








COVID 19 & vaccines: Development and practice
More infoMass vaccination poses a challenge for health authorities due to the high volume of people who need to be vaccinated in a short period of time. Manual processes in vaccination centres to record and control vaccinations where the data is entered on paper result in delays in the timely input of information rendering the vaccination process inefficient. The proposed prototype, as a strategy for mass COVID-19 vaccination, to generate appointments, record, and control entry to vaccination centres, uses mobile technology, QR codes, and cloud computing to automate these data-driven processes. Technology-based processes help people by giving them the flexibility to choose the most convenient vaccination centre and provide health authorities with data-driven tools for management, control, and real-time decision-making.
Las vacunaciones masivas son un desafío al que se enfrentan las autoridades sanitarias, debido al alto volumen de ciudadanos que deben ser vacunados en un corto tiempo. Los procesos manuales en los centros de vacunación para el registro y control de las vacunas donde se emplea el papel como elemento repositorio de los datos generan retrasos en la entrega oportuna de la información procesada y el proceso de vacunación se vuelve ineficiente. El prototipo propuesto, como estrategia de vacunación masiva contra el COVID-19 para la generación de citas, registro y control de ingreso a los centros de vacunación utiliza las tecnologías móviles, código QR y Cloud Computing, para la automatización de estos procesos basados en datos. Los procesos apoyados en tecnología ayudan al ciudadano por la flexibilidad de elegir el centro de vacunación más conveniente a su realidad y permiten a las autoridades sanitarias disponer de herramientas basados en datos para la gestión, control y la toma decisiones en tiempo real.
Mass vaccinations against COVID-19, given the sheer number of citizens to be vaccinated, are known to be complex1 and challenging,2,3 require efficient interdisciplinary management across different stakeholders, such as the supply chain, logistics for vaccine transport and storage,4,5 vaccination centre management, dose distribution, scheduling and allocation of personnel for perimeter security, verification, monitoring, and vaccination, among others. A study of health services in Vatican City6 concludes that the successful implementation of a mass vaccination campaign of residents, workers, retirees, and their families is of paramount importance to control the spread of infection; nevertheless, there is no single approach to vaccination7,8 and the delay in new vaccination strategies among countries is by no means new; for example, countries such as Israel, the United Kingdom, and the United States made rapid strides in COVID-19 vaccination programmes in contrast to other countries in the southern hemisphere that were just getting started.9 Technology support plays a major role in developing solutions in many fields of knowledge, and mass vaccinations against COVID-19 are no exception.10
New variants of the virus are expected despite the fact that mass vaccinations against COVID-19 have been initiated; one of the strategies for vaccination would therefore be to increase the number of doses.11 This increase in doses entails maintaining mass vaccination schedules. However, when registration and entry control activities at vaccination centres are performed manually, they have a negative impact on the vaccination process because the complexity of the process12 or the pressure of care increases the likelihood of human error and this results in mistakes, risks, and high costs associated with routine tasks,13 or they are too slow.14
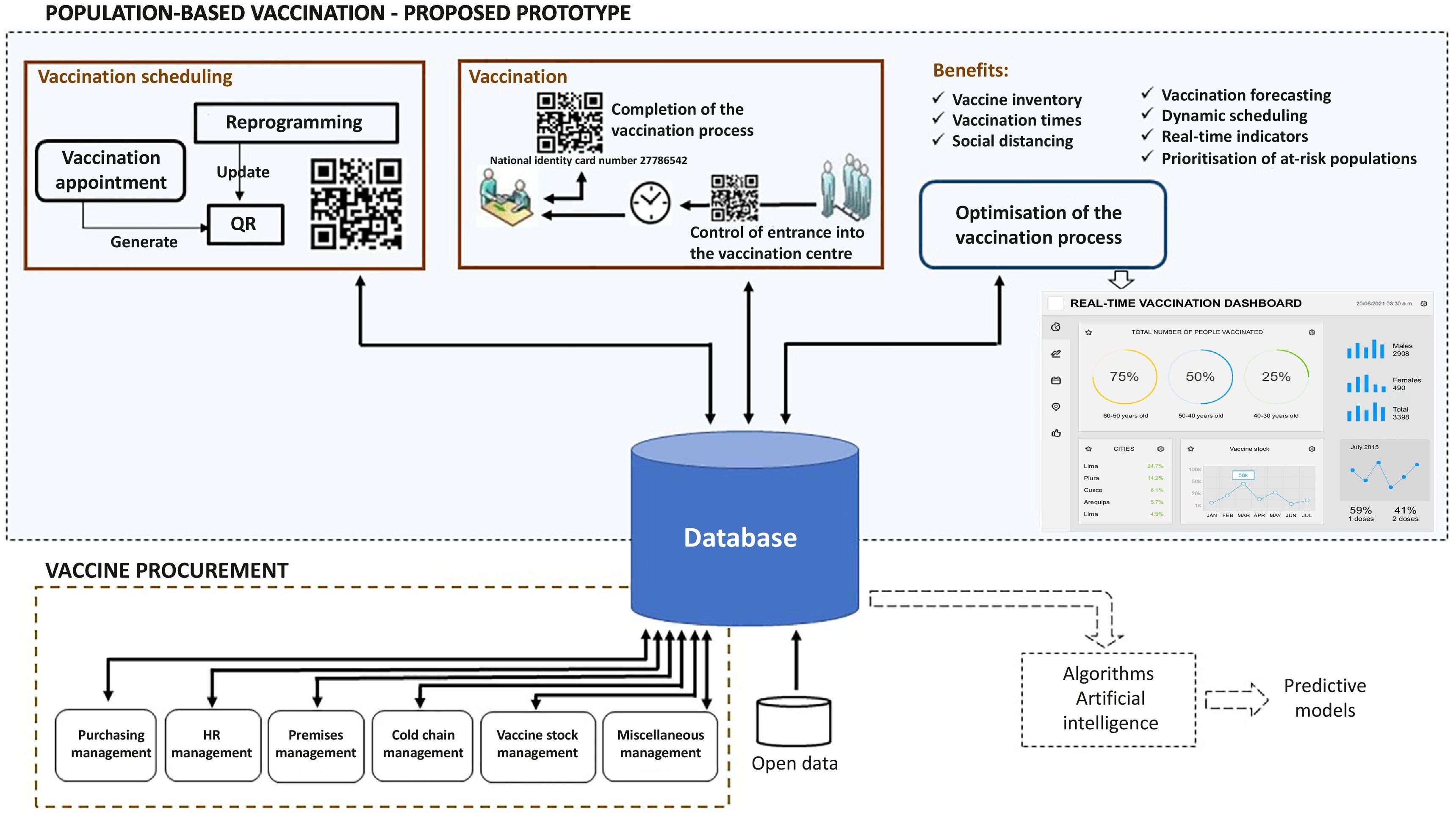
Automation through the use of technology as an advantage to save human labour and put it to a more productive use, typically decreases the number of errors, repetitive activities, and processing times, among others.13,15 Automating processes and digitising data for real-time management and control in order to optimise the resources involved makes it possible to outline predictive schemes. The integration, homogenisation, and synchronisation of digital solutions through a framework and policies16 enables the impact of the vaccination process to be monitored, thereby accelerating deployment and optimising supply chain strategy by managing and analysing data9 in a single centralised database for the different processes to update or consult and, most importantly, share the same data. Eliminating the information silos that lead to inefficiency in organisations as a result of the difficulty of sharing data with all those who need it,14 which, in our particular case, would be to eliminate the information silos of a mass vaccination programme, as shown in Fig. 1. For example, in the case of Chile, for the COVID-1917 vaccination, they had the infrastructure and health personnel, among other elements, but they stressed that their success was achieved thanks to their electronic vaccine registry, which was pivotal for deployment, monitoring, and follow-up, enabling them to sustain the strategy, increase efficiency, minimise errors owing to the existence of multiple vaccination centres, different vaccination schedules for different groups of vaccines that required 2 doses, and the presence of several different vaccines at the same time in the same place. In other words, information and communication technologies (ICTs) become strategic support tools for health personnel: doctors and nurses, among other specialties that would make it easier for them to conduct their activities according to the role they play. For example, the University of Miami, USA, used ICTs to automate key COVID-19 vaccination processes, and managed to administer 19 000 vaccines in the first 37 days, which accounted for 100% of vaccine allocation without a single dose being wasted.18 Another successful experience of using ICTs is that of Inova Health System, USA, which vaccinated more than 12 000 people over the course of 3 weeks since the first COVID-19 vaccine was approved, noting that the next steps in their vaccination programmes involve leveraging technologies to optimise patient flow.19

In a pandemic, time plays a crucial role to get ahead of the spread. Agile R&D approaches will be required that can adapt as quickly as epidemics evolve and against new infectious disease threats, harnessing the potential of immunisation data to inform programme interventions.20 In that regard, the generation and availability of real-time data in the process of mass immunisation will enhance the efficiency of control, surveillance, and monitoring, all in real time. The benefits of having digital data make it possible to take advantage of them by means of various techniques such as Big Data, Machine Learning, and Deep Learning, among others. However, asynchronous digital data, i.e., with delays of hours, days, weeks, or months, involve considerable disadvantages. Sophisticated artificial intelligence predictive models could be rendered useless because the data is not available in real time. Public policy or health policy decisions must be made as quickly as possible in order to halt or forecast the spread of COVID-19; consequently, access to real-time data is a necessity.
In this research, we propose a prototype for vaccination centres to generate appointments and to register and control entrance based on a mobile digital platform that allows for decentralisation, balancing of vaccination centres, and real-time availability of the vaccinated registry. Decentralisation will provide citizens with flexibility in selecting the vaccination centre closest to them, which will not necessarily be the one closest to their home. The prototype has 3 purposes: first, to provide citizens with a tool that gives them flexibility in the processes involved in vaccination registration and control; second, to provide executive staff responsible for public health with a decision-making dashboard based on public or health policy data, and third, to provide a single, centralised database that is updated in real time for use in different detection or predictive models that researchers can propose and combine with other databases or information sources.
The problem of vaccination centres in contextThe effective deployment of vaccines and vaccination [strategies] will depend on the effective management of planned activities and processes at the national, regional, district, and local levels. This planning is complex, given that it must include budget management, vaccine management, demand for vaccine uptake and adoption, vaccine safety surveillance, and monitoring and control.21,22 In addition, vaccination sites should be established based on a target population and geographic area, which determines equitable distribution. This would estimate projections of the number of people they can support, the number of staffs that need to be involved, and the number of vaccines that must be allocated, among other aspects. In other words, vaccination centres must have estimates of the maximum demand they will serve based on the proportion of the population by geographic area in order to achieve equitable distribution throughout the country. In this context, the success of COVID-19 vaccination centres is based23 on safe and effective demand and capacity planning. The balance between the number of people to be vaccinated and the capacity of vaccination centres will prevent long queues from forming caused by excessive demand or wasting installed capacity caused by under-demand.
Mass vaccinations against COVID-19, in Peru, are evidence of a series of situations that arise before, during, and after the vaccination process. Such occurrences have a direct impact on distribution efficiency, human resource utilisation, management, data generation, and control of vaccines. Table 1 depicts the challenges of mass vaccination.
The challenges of mass vaccination in the Peruvian context.
| Antes | During | After |
|---|---|---|
| ● For each citizen, the distribution of vaccination centres, dates, and times is rigid and static. They are dictated by the health sector47,48 | ● The citizen presents him/ herself at any vaccination centre. They do not comply with the vaccination centre, date, and time assigned, resulting in an imbalance in the capacity of the vaccination centres. One vaccination centre may be overcrowded while another is not.49 | ● Delays in the availability of information from the registry of vaccinated people. It is subject to the time it takes to digitise the data recorded on paper into the electronic databases of vaccinated individuals.27 |
| ● The control and registration at the vaccination centres is done manually and on hard copy paper (including the vaccination informed consent form). Physical contact is unavoidable between the control staff validating the appointments and the citizen through paper and/ or pencils.25 | ● The integrity and authenticity of paper vaccination certificates given to the vaccinated person is not guaranteed. The likelihood of falsification and/ or tampering of the information they contain is proportional to the time it takes to digitise the information.50,51 | |
| ● There is no centralised, real-time control among vaccination centres. It could turn out that the same citizen is vaccinated at more than two vaccination centres.27,49 | ● The data generated during the vaccination process is not used for analysis, prediction, or in combination with other databases. |
At the moment, vaccination centres have 3 fronts on which to improve: first, to optimise human resources for the tasks of control, registration, and data digitalisation recorded on paper;24 second, to minimise the probability of infection of ordinary citizens who attend vaccination centres that is caused by manual controls and records,25 by the crowds resulting from long queues,23,26 or by the use of public transportation (the high probability of infection would represent a setback in the fight against COVID-19), and third, official figures on the vaccination process are not available in real time,27 and can take days to be published. Citizens lack timely information that would enable them to select the vaccination centre with the fewest people and close to where they live in real time.
Proposed prototypeA country's mass vaccination plan can be viewed as 2 major activities that are not necessarily sequential: first, vaccine procurement and second, vaccination of the population at the vaccination centres. Accordingly, logistics, distribution, and storage systems at different levels within the country must be systematically and simultaneously organised and prepared3 by a variety of professionals who have a specific role or task to perform. In the case of vaccination centres, safe and effective demand and capacity planning23 is essential; i.e., the vaccination centre's demand must conform to the planned number of citizens to avoid overcrowding and the vaccination centre's capacity must ensure that both the facility's infrastructure and health personnel suffice to meet the anticipated demand. Within the healthcare personnel involved in vaccination centres, nurses have a key function, because of their characteristic role in cold chain care, handling, administration, education, and surveillance of events and reactions,24,29,30 and among other functions, recording the vaccination process. According to Eggertson,31 physicians are concerned about the absence of a national immunisation registry because neither health professionals nor patients can track individuals as they move from one jurisdiction to another. Ideally, both physicians and patients would be able to access records through an end-to-end electronic database, allowing them to determine which vaccines have been missed, which ones require boosters, and what new vaccines are available. The integration of ICTs into mass vaccination processes is both necessary and obligatory. Furthermore, Uwabor et al.32 highlight the value of digital access to immunisation records for clinicians and the importance of centralisation and the transferability of the data contained in digital repositories to support patient education and the planning and evaluation of public health programmes.
In this context, the proposed prototype as a mass vaccination strategy against COVID-19 for appointment generation, recording, and control of entrance at vaccination centres draws on experiences from research,17,23,33 recommendations from the World Health Organisation (WHO)30 and EsSalud.24 In that sense, the proposed prototype incorporates 3 technologies: mobile telephone, QR code, and Cloud Computing, to achieve the objectives of this study and ensure that vaccine doses are rapidly distributed to priority populations, together with a renewed approach to the fight against COVID-19.34
Mobile systems are being increasingly integrated into the production chain and Cloud Computing, or commonly known as the cloud, is playing an increasingly important role in the immediate future of overall process management.35,36 Mobile telephony, by means of terminal equipment such as smartphones, tablets, or laptops, is a technology that citizens are using on a daily basis, with 89.3% of the Peruvian population over the age of 6 using them,37 which will serve as a user interface terminal. Other technologies, such as QR codes and Cloud Computing, have advantages when they are combined with mobile technology, because the use of smartphones grew from 10% in 2014 to 36% in 2018; high-speed mobile Internet went from 48% penetration in 2014 to 61% in 2018, and today, many smartphones come with a QR code scanner, so there are more people with the ability to scan a code while out and about.38 The QR code is nothing more than a graphic dot matrix that stores information and its strength lies in the fact that information can be obtained through the mobile phone camera without physical contact. In addition, cloud technology offers services through the Internet, such as storing and accessing data; its strength lies in having the stored data available in real time from any device connected to the Internet.
It had been noted that vaccination centres used manual processes with data being recorded on paper and then entered into a digital database. In this context, the prototype considers these data for the transition to the automated vaccination process. The data will be available in real time through our proposed prototype via an Internet-hosted database, Cloud Computing, which we have named «Registro Vacunación online QR» [Online QR Vaccination Registry]. This database will contain the historical information of the dataset of the current manual process: «healthcare establishment», «vaccines», «vaccination centres », «vaccination scheduline »,39 and the future data generated by the new, automated vaccination process that corresponds to our solution prototype.
Components of the prototypeFig. 1 illustrates the proposed prototype within a complex mass vaccination system. The degree of interaction between the user, the software installed on the mobile terminal, and the database takes place in real time in the prototype. The interaction between the citizen, the control personnel, and the healthcare personnel, with the software installed on the mobile devices, depending on the role they play, will make it possible to write, read, or update the database hosted in the cloud, Cloud Computing, in real time. The strength of the prototype lies in having a digital and centralised database that is constantly updated in real time by the processes of registering vaccinated people at the vaccination centres, as well as other processes that are not part of the prototype, such as the vaccine procurement and distribution, as well as the maximum scaling of the vaccination centre depending on the space capacity of the premises for the capacity of the public, medical equipment, vaccine stock, cold chains, the staff involved, the non-medical staff necessary for the vaccination process, among others. Table 2 describes the modules that comprise the prototype from the perspective of time; that is to say, the role they play before, during, and after vaccination.
Prototype for mass vaccinations, architecture modules based on the Peruvian context.
| Before | During | After |
|---|---|---|
| Vaccination Scheduling ModuleThe application to be installed on the citizen's mobile phone will have the following functions:- Selection of the vaccination centre according to the specific needs of each citizen. | Vaccination ModuleThe application that will be installed by the healthcare staff at the vaccination centres on their mobile devices that play the role of security, citizen control, and registration of the vaccine administered, will interact with the QR code generated by the citizen, and will have the following functions:- Control of verified entrance into the vaccination centre, informed consent, selection, and registration in the centralised database. | Vaccination Process Optimisation ModuleThe application to be installed by the executive healthcare personnel on their mobile devices, as the person in charge of the vaccination programme, will have the following functions:- Provision of real-time information on the movement of doses administered at vaccination centres, saturated vaccination centres, and empty vaccination centres. |
| - Appointment re-scheduling | - Record of the vaccine administered; it will record the vaccine batch number, type of vaccine administered, and number of doses in the centralised database. The address of the vaccination centre, date, and time will be added automatically. | |
| - QR generation | ||
| - Provision of information in real time regarding the amount of vaccine by vaccination centres, among others that can be personalised throught the programming code of the application server. |
Vaccination Scheduling Module: The aim of this module is to provide citizens with a tool on their mobile device that offers them flexibility in the registration process, the selection of the vaccination centre, and access to their vaccination certificate. All in real time. Fig. 2 is a graphic representation of entrance into the system and QR code generation that is created as a result of the citizen having chosen the vaccination centre, having real-time information as to the amount of vaccines available per vaccination centre. Bearing in mind the sensitive and high-security nature of the data contained in the centralised database, access to the system will take place via security protocols, such as the 2-factor authentication and cloud solutions said companies provide, such as identity access management (IAM), encryption of data in transit because of Internet communications, and encryption of idle data to ensure data availability and reliability. The centralised digital database, in addition to allowing the citizen flexibility in the selection of the vaccination centre, would also show additional relevant information for managers through the «observations» window, such as: the number of nurses in the vaccination centre, the capacity available, the average rate of vaccination, waiting time between vaccinations, type of vaccine, among others, thanks to the data being centralised and constantly updated in real time (Fig. 1); these data are selected and sent to the user interfaces by means of the programming codes in a way that is transparent for the user.

Vaccination Module: Its objectives are: first, to provide the security and support staff at the vaccination centres with a tool to control the entrance of citizens to be vaccinated; second, to provide healthcare staff with a tool to confirm that the vaccine has been administered to the citizen. In both cases, the use of paper will be eliminated and digital data will be generated, updated, and stored in the cloud.
Vaccination Process Optimisation Module: This pursues 2 main objectives: first, to provide the executive staff in charge with a real-time control and command dashboard for decision making based on data that will allow them to direct public or healthcare policies properly; second, to provide a database updated in real time that can be used for applications that different researchers may propose as predictive models or detectors, in combination with other databases.
Results of the prototypeAs previously mentioned, the mobile platform will provide for decentralisation, balancing of vaccination centres, and real-time availability of the vaccinated register. This information is important and necessary because, according to Zachreson et al.,40 vaccination cannot provide herd immunity without massive population coverage, raising the question of the minimum number of vaccinated people to achieve this goal. In Peru, herd immunity will be achieved only when 75%–80% of the population are vaccinated.41 The automation of mass vaccination processes will make it possible to quantify the number of people vaccinated in real time. However, one aspect to take into account is that herd immunity would not only depend on vaccination coverage, but also on whether the vaccine has the capability to produce it, a matter that is beyond the scope of the proposed prototype.
Axure RP software was used as the tool to design and build the functional and realistic prototype. The results of the prototype are published on the Internet.28
The prototype starts with the process of vaccination centre selection by the citizen (Fig. 2), which generates a QR code. This QR code is used until vaccination is complete, making it possible for the user to enjoy a simple, innovative experience, thanks to the flexibility of scanning a QR code with the mobile phone's camera. The will prevent the inefficiency of the traditional method of registration and vaccination control on paper.
The dashboard displays the information in real time, given that it is no longer necessary to wait hours, days, or even weeks to promptly have the data from a process of mass vaccination. Fig. 3 shows the prototype's dashboard where the information is displayed in real time. This characteristic of being able to have real-time data available allows for decision making and continuous improvement of the mass vaccination process; i.e., data-based decision making.
Limitations of the prototype
This proposal requires that both citizens and healthcare workers have a mobile smartphone or tablet with Internet access in order to keep data updated in real time. According to INEI42 [regarding] the digital divide in Peru in the fourth quarter of 2020 [revealed that] 87.7% of the population using the Internet does so via a mobile phone. By area of residence, 88.8% of the user population aged 6 and over resides in Metropolitan Lima and accesses the Internet via mobile phone, 87.1% in the Remaining of Urban Area, and 86.5% in the Rural Area. However, the lack of such equipment or services, which generally occurs in rural areas where there is no access to land-based mobile telephony services, should not be a limiting factor for the use of the proposed solution, given that it could be used under the following considerations: first, in the case of the citizen, registration modules with satellite Internet access could be installed, staffed by local or regional government support personnel, so that appointments and the respective QR code printed on paper can be generated by these modules; second, in the case of healthcare personnel, satellite Internet access could be used to control and register the vaccination, as well as to scan the QR codes printed on paper.
Future studiesThe prototype presented has not included a common feature of vaccination systems, the voluntariness of the citizen in that the vaccine is not imposed on anyone.43 Doubts about the effectiveness of vaccines are a major challenge that will place an additional burden on the immunisation programme,44 given the need to neutralise the false news against vaccines circulating on social networks, which is creating rejection and mistrust in the population. Consequently, efforts to have vaccination centres adequately sized in terms of demand, capacity, and real-time information will be wasted if citizens do not attend. This situation is left to the reader as future studies to address the perceived risks, hesitation, and communication crises that should be addressed in all mass vaccination programmes.
It has been pointed out that the strength of the prototype lies in the centralised database specifically for the vaccination programme (Fig. 1), however, we cannot ignore the fact that there are other sources of health data which are not integrated because of the lack of systematic frameworks and tools, making their integration to promote interoperability a challenge,45 giving rise to the information silos mentioned above. This scenario raises the need for new, future studies to design technological architectures aimed at creating a patient health record by integrating different sources of health data, so that data can be accessed for consultation from any legal healthcare setting. This would be useful for vaccination programmes, health professionals, patients, and their families to understand how and why a critical medical decision or recommendation was made or recommended.46
ConclusionsManual processes are known to be inefficient, error-prone, and to generate unnecessary costs, not only in terms of human resources, but also in terms of the logistical resources involved. Facing the current situation of the COVID-19 pandemic, specifically in the vaccination processes performed at vaccination centres, calls for streamlined appointment and registration processes, entry control, and real-time availability of information related to the vaccination process.
The proposal of this project aims to achieve this efficiency by using mobile phone technology in daily use in the population with Cloud Computing technology and the QR code. The results of the prototype are yielding promising results that will enable efficiency, control of the vaccination process at the vaccination centres, and real-time monitoring thanks to the strength of having a centralised, digital database, not only because it is updated in real time during the vaccination centre process, but also because it will complement the data for processes other than the ones at the vaccination centres and can be used by different applications to display other types of information with these data or exploit them through artificial intelligence techniques to generate predictive models.
However, there are other variables such as the citizen's willingness to be vaccinated or the ethics in the treatment of their data that guarantee confidentiality that have not been addressed, at least in this first version of the prototype.
FundingThis study has not received any specific support from public sector agencies, the commercial sector, or non-profit organisations.
Please cite this article as: Rodas-Martinez AK, Altamirano-Yupanqui JR. Vacunaciones masivas contra el COVID-19 mediante el uso de las tecnologías para la gestión de la programación de citas y de datos de grandes volúmenes de vacunados. Vacunas. 2022. https://doi.org/10.1016/j.vacun.2022.07.003