyst, therefore histopathological study is recommended in all cases.15 Soluk Tekkesin M et al, conducted a study in 2012 where they assessed histological characteristics of 160 odontoma. Within their results they mention that ameloblastic epithelium was more frequently observed in complex odontoma, whereas mesenchimal odontogenic tissue was mainly observed in compound odontoma; they equally reported that phantom cells were found in up to 20% of examined samples.4
 Histopathology of compound odontoma characterized by the presence of dental tissues arranged in an organized manner, dentin and pulp. B) Dentin (400x).")

When complex odontoma is in its intermediate phase it resembles other lesions such as fibro-osseous lesions, calcifying cystic odontogenic tumors, fibrous dysplasia and chronic osteomyelitis.20 Odontoma is an odontogenic tumor most frequently associated to calcifying cystic odontogenic tumors, it can be found in up to 24% of all cases.22 Likewise, differential diagnosis must be performed with ameloblastic fibroma, ameloblastic fibro-odontoma, and odontoameloblastoma. If they exhibit a radiographic image similar to that of odontoma and are located in the intra-radicular area, a differential diagnosis must be established with lesions such as focal residual osteitis, cementoma, calcifying epithelial odontogenic tumor, adenomatoid odontogenic tumor, supernumerary tooth, cementing fibroma or benign osteoblastoma. When it is found surrounding a crown, it should be differentiated from adenomatoid odontogenic tumors, calcifying epithelial odontogenic tumor, ameloblastic fibrodentinoma or an odonto-ameloblastoma. In the maxillary sinus it could be confused with sinusitis, periapical infection with antral polyps, antral mycosis, displaced root or tooth, foreign body, peripheral osteoma, mesenchymal benign neoplasia, inverted papilloma or antral carcinoma or sarcoma.26
PrognosisSome of the complications that might arise are the following: impacted teeth, nasal obstruction, otodental syndrome.15 Odontoma and supernumerary teeth are the main cause of permanent incisors’ impaction, due to the existing direct obstruction to their eruption.26 In exceptional cases, spontaneous eruption of odontoma into the mouth occurs, accompanied by possibility of eliciting pain, inflammation of adjacent soft tissues or infection associated to the suppuration. Twenty reports of erupted odontoma were found in literature review, out of which eleven were complex odontoma, and nine were compound odontoma.27 Erupted odontoma can exhibit caries and entail abscess formation.11
TreatmentTreatment of choice consists in conservative surgical enucleation by means of the removal of the conjunctive tissue capsule that surrounds it, suitably preparing the sample for the histo-pathological study which will support an accurate diagnosis.15,20 Sometimes, orthodontic treatment will be required to reposition the arch of the retained tooth.10 Prognosis is generally favorable, with scarce relapse index; relapse rate increases when enucleation is conducted during the first calcification stage.21,26
Final considerationLiterature review revealed a wide panorama of descriptive aspects for odontoma. Odontoma is one of the most frequently found odontogenic tumors; it is detected through routine radiographic examination, and mainly found in patients in their second decade of life.8 It is therefore advisable to conduct a timely and accurate diagnosis in order to avoid subsequent complications.11 It is further recommended to perform histopathological analyses so as to discard the possibility of association to some other type of odontogenic tumor.22
Student of Pediatric Stomatology Master's Degree, School of Dentistry, Chihuahua Autonomous University, Mexico.